
Muhammad Kamal ( Department of Dermatology, Gazi University School of Medicine, Ankara, Turkey. )
Muhterem Polat ( Department of Dermatology, Gazi University School of Medicine, Ankara, Turkey. )
September 2015, Volume 65, Issue 9
Original Article
Abstract
Objective: To investigate the effects of different doses of isotretinoin on serum homocysteine, vitamin B12 and folic acid in patients with acne vulgaris.
Methods: The case-control study was conducted at Gazi University School of Medicine, Ankara, Turkey, from November 2012 to March 2013, and comprised male or non-pregnant female patients more than 18 years of age. The cases had moderate to severe nodulocystic acne, while an equal and matching control group had healthy individuals. Isotretinoin was started in a dosage of 0.5 mg/kg/day, and 1.0 mg/kg/day in patients with medium and severe acne vulgaris respectively. Homocysteine, vitamin B12, folic acid, liver function tests, serum cholesterol and triglyceride levels were tested at the baseline and on day 45. SPSS 11 was used for statistical analysis.
Results: The two groups had 62 subjects each. The cases had 47(76%) women and 15(25%) men with a group mean age of 21.0±2.7 years. The controls had 45(72.6%) women and 17(27.4%) men with a group mean age of 21.6±3.0 years. Homocysteine levels were significantly increased in both groups taking 0.5 mg/kg/day and 1.0 mg/kg/day isotretinoin (p<0.05). There were no statistically significant differences in the levels of vitamin B12, folate and liver function tests (p>0.05 each). Total cholesterol level increased significantly in the group using 1.0 mg/kg/day (p<0.05). In the triglyceride levels, significant increases were seen in both groups (p<0.05).
Conclusion: Evaluation of homocysteine, vitamin B12 and folic acid beside the routine tests were beneficial for the patients before they started isotretinoin treatment.
Keywords: Isotretinoin, Acne, Homocysteine, Vitamin B12, Folic acid. (JPMA 65: 950; 2015).
Introduction
Oral isotretinoin (Iso) is a highly effective treatment agent for patients with nodulocystic acne and moderate to severe acne resistant to conventional therapy. It affects all major aetiological factors involved in the pathogenesis of acne vulgaris (AV).1 In addition to a variety of clinical side-effects, Iso may cause dyslipidaemia, increased liver enzymes, and reduction of biotinidase activity.2 There are studies indicating elevation in homocysteine(Hcy) levels after treatment with Iso.3-6
Iso may also affect cystathionine-b-synthase which is the responsible enzyme for Hcy metabolism, and may cause hyperhomocysteinaemia. Hcyis recycled into methionine by a transmethylation reaction requiring vitamin B12 and folate. Both vitamin B12 and folic acid are also required as cofactors for the enzyme Hcymethyltransferase, and any deficiency in these vitamins results in hyperhomocysteinaemia.7,8 There are several studies reporting that elevated plasma Hcy concentrations are associated with an increased risk of premature occlusive vascular diseases.9-12
The current study was planned to investigate the effect of different doses of Iso on serum Hcy, vitamin B12 and folic acid in patients with AV.
Patients and Methods
The case-control study was conducted at Gazi University School of Medicine, Ankara, Turkey, from November 2012 to March 2013, and comprised male or non-pregnant female patients more than 18 years of age. The cases had moderate and severe nodulocystic acne (31 patients in each sub group), while an equal and matching control group had healthy individuals. Patients using any vitamin A supplements or any other medications, patients having history of previous therapy with oral retinoids, and of diseases known to affect vitamin B 12 and/or folic acid metabolism were excluded from the study. After obtaining approval from the institutional ethics committee and informed written consent from the subjects, Iso therapy was initiated at the dose of 0.5 mg/kg/day in cases of moderate AV, and 1.0 mg/kg/day in severe AV. The cases completed the treatment that lasted at least five months. Before the initiation of the therapy, laboratory screening was done and it included serum glutamic-oxaloacetic transaminase (SGOT), serum glutamic-pyruvic transaminase (SGPT), alkaline phosphatase (ALP), gamma glutamyltransferase (GGT), cholesterol, triglycerides, folic acid, vitamin B12, and Hcy. The same tests were repeated on the 45th day of the treatment. Folic acid, vitamin B12, and Hcy were tested only once in the control group.
Fasting blood samples were obtained by venipuncture of the large antecubital veins of patients without stasis and after a 12-hour fasting. The samples were centrifuged and the plasma was separated and stored at -80°C. In order to avoid variation, all samples were studied on the same day and by using the same kit. Vitamin B12 and folic acid levels were determined by the electro-chemiluminescenceimmunoassay (ELICA). Hcy levels were determined by axis Hcyenzyme immunoassay method.
Statistical analyses were done using SPSS 11.5. P<0.05 was considered statistically significant. Distributions of variables were analysed by Kolmogorov-Smirnov test. The significance of differences as mean values and median values between the groups were analysed by using Student\'s t test and Mann Whitney U test respectively. Pearson\'s chi-square test was used for the evaluation of nominal variables. The significance of differences in the laboratory data before and after the treatment in groups was assessed by Wilcoxon signed rank test. Spearman\'s correlation test was used to determine the correlation of variables.
Results
The two groups had 62 subjects each. The cases had 47(76%) women and 15(25%) men with a group mean age of 21.0±2.7 years. The controls had 45(72.6%) women and 17(27.4%) men with a group mean age of 21.6±3.0 years. There was no statistically significant difference in terms of gender (p=0.681) and age (p=0.305) in the two groups. The differences between the baseline values of Hcy, vitamin B12 and folic acid were not statistically significant between the groups (p>0.05 each).Within the cases, plasma Hcy levels were statistically increased after treatment (0.5 mg/kg/day and 1.0 mg/kg/day) compared to the baseline values and the control group, but there was no statistically significant difference in vitamin B12 and folic acid levels (Table-1).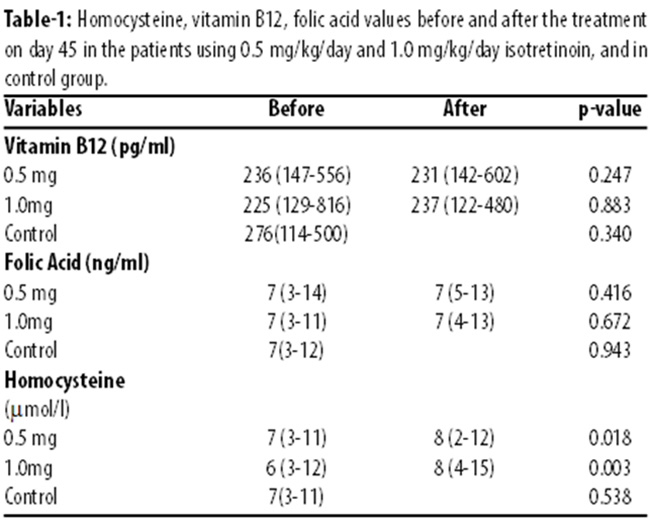
No statistically significant differences were found in the levels of SGOT, SGPT, ALP and GGT tested before and after the treatment in the patient groups using 0.5mg/kg/day and 1.0 mg/kg/day Iso when compared with baseline values (p>0.05 each).The total cholesterol levels increased significantly in the group using 1.0 mg/kg/day Iso after the treatment (p<0.05). In the sub-group using 0.5 mg/kg/day Iso, however, no significant increases were observed (p>0.05). Triglyceride levels saw statistically significant increase in both sub-groups after the treatment (Table-2).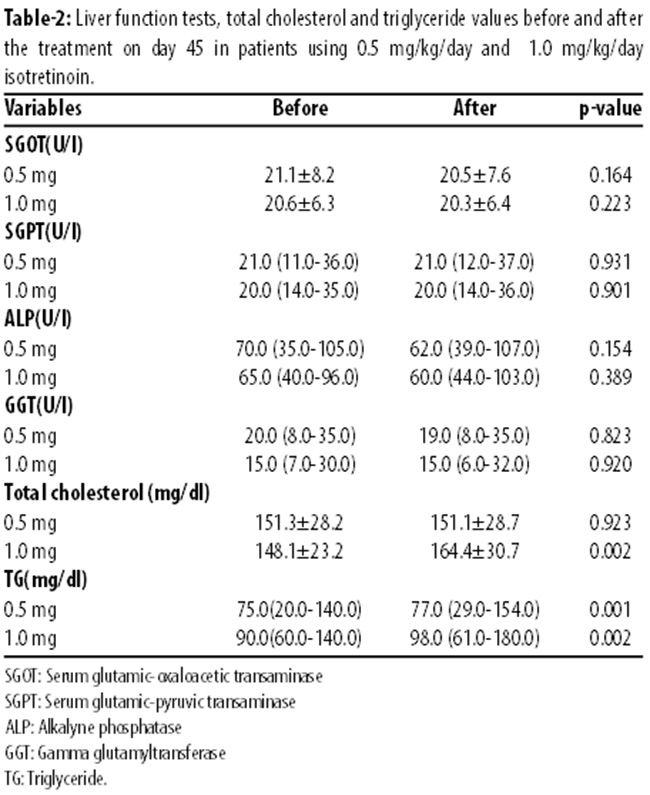
Discussion
Our study was in continuation of several studies on the effect of Iso on Hcy levels. The first such study3 evaluated plasma Hcy levels in 28 patients on Iso therapy (0.5 mg/kg/24 h) for nodulocystic acne, and found that plasma levels of Hcy, serum triglycerides, cholesterol, very low-density lipoprotein (VLDL), and low-density lipoprotein (LDL) were elevated after 45th day of the treatment. However, there was no significant change in vitamin B12 and folate levels. In another study4 comprising 74 patients on Iso therapy (0.5 mg/kg/24h) with nodulocystic acne, plasma Hcy, liver enzymes, triglycerides, cholesterol, LDL, and VLDL levels increased after treatment,but there were no change in vitamin B12 and folate levels. In a similar study5 that had 47 patients with moderate or severe acne receiving Iso (0.5 mg/kg/24h), Hcy levels increased, folate and vitamin B12 did not change significantly. Besides liver enzymes, serum triglycerides cholesterol, VLDL, LDL were elevated. Another study published in recent years6 that had 66 patients found that folic acid and vitamin B12 levels decreased, whereas Hcy levels increased at the end of 4 months of Iso therapy (0.5-0.75 mg/kg/24h). It also found that LDL, VLDL, SGOT and SGPT levels increased after the treatment. The first 3 studies3-5 concluded that elevation of Hcy levels despite the normal values of responsible vitamins for the metabolism of amino acid strongly suggested that cystathionine-b-synthase might be affected by the drug, acting as an inhibitor of the enzyme or the liver dysfunction caused by Iso. A recent study6 showed decrease in folate and vitamin B12 levels after 4 months of treatment and mentioned that longer treatment with higher cumulative doses of Iso might have caused subclinical vitamin B12 and folic acid deficiencies to have more effect on Hcy levels.
To our knowledge, our study is the first to evaluate the effect of different doses of Iso (0.5 mg/kg/day and 1.0 mg/kg/day) on serum Hcy, vitamin B12 and folic acid in patients with AV. In the present study, plasma Hcy levels were statistically increased after treatment in both 0.5 mg/kg/day and 1.0 mg/kg/day groups. In order to say that less dosages of Iso also cause an elevation in Hcy levels, further studies with less Iso doses should be carried out. There was no statistically significant difference in vitamin B12 and folic acid levels after the treatment. These results were similar with the previous 3 studies.3-5 Onlyone study6 showed decreased vitamin B12 and folic acid levels after the treatment. According to the study, longer treatment with higher cumulative doses of Iso might have caused subclinical vitamin B12 and folic acid deficiencies. In contrast with previous studies, we found no significant increase in liver enzymes. The result supports the notion that elevation of Hcy levels might be due to the drug impact on the enzyme cystathionine-b-synthase without liver dysfunction. Total cholesterol levels increased significantly in the group using 1.0 mg/kg/day Iso after treatment. In the group using 0.5 mg/kg/day Iso, however, no significant increases were observed. Therefore the dosage of Iso might be important in the elevation of serum cholesterol levels and there may be a relationship between the doses of Iso and serum cholesterol levels. In the triglyceride levels, statistically significant increases were seen in both sub-groups after the treatment. It can be said that triglyceride levels increase both in less and higher doses of Iso usage. The effect of Iso on triglycerides is a well-known side effect of the drug.2 A study including 13,772 patients reported that triglyceride levels were elevated in 44% patients on Iso treatment and it was the most common laboratory abnormality.13 It has been reported in many studies that hyperhomocysteinaemia is a risk factor for coronary heart disease and is associated with endothelial damage and oxidative stres.10,13-16 The elevated levels in addition to hyperhomocysteinaemia could be associated with an increased risk of premature occlusive vascular disease in patients on Iso therapy.4,6 A study about the importance of folic acid and vitamin B12 in reduction of risk of vascular disease found that supplementing with both provides a more certain way to improve Hcy levels.17 It would be helpful if the levels of vitamin B12 and folic acids are known and supply in the case of deficiency.
Conclusion
Whatever the dosage of prescribed Iso, follow-up of the levels of Hcy as well as liver enzymes, cholesterol and triglycerides will be beneficial for the patients. Patients should also be tested for vitamin B12 and folate levels. All these precautions need to be taken in order to prevent hyperhomocysteinaemia and associated complications.
References
1. Mills C, Marks R. Adverse reactions to oral retinoids. Drug safety. 1993:9:280-9.
2. Schulpis KH, Georgala S, Papakonstantinou ED, Karikas GA. The effect of isotretinoin on biotidinase activity. Skin Pharmacol. 1999: 12:28-33.
3. Schulpis KH, Karikas GA, Georgala S, Michas T, Tsakiris S. Elevated plasma homocysteine levels in patients on isitretinoin therapy for cystic acne. Int J dermatol. 2001: 40:33-6.
4. Polat M, Lenk N, Bingöl S, Özta? P, ?lhan MN, Artüz F, et al. Plasma homocysteine level is elevated in patients on isotretinoin therapy for cystic acne: A prospective controlled study. J Dermatolog Treat. 2008:19:229-32.
5. Roodsari MR, Akbari MR, Sarrafi-rad N, Saeedi M, Gheisari M, Kavand S. The effect of isotretinoin treatment on plasma homocysteine levels in acne vulgaris. Clin Exp dermatol. 2010:35:624-6.
6. Karadag AS, Tutal E, Ertu?rul DT, Akin KO. Effect of isotretinoin treatment on plasma holotranscobalamin, vitamin B12, folic acid, and homocysteine levels: non-controlled study. Int J Dermatol 2011: 50:1564-9.
7. Amichai B, Grunwald MH. Isotretinoinin dermatology. J Dermatol treat 2000:11:219-40.
8. Guttormsen AB, Schneede J, Ueland PM, Refsum H. Kinetics of plasma homocysteinein subjects with hyperhomocysteinemia due to folic acid or cobalamin deficiency. Am J ClinNutr. 1996:63:194-202.
9. Malinow MR, Kang SS, Taylor LM, Wong PW. Prevalence in hyperhomocysteinemiain patients with peripheral arterial occlusive disease. Circulation. 1989: 79:1180-8.
10. PerrtIJ, Refsum H, Morris RW, Ebrahim SB, Ueland PM, Shaper AG. Prospective study of serum total homocysteine concentration and risk of stroke in middle-aged British men. Lancet. 1995: 346:1395-8.
11. Pancharuniti N, Lewis CA, Sauberlich HE, Perkins LL, Go RC, Alvarez JO, et al. Plasma homocysteine, folate and vitamin B12 concentrations and risk of early-onset coronary artery disease. Am J ClinNutr. 1994: 59:940-8.
12. Schneyder G, Roffi M, Flammer Y, Pin R, Hess OM. Effect of homocysteine-lowering therapy with folic acid, vitamin B12, and vitamin B6 on clinical outcome after percutaneous coronary intervention. The Swiss Heart Study: A randomized controlled trial. JAMA. 2002:288:973-9.
13. Zane LT, Leyden WA, Marqueling AL, Manos MM. A population-based analysis of laboratory abnormalities during isotretinoin therapy for acne vulgaris. Arch Dermatol. 2006: 142:1016-22.
14. Mayer EL, Jacobsen DW, Robinson K. Homocysteine and coronary atherosclerosis. J Am Coll Cardiol. 1996: 27:517-27.
15. Verhoef P, Kok FJ, Kruyssen DA, Schouten EG, Witteman JC, Grobbee DE, et al. Plasma total homocysteine, B vitamins, and risk of coronary atherosclerosis. Arterioscler Thromb Vasc Biol. 1997:17:989-95.
16. Langman LJ, Ray JG, Evrovski J, Yeo E, Cole DE. Hyperhomocysteinemia and the increased risk of venous thromboembolism: More evidence from a case-control study. Arch Intern Med 2000: 160:961-4.
17. Quinlivan EP, McPartlin J, McNulty H, Ward M, Strain JJ, Weir DG, et al. Importance of both folic acid and vitamin B12 in reduction of risk of vascular disease. Lancet 2002: 359:227-8.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: