
Naseema Mehboobali ( Department of Community Health Sciences, Aga Khan University, Pakistan. )
Saleem Perwaiz Iqbal ( Department of Biological and Biomedical Sciences, Aga Khan University, Pakistan. )
Mohammad Perwaiz Iqbal ( Department of Community Health Sciences, Aga Khan University, Pakistan. )
September 2015, Volume 65, Issue 9
Original Article
Abstract
Objective: To determine the frequency of vitamin D deficiency and insufficiency in a low-income peri-urban population.
Methods: The cross-sectional study was conducted in a low-income, unplanned settlement in Karachi, and comprised apparently healthy adults who were recruited randomly with informed consent. Serum levels of 25-hydroxy vitamin D were measured using a kit obtained from Roche Diagnostics. One-way analysis of variance and logistic regression were used for statistical analysis.
Results: Of the 858 subjects, 507(59%) were females and 351(41%) males (age range: 18-60 years). Prevalence estimates of vitamin D deficiency (<20ng/ml) and insufficiency (20.0-29.9ng/ml) were found to be 501(58.4%) and 269(31.4%), respectively. Odds ratio of vitamin D deficiency was significantly higher in females compared to males after adjusting for education and smoking status (p=0.001).
Conclusion: High prevalence of vitamin D deficiency among females in one of the peri-urban areas points towards a public health problem which requires attention of the medical community.
Keywords: Vitamin D deficiency, Urban population, Socioeconomic factors. (JPMA 65: 946; 2015).
Introduction
Hypovitaminosis D is a worldwide health problem.1 Its deficiency is defined as serum levels of 25-hydroxy vitamin D (25[OH]D)) less than 20ng/ml, while those having serum levels of 25(OH)D in the range 20-29.9ng/ml fall into the category of vitamin D insufficiency.1,2
Vitamin D deficiency has reached epidemic proportions in South Asia, especially in Pakistan where deficiency could be in the range of (70%-92%).3-6 Most of these reports pertain to ambulatory patients visiting hospitals or clinics with various illnesses.4,5 A study reported serum levels of 25(OH)D in adults from 10 different localities in Karachi and showed an overall prevalence of vitamin D deficiency to be 74%.7 However, these individuals were referred by their physicians to have their vitamin D levels assessed. To the best of our knowledge, no systematic large-scale study has been carried out to ascertain the prevalence of vitamin D deficiency or insufficiency in an apparently healthy general population in Pakistan. We planned the current study to determine the frequency of vitamin D deficiency and insufficiency in a low-income peri-urban population in Karachi.
Subjects and Methods
The nested study was conducted from a cohort of 926 healthy subjects enrolled from the low-income, unplanned settlement in Sultanabad area in eastern Karachi to find out the prevalence of deficiencies of folate, vitamin B6 and vitamin B12.8 For the parent study (February 2006 to March 2007), a sampling frame of 4000 houses was available in this locality of a population of about 53,000 subjects,9 and systematic random sampling was carried out to select houses and subsequently individuals from these houses as described in a previous publication.10
For the nested study (September 2009 to October 2010), 858 healthy adults were included who had no acute or chronic illness, were non-pregnant, and were not taking vitamin D supplements for the preceding 6 months The study was approved by the Ethics Review Committee of the Aga Khan University, Karachi, and informed consent was obtained from all the participants.
Demographic characteristics, education, house-hold income and smoking statuses were determined through a questionnaire. Blood sampling was done in fasting state and serum levels of 25(OH) D were measured using a commercially available kit based on electrochemiluminescence immunoassay (Elecsys; Roche Diagnostics, Indianapolis) at the Laboratory of Roche Pakistan Limited, Karachi. Vitamin D deficiency was defined as <20ng/ml, while insufficiency was defined as 20.0-29.9ng/ml.1,2 Quantitative values were expressed as means ± standard deviation and were compared using one-way analysis of variance (ANOVA0 followed by Tukey's HSD test for multiple pair-wise comparisons. Logistic regression was used to assess the relationship of gender with the odds of having vitamin D deficiency in this population. P<0.05 was considered significant.
Results
Of the 858 subjects, 507(51%) were females and 351(49%) males with an overall mean age of 32.5±10.7 years (range: 18-60 years). The mean age of males was 32.1±11.5 years and that of females was 32.8±10.1 years and the difference was not significant (p=0.32) (Table).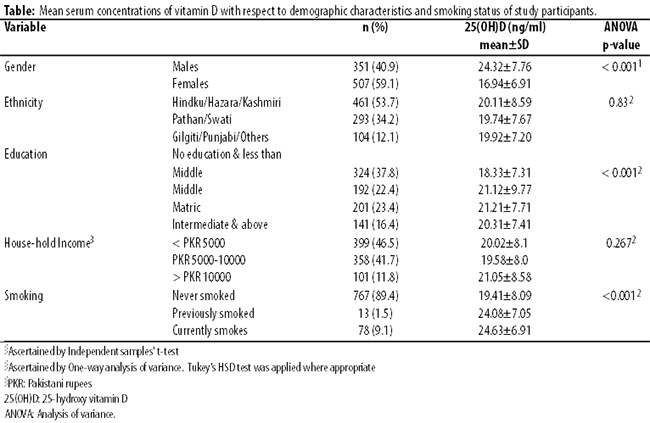
Mean serum 25(OH) D concentration in females was significantly lower compared to males (p<0.001), while no significant differences were observed in mean concentration values of 25(OH) D among various ethnic groups and groups with different house-hold income (p=0.83; p=0.267). Mean serum concentration of 25(OH) D was significantly lower in the group of individuals with formal education less than middle class compared to other groups with education higher than that level (p<0.001). Similarly, mean 25(OH) D levels among non-smokers were significantly lower compared to current and previous smokers (p<0.001). A further analysis of smoking status of subjects revealed that low mean serum level of 25(OH) D among non-smokers was primarily due to very high proportion of females in this group. Frequency distribution of vitamin D deficiency in males and females was found to be 115(33%) and 386(76%), respectively, while frequency distribution of vitamin D insufficiency in males and females was 165(47%) and 104(21%), respectively. Overall, prevalence estimates of vitamin D deficiency and insufficiency in this population were 501(58.4%) and 269(31.4%), respectively. Overall, 281(80%) males and 492(97%) females were vitamin D deficient/insufficient. A logistic regression model employed to evaluate the relationship between vitamin D deficiency and gender indicated that the odds ratio (OR) of vitamin D deficiency in females was 6.69 compared to males after adjusting for education and smoking status [OR (95% Confidence Interval [CI])=6.69 (4.63-9.67); p=0.001]. For determining if the addition of education and smoking status improved the calibration of the model, the Hosmer-Lemeshow Goodness of Fit test was performed which was found to be insignificant, indicating a good fit of the adjusted model (X2=3.579; df=6; p=0.733).
Discussion
Our study found very high prevalence of vitamin D deficiency and insufficiency in Pakistani female population which is consistent with reported values of vitamin D insufficiency/deficiency in a few earlier studies carried out in Pakistan.3-7 One reported vitamin D insufficiency/deficiency to be 95.5% in patients (n=600) presenting themselves at various clinics in Islamabad with some ailment,4 while our study is unique in terms of reporting prevalence of vitamin D deficiency and insufficiency in healthy general population in Karachi. Another study reported 94.3% insufficiency/deficiency of vitamin D among apparently healthy adult females in Karachi,3 but the sample size was small compared to the present study (n=123 vs. n=858). A study in Islamabad comprised 737 subjects.11 However, the selection of subjects was not through randomisation, while in our study we employed systematic random sampling strategy to select our subjects, thus making our estimates more robust and generalisable.10 Similarly, another study had a large sample size (n=4, 788),7 but almost all the individuals appeared to have been referred by their physicians for assessment of vitamin D status for a problem and, as such, they cannot be considered healthy individuals, while all subjects in the present study were from the community and were not suffering from any chronic or acute disease.
In a recent study on Bahraini mothers, high prevalence of vitamin D deficiency was observed in those with no primary education compared to those with education.12 In another study carried out in Karachi, 7 out of 11 vitamin D deficient pregnant women were found to be uneducated, indicating higher proportion of vitamin D deficiency among uneducated women in that cohort.13 A similar trend has been reported in Finnish population, where higher education was found to be associated with higher serum levels of vitamin D compared to those with less than 7 years of education.14 These reports point towards the notion that educated people are more likely to be aware of the significance of vitamin D sufficiency for good health. This is also suggestive of an association of vitamin D sufficiency or insufficiency with socio-economic status of the population. Although we did observe some association of lack of formal education and education below middle level with low serum levels of vitamin D, yet we did not find any association of household income with serum levels of vitamin D in the present cohort. Perhaps, all the subjects in the present study belonged to the lower socio-economic strata and, therefore, any impact of household income on vitamin D status could have been masked.
High OR (6.69) of vitamin D deficiency among females in this cohort compared to the males is indicative of the vulnerability of our female population, especially those belonging to the lower socio-economic group towards developing vitamin D deficiency. Consumption of food low in vitamin D, multiparity, air pollution preventing ultraviolet (UV) rays' penetration into the skin, avoidance of exposure to sunlight due to concern of tanning (darker skin) and living in houses with limited open spaces could be some of the factors contributing to low serum levels of vitamin D in female population in Karachi settlements.15 It is incumbent upon public health professionals to be proactive in terms of creating awareness among the masses towards avoiding vitamin D deficiency by adopting healthy lifestyle and consuming vitamin D fortified food.
The study was not without limitations. Due to limited resources, we did not measure serum levels of parathyroid hormone which would be expected to be high at such low serum levels of vitamin D. Mean age of the study population was 32.5±10.7 which is quite wide and might have confounded some of the results. Moreover, we also did not determine the daily exposure of subjects to sunlight. Future studies need to address these limitations to better quantify vitamin deficiency/insufficiency burden. Despite these limitations, it is, perhaps, the largest community-based study carried out in Pakistan on vitamin D status of its healthy adult population.
Conclusion
High prevalence of vitamin D deficiency among females in one of the peri-urban areas in Karachi points towards a public health problem that requires attention of the medical community and policy-makers.
Acknowledgement
We are grateful to Dr. Mohsin Yakub for assistance in recruitment of subjects and collection of blood samples; to Roche Pakistan Limited, Karachi, for facilitating the analysis of vitamin D on Elecsys 411; to Mr Iqbal Azam, Assistant Professor, Aga Khan University, for facilitating the post-hoc power analysis using OpenEpi version 3; and to Pakistan Science Foundation which partly the study through a grant to one of the authors..
References
1. Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357: 266-81.
2. Dawson-Hughes B, Heaney RP, Holick MF, Lips P, Meunier PJ, Vieth R. Estimates of optimal vitamin D status. Osteoporos Int. 2005; 16: 13-16.
3. Mansoor S, Habib A, Ghani F, Fatmi Z, Badruddin S, Mansoor S,et al. Prevalence and significance of vitamin D deficiency and insufficiency among apparently healthy adults. Clin Biochem. 2010; 43: 1431-5.
4. Masood Z, Mahmood Q, Ashraf KT. Vitamin D deficiency - an emerging public health problem in Pakistan. Journal of University Medical & Dental College, Faisalabad. 2010; 1:4-9.
5. Zuberi LM, Habib A, Haque N, Jabbar A. Vitamin D deficiency in ambulatory patients. J Pak Med Assoc 2008; 58: 482-4.
6. Khan AH, Iqbal R, Naureen G, Dar FJ, Ahmed FN. Prevalence of vitamin D deficiency and its correlates: results of a community-based study conducted in Karachi, Pakistan. Arch Osteoporos. 2012; 7: 275-82.
7. Iqbal R, Jafri L, Haroon A, Khan AH. Illuminating the dark side-vitamin D status in different localities of Karachi. J Coll Physicians Surg Pak 2013; 23: 604-6.
8. Yakub M, Iqbal MP, Kakepoto GN, Rafique G, Memon Y, Azam I, et al. High prevalence of mild hyperhomocysteinemia and folate, B12 and B6 deficiencies in an urban population of Karachi, Pakistan. Pak J Med Sci. 2010;26:923-6.
9. Iqbal SP, Ahmer S, Farooq S, Parpio Y, Tharani A, Khan RAM, et al. Benzodiazepine use among adults residing in the urban settlements of Karachi: A cross sectional study. Subst Abuse Treat Prev Policy 2011; 6:19.
10. Yakub M, Iqbal MP. Association of blood lead (Pb) and plasma homocysteine: A cross sectional survey in Karachi, Pakistan. PLoS ONE. 2010; 5: e11706.
11. Khan H, Ansari MA, Waheed U, Farooq N. Prevalence of vitamin D deficiency in general population of Islamabad, Pakistan. Ann Pak Inst Med Sci. 2013; 9: 45-7.
12. Al-Mahroos FT, Al-Sahlawi HS, Al-Amer E, Mahmood NA, Sandhu AK, Sharida H, et al. Prevalence and risk factors for vitamin D deficiency among mothers in labor and their newborns. Bahrain Med Bull. 2013;35:60.
13. Karim SA, Nusrat U, Aziz S. Vitamin D deficiency in pregnant women and their newborns as seen at a tertiary-care center in Karachi, Pakistan. Int J Gynecol Obstet. 2011; 112: 59-62.
14. Jääskeläinen T, Knekt P, Marniemi J, Sares-Jäske L, Männist? S, Heli?vaara M, et al. Vitamin D status is associated with sociodemographic factors, lifestyle and metabolic health. Eur J Nutr 2013; 52: 513-25.
15. Mehmood K, Akhtar ST, Talib A, Haider I. Vitamin-D status in a population of healthy adults in Pakistan. Pak J Med Sci 2009; 25: 545-50.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: