
Parisa Taheri Tanjani ( Safety Promotion and Injury Prevention Research Center, Department of Internal Medicine Ayatollah Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. )
Samaneh Akbarpour ( Tehran University of Medical Sciences, Tehran, Iran. )
Elaheh Ainy ( Safety Promotion and Injury Prevention Research Center, Department of Internal Medicine Ayatollah Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. )
Hamid Soori ( Safety Promotion and Injury Prevention Research Center, Department of Internal Medicine Ayatollah Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. )
October 2015, Volume 65, Issue 10
Original Article
Abstract
Objective: To examine self-reported mobility and limitation in physical functioning among the elderly and associated socio-demographic risk factors.
Methods: The population-based cross-sectional study was conducted from January 2012 to January 2013 and comprised subjects from five provinces of Iran. The variables were measured using a questionnaire. Self-reported mobility disability and physical functioning disability were defined as having no problems in daily activities and physical tasks. Logistic regression was used to calculate the odds ratio for association of socio-demographic risk factors and outcomes.
Results: Of the 1325 subjects, 636(48%) were men. The overall mean age was 69.14±7.37 years. Prevalence of mobility disability and limitation in physical functioning was 401(63%) and 553(87%) in men, and 524(76%) and 641(93%) in women. There was a significant association between mobility disability and family composition and satisfaction with financial situation and housing tenure in both genders (p<0.05 each). Physical functioning had a significant relationship with family composition, and satisfaction with financial situations and housing tenure in men and women and population density in men and marital status in women (p<0.05 each).
Conclusion: The elderly had a high risk of disability. Social factors had more association with mobility disability and limitation in physical functioning and required specific social support.
Keywords: Elderly, Older population, Physical functioning, Mobility disability. (JPMA 65: 1060; 2015).
Introduction
The number of old people has increased in low, middle and high-income countries as a result of increase in life expectancy,1,2 According to the World Health Organisation\'s (WHO) definition, people over 60 years of age in low and middle-income countries are called elderly.3 Mobility, which is the ability to move without assistance, is an important part of physical functioning. It is necessary for doing everyday tasks and having an independent life.4,5 Mobility impairment increases with age. A majority of the elderly experience a decline in mobility, which impacts their quality of life and dependence on healthcare system.6-8 Many of these changes lead to decreased muscle strength and balance, which are important for the development of functional ability.9
Mobility disability, limitation in physical functioning, and falling are major health issues among the elderly. WHO has reported that about 20% of people over 70 years and 50% older than 85 years have some kind of mobility disability.10,11 About 7.3% of Iranian population was above 60 years old in 2005. However, according to the estimation of World Population Ageing, United Nations, it will increase to 11.6% in 2025 and 30.8% in 2050.12,13
No national studies have been conducted on mobility disability and limitation in physical functioning in the elderly in Iran. Considering the aging population and limited information about this issue, the current study was planned as the first one at the national level. It was planned to examine self-reported mobility, limitation in physical functioning, and socio-demographic risk factors in older people.14
Subjects and Methods
The population-based cross-sectional study at the national level was carried out in Iran from January 2012 to January 2013, and comprised people over age 60 of either gender. The subjects were randomly selected in three phases, based on proportion of population from 5 provinces (Alborz, North Khorasan, West Azerbaijan, Sistan & Baluchestan, and Hormozgan), using stratified sampling. In the second phase, 66 cities were randomly selected from the 5 provinces. In the third phase, 109 healthcare centres were selected using cluster sampling. After taking consent form the subjects, data was collected using a valid and reliable questionnaire.
Mobility disability was measured by the mobility-help scale, by asking the participants whether they had difficulty with any of their daily activities, including bathing, going to toilet, cooking, shopping, doing domestic chores (cleaning home), transferring, using the phone, and dressing. A binary variable was constructed to indicate the mobility disability in any of these activities. Mobility disability was defined as having no problems based on the daily activities.
Limitation in physical functioning was calculated in the same way by asking the participants about the following tasks: difficulty in severe activity (pushing tables, running, lifting, weighing), difficulty in moderate activity (vacuuming, replacing desks), difficulty in walking more than 100m, difficulty in climbing one flight of stairs, and difficulty in climbing more than one flight of stairs. Limitations in physical functioning were defined as having no problems in doing daily tasks.
Data was analysed separately from men and women, using SPSS 17. Distribution of socio-demographic characteristics, mobility disability, and limitation in physical functioning were presented as mean values for numerical variables and frequencies and percentage for categorical variables. Baseline characteristic differences between men and women were determined by Chi-square test for categorical variables, and student t-test for continuous variables. Association of socio-demographic and outcomes was investigated by logistic regression analysis.
Results
Of the 1325 subjects, 636(48%) were men and 689(52%) were women. The overall mean age was 69.14±7.37 years. Overall, 708(53%) participants were living in urban areas, and 868(65.6%) were illiterate (Table-1).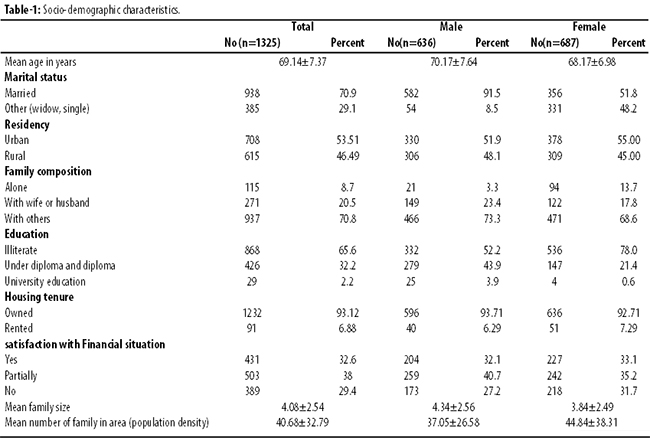
Prevalence of mobility disability and limitation in physical functioning was 401(63%) and 553(87%) in men, and 524(76%) and 641(93%) in women (Table-2).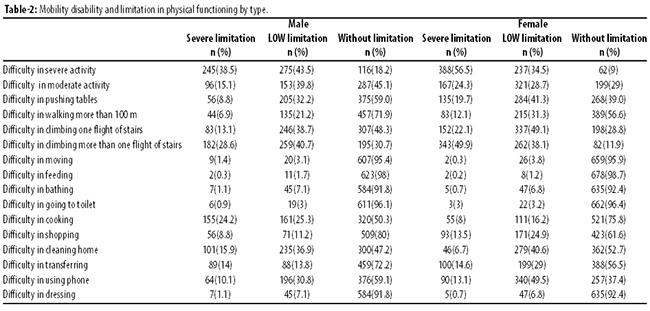
There was a significant association between mobility disability and family composition and satisfaction with financial situation and housing tenure in both genders (p<0.05 each). Physical functioning had a significant relationship with family composition, and satisfaction with financial situations and housing tenure in men and women and population density in men and marital status in women (p<0.05 each) (Table-3).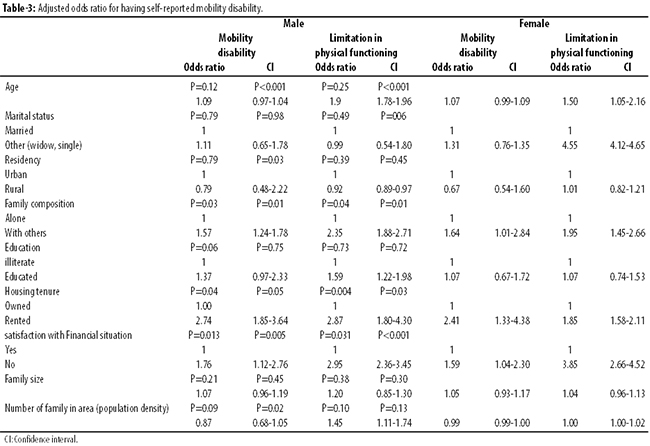
Discussion
The study aimed at describing the pattern of self-reported mobility disability and limitation in physical functioning, and their association with socio-demographic risk factors among the elderly in Iran. As a country, Iran has diversified socio-demographic factors and it was expected that these factors would be related to the kind of disability and limitations in the target population. Self-report assessment was applied for evaluating the type of disability as a traditional method to examine mobility and functional ability.14 Although some researchers believe that self-reported measurements for mobility and physical measurement are less reliable than objective tests,15 but they are practical methods in large samples, and have been widely used in a large number of population-based works. To the best of our knowledge, there have been no works about mobility disability in the elderly in Iran. Most previous studies have focused on depression and nutrition.15,16 This study was the first national work on evaluating the issue.
Mobility disability and limitation among older people are key health markers of the elderly. These are often neglected in developing countries. Here, attempts were made to evaluate a random and representative sample of the elderly, and demonstrate the overall pattern of mobility disability in Iran. According to the obtained results, the highest prevalence of difficulties in physical functioning markers was difficulty in severe activity in women and men. Other studies have also reported the same results.17
Our results showed that the overall prevalence of mobility disability was very high. Some studies have indicated lower prevalence in other countries.18 More frequent prevalence of mobility disability in Iran demonstrated that the elderly had a great risk of disability.
Based on the findings of this study, women experienced more disability than men, which was consistent with the results of other studies.19
The highest percentage of difficulties in disability markers was found in cleaning homes in men and using phones in women. This can be related to the point that Iranian men were less likely to cook; even young men. Difficulty in using phones was high among women as well as men. It can be related to hearing loss which increases with age. Majority of the elderly people experience a decline in hearing.
Mobility disability and limitation in physical functioning were found to be correlated with some socio-demographic risk factors. Our results showed that family composition and satisfaction with financial situation, and housing tenure could increase the odds ratio for two outcomes in both the genders. Satisfaction with financial situation had the strongest association in all the regression models as well.
A Brazilian study has reported that education in women and income in men were the strongest risk factors for disability among socio-demographic risk factors.21 Here, no significant association was found between education and outcomes. This different effect can be related to the lack of education diversity among the elderly in Iran.
There were some limitations in the present study. First, it was based on a single questionnaire. Also, all the variables were self-reported and no variable was measured by the researchers. Second, this study was cross-sectional. Therefore, explanation of the causality was challenging. However, there were some strong points. This study was the first population-based and national study among the elderly, with a representative sample in Iran. Socio-demographic index was important in influencing mobility disability in the elderly. It has rarely been reported in previous works.17
Results showed that the social factors (family composition and satisfaction with financial situation and housing tenure) were more associated with interesting outcomes. These factors may increase the need for social support. These findings suggested that interventions aimed at improving social support in the elderly may decrease disability.
Conclusions
The overall prevalence of mobility disability and limitation in physical functioning were very high among the elderly in Iran. Social factors have more association with mobility disability, and limitation in physical functioning. Thus, the elderly need special social support. More studies are recommended to substantiate the findings.
Acknowledgements
We are grateful to the Safety Promotion and Injury Prevention Research Centre of Shahid Beheshti University of Medical Sciences for advice and guidance.
References
1. Maia FOM, Duarte YAO, Lebrao ML, Santos JLF. Risk factors for mortality among elderly people. Rev Saude Publica 2006; 40: 1-7.
2. Definition of an older or elderly person. Proposed working Definition of an older person in Africa for the MDS project. [online] [cited 2015 March 22]. Available from: URL: http://www.who.int/ healthinfo/ surrvey/ageingdefnolder/en.
3. Mackenbach JP, Borsboom GJ, Nusselder WJ, Looman C, Schrijvers C. Determinants of levels and changes of physical functioning in chronically ill persons: results from the globe study. J Epidemiol Comm Health 2001; 55: 631-8.
4. Spillman BC. Changes in elderly disability rates and the impli-cations for health care utilization and cost. Milbank Q 2004; 82: 157-94.
5. Manton KG, Gu X, Lamb VL. Change in chronic disability from 1982 to 2004/2005 asmeasured by long-termchanges in function and health in the U.S elderly population. Proc Natl Acad Sci 2006; 103: 18374-9.
6. Gill T, Guo Z, Allore H. The epidemiology of bathing disability in older persons. J Am Geriatr Soc 2006; 54: 1524-30.
7. Larry LS. Disability among adults in New York State, 2001-2003. Prevalence and health risk behavior. Behavioral Risk Factor Surveillance System 2005; 12:1-8.
8. American College of Sports Medicine, Chodzko-Zajko WJ, Proctor DN, Fiatarone Singh MA, Minson CT, Nigg CR, Salem GJ, Skinner JS. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med Sci Sports Exerc 2009; 41:1510-30.
9. Delbaere K, Crombez G, Vanderstraeten G, Willems T, Cambier D. Fear-related avoidance of activities, falls and physical frailty. A prospective community-based cohort study. Age Ageing 2004; 33: 368-73.
10. World Health Organization. What are the main risk factors for disability in old age and how can disability be prevented? [online] 2003 [cited 2012 April 26]. Available from: URL: http://www.euro.who.int/document/E82970.pdf.
11. World Health Organization. Disability and rehabilitation WHO action plan 2006-2011. [online] 2006 [cited 2012 April 26]. Available from: URL: http://www.who.int/disabilities/ publications/dar_action_plan_2006to2011.pdf
12. Publications Information Base Statistical Centre of Iran. [online] Cited 2015 March 22. Available from: URL: http://amar.sci.org.ir/
13. Amir-Sadri A, Soleimani H. Elderly phenomena and its outcomes in Iran. Int J Hyg Health 2005; 1: 19-35.
14. Seidel D, Carol B, Carol J. Limitations in physical functioning among older people as a predictor of subsequent disability in instrumental activities of daily living. Age Ageing 2011; 40: 463-9.
15. Melzer I, Kurz I, Sarid O, Jette AM. Relationship between self-reported function and disability and balance performance measures in the elderly. J Rehabil Res Dev 2007; 44: 685-92.
16. Kheirkhah F, Hosseini R, Hosseini F, Ghasemi N, Bijani A. Relationship between testosterone levels and depressive symptoms in older men in Amirkola, Iran, Caspian J Intern Med 2014; 5: 65-70 .
17. Melzer D, Parahyba M. Socio-demographic correlates of mobility disability in older Brazilians: results of the first national survey. Age Ageing 2004; 33: 253-259.
18. Fagerstro C, Persson H, Holst G, Hallberg I. Determinants of feeling hindered by health problems in daily living at 60 years and above. Scand J Caring Sci 2008; 22: 410-21.
19. Mollaog M, Fatma O, Tuncay Z. Mobility disability and life satisfaction in elderly people. Arch Gerontol Geriatr 2010; 51: 115-9.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: