
Zohra Kurji ( School of Nursing and Midwifery, The Aga Khan University, Karachi. )
Zahra Shaheen Premani ( Chief Operating Officer, Catco Kids, Inc., Karachi. )
Yasmin Mithani ( School of Nursing and Midwifery, The Aga Khan University, Karachi. )
July 2015, Volume 65, Issue 7
Review Articles
Abstract
Quality has multidimensional perspectives. It is a continuous and dynamic process. A systematic search of national and international literature was conducted from peer-reviewed databases MEDLINE, CINAHL and PubMed during January to July 2012. There are many frameworks to assess and measure quality. All frameworks give some levels in which quality could be assessed. Therefore, multiple frameworks should be used for measuring quality based on the situation and environment. Measuring quality is very important for primary healthcare programme, especially for developing countries because if we will not do quality assessment, our resources will not be utilised effectively and people may divert to curative services. Thus, in developing countries where healthcare system needs to optimise resources for increased population coverage and scale up the care, quality approaches can suggest workable solutions to using resources appropriately.
Keywords: Quality, Measurement of quality, Quality approaches.
Introduction
Rapid demand at the global level for healthcare management is increasing over the past few decades, increasing emphasis on healthcare quality. Before defining quality improvement it is important to define what is quality.
Problems in defining and measuring quality
Quality has multidimensional perspectives. It is a continuous and dynamic process.11 Most of the people believed that it is very difficult to define, assess or measure quality.1,2 Many others believed that it does not have any universal definition.1,2
Generally, there are four broad perspectives about quality. From professional perspective, it is just to gain technical competencies of staff, continue professional development of the staff and certification to expand the knowledge base.3-5 According to the patients, quality is defined by access to care, good repose from care-providers, low-cost treatments, improvement in their health status etc. Quality from the management\'s point of view is about optimising resources by bringing in innovative approaches. Finally, we can say that quality is an abstract concept and difficult to define.3-6
There are many studies which indicate that by improving quality, many medical errors are decreased.7 In a study, 19% to 28% of medication errors in hospitals increased due to lack of quality.7 Medication errors are the biggest and significant growing issue in healthcare and it is the cause of patient morbidity and mortality.7 One study mentioned that 44,000 to 98,000 patients die each year as a result of medication-related problems.7 Such errors affect 1.5 million people annually, increasing the per-year cost to $3.5 billion.7 One cross-sectional direct-observational study done in the surgical intensive care unit to assess nurses\' views on the factors contributing to medication errors suggested that 65% of errors could be averted by implementing strategies which will improve medication administration process.7
Measuring quality Framework
Quality assessment and improvement will promote confidence, give us clear guideline to meet the needs of the population and will increase health professional\'s satisfaction. There are many frameworks to assess and measure quality.3,6 All frameworks give some levels in which quality could be assessed. Most of the authors mentioned dimensions of quality which are measured through these frameworks. The most frequently used dimensions include effectiveness, efficiency, access, safety, equity, appropriateness, timeliness, acceptability, patient responsiveness or patient-centeredness, satisfaction, health improvement and continuity of care. Effectiveness and efficiency are integral parts of all dimensions of quality.
On the other hand, safety has not been included by some.2 Safety is a very important dimension, according to many authors, who feel that it is a very important indicator of the quality.2 Some even think that it is parallel to quality.2 Another set of dimension (Table)is appropriateness which tells us how the treatment progressed according to the need of the patient. However, this is not the part of the Department Of Health, UK and IOM frameworks.2 Timeliness explains that treatment completes within a reasonable timeframe which is only considered by the Department of Health, Institute Of Medicine and Joint Commission Accreditation of Healthcare Organisation (JCAHO).2,3 Responsiveness to patients, or patient-centeredness, describes values and preferences of individual and community.2 In addition, patient satisfaction counts as a client or community expectation of the treatment. Finally, continuity of care, which is described as connectivity of the patient during all stages, is only considered by IOM (2001).2
The discussion above indicates that none of the frame work has given a complete picture of how quality will be measured. Most of them are quantitative and not taking care of qualitative perspective of the patient. Quality is abstract and it is very individualised. It has different meanings for indivi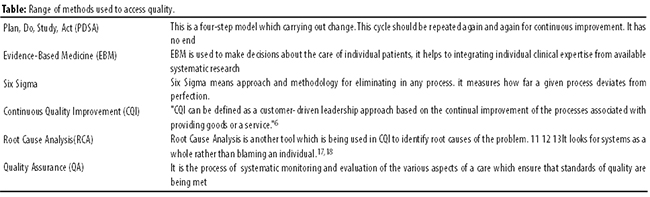
dual and very different for population. Therefore, multiple frameworks should be used for measuring quality based on situation and environment. For example, quality framework for community would be different from a hospital setting.2
Overview of quality improvement
Quality improvement is a continuous and ongoing process within a specific organisation like hospitals or clinics which work on identification of root cause of the problem, or any sentinel event and to implement evidence-based strategies to improve quality of care. It always helps to achieve better performance.8 Literature demonstrates that each organisation has clear vision of quality care due to which they are trying hard to provide comprehensive and systematic care. In addition, they adopt multiple approaches that avert errors before they occur for patient safety and to maximise quality.9 The process of quality improvement never stops because organisations want to grow by improving products and services. This proactive approach emphasises "doing the right thing" for the patient.9
The quality improvement starts with good performance key indicators which are at the benchmark level.10,11 Quality improvement of any organisation very much depends upon openness, collaboration and resources. Quality improvement process needs comprehensive approaches which include technical assistance and rewards that may be in terms of financial incentives.
Range of approaches, tools and strategies
There are several approaches that can provide solution of this problem. Some of them focus only on the professionals, whereas some others focus on organisations.11 Similarly, some approaches give importance to self-regulation, while others are centre of external control.3-5
There are three main categories — licensing, certification, and accreditation — that are used by governments and professional bodies to improve the quality of healthcare.12 All three approaches are based on external assessment and ensure quality and patient safety in healthcare organisations. Common quality improvement tools and approaches include Plan, Do, Study, Act (PDSA), Monitoring, Assessment, Evidence-Based Medicine (EBM), Total Quality Management (TQM), Quality Assurance (QA), Six Sigma and Patient Empowerment.
This paper aims at describing two of these approaches in detail.11
Continuous Quality Improvement (CQI): CQI, which is also known as Total Quality Management (TQM), is an effective practical tool to reduce errors. It was initiated by Shewart and later, Deming, Juran and others re-designed quality processes in the industry.13 During the 1980s, this approach was utilised in healthcare.8 There are many definitions of CQI/TQM but the most comprehensive is the one by Weiner et al. who defined CQI as "… an ongoing effort to provide care that meets or exceeds customer expectations".8 According to Counte et al. CQI can be "defined as a customer-driven leadership approach based on the continual improvement of the processes associated with providing goods or a service."8
CQI not only targets individual professionals but also focuses on organisations.8 Moreover, it assesses how efficiently care was provided by the organisation, team building and culture within the organisation, infrastructure and patient satisfaction.8 It is used by many Western countries and literature demonstrates that it has been very successful in a number of industries.14 In terms of health, it was first used in 1980 by USA. Yet, many limited reports exist that analyse the outcome of TQM/CQI approach.8
Moreover, literature demonstrates that one of the elements of CQI is to measure improvement, self-assessment of performance, critical analysis of efficiency and effectiveness of interventions. On the other hand, it overestimates the performance and practices which means that the results may not be accurate.8 One study reported that in rural clinics, quality of care of patients with diabetes and patients with hypertension improved as a result of a quality improvement process.8 In addition, other studies suggested that the use of CQI improved patient outcomes in the area of vascular access planning.8
Root Cause Analysis
Root Cause Analysis (RCA) is another tool which is being used in CQI to identify root causes of the problem.14-16 It looks for systems as a whole rather than blaming an individual.11,17 It also helps in identifying system errors through investigation and analysis.14,15 Furthermore, it is cost-effective and problem-preventive approach.14,15 A longitudinal found a decrease in falls in postpartum women in two large hospitals in Taiwan.18 Root causes are classified into four major categories: environment and facilities, procedure, individual, and communication.18 Results of the above study also shared that RCA can be implemented to analyse causes and then formulate interventions to reduce the incidence, thereby improving patient safety and quality.18 One more study said RCA has contributed to a decrease in the occurrence of wrong-site surgery.18 One more study reported that using RCA helps in reducing mistakes by nursing staff and improve patient safety.18 There are many tools used in RCA, for example, cause and effect or fish bone tool, barrier analysis, change analysis etc.19 RCA should be done within 45 days after every sentinel event and root cause should be identified to improve systems and processes.19 In addition, RCA focuses on system and not on individuals. Modern literature revealed that RCA is one of the approaches used for improving quality.14,19
Analysis of approaches of quality in primary healthcare
Measuring quality is very important for the primary healthcare programme and especially for developing countries because if we will not do quality assessment, our resources will not be utilised effectively and people may move towards curative services.20,21 Analysis of literature shows that whatever approaches are being used, they should focus on the solution of the problem.20,21 While selecting an approach, we need to make sure that problems or errors should not re-occur. There should be clear understanding at all levels. Appropriate approaches need to be selected on the basis of organisation\'s mission, vision and goals.13,22
In this case, using a mixed approach is the solution. Literature also mentions that these approaches will not work if used alone, and that multiple interventions are better than single interventions.11,23,24 Further analysis reveals that there are no approaches in quality improvement (QI) which address ethical issues in the proposed QI interventions. In addition, while making policies, ethical principles like minimal risk, respect for privacy and confidentiality of the client are not highlighted in QI initiatives.25
Finally, there are no \'magic bullets\' for improving the quality of healthcare, "but there is a wide range of interventions available, that if used appropriately, could lead to important improvements in professional practice and patient outcomes".13
However, whatever methodology any organisation selects, effective planning, leadership and governance, consumer involvement, information management and competence and education are key success factors.26
Who is responsible for QI initiatives?
Literature suggests that trend for quality is increasing rapidly and organisational culture advocates "quality as everyone\'s responsibility" to achieve significant and sustained outcomes.11
Maintaining quality and decreasing error is the not responsibility of any individual, but it is the responsibility of multidisciplinary teams. In this way, it gives ownership and accountability for patient safety and quality.11 As stated in literature, "Something happened. Let\'s check what went wrong together."11
QI is not a one-man show; it involves many people, policy-makers, front-line staff like doctors and nurses, and consumers in which community and patients are involved.
Policymaker\'s involvement in QI
Stakeholders who are involved at policy level have a major responsibility at national as well as regional level.27 Literature mentions that stakeholders would normally include political and community leaders, service users and their advocates, regulatory bodies, and representative bodies etc.27 One more study suggested that without leader\'s involvement, change will be difficult to sustain.24 Many countries like Sweden, Australia, UK, the Netherlands, and Japan have introduced involvement of leaders in QI strategy.24 Hence, literature highlights that support has to come from the top to achieve successful QI outcomes.11
Health provider\'s involvement in QI
Improvement in quality is not the sole responsibility of health care providers.27 Physicians, nurses, paramedics, staff are all part of the QI initiative. In addition, 45% of physicians believed that leaders cannot work in isolation.28 In America, hospital nurses play vital role in high quality patient care.19 Moreover, physician involvement in early stage during CQI shows very successful outcomes.19 Another study done in Nicaragua on one of the projects on essential obstetric care used partographs and observed that within 10 months, maternal mortality decreased from 10 in 1999 to 2 in 2000.19
Communities and service users\' involvement in QI
Consumers have critical role and responsibility in quality improvement.23 Literature highlights that patient engagement in quality initiative is a vital part in improving quality intervention and brings effective outcomes.23 Several studies demonstrate that patient involvement in healthcare interventions affect the function of the practice and it leads to improvement in patient outcomes. Literature also shows that patient and family involvement in participating in their own care will improve quality and reduce cost of care.23 On the contrary, literature highlights that some patients do not want to participate in their treatment; for instance, terminally ill patients.29
Barriers and success factors in QI
There are many success factors which influence QI such as strong leadership commitment, support and consistency in all QI steps. Moreover, leadership, direction, organisational culture, training, resources, and practical support are all important.30
Leaders are involved in ensuring adequate financial resources, training staff on QI and purchasing innovative technologies and equipment. As change is not always easy, it becomes the leader\'s responsibility to provide administrative support, especially in those QI projects which are time-consuming. Results of a study revealed that more than half of physicians shared the perception that leaders are "instrumental" in deciding to pursue QI.
Institutional factors are also very important in QI success, like strong commitment for culture that value team-building. A study mentioned that team should be the focus of QI programmes rather than the physicians.28 Team building in QI helps members to anticipate problems and overcome potential barriers. Moreover, another study said multidisciplinary approach enables team to focus on the accomplishment of goals.31
Organizational culture is an important success factor for effectiveness of QI. Cultural attributes for the development of quality is essential. Literature demonstrates that hospitals known to be "good places to work" have a lower medicare mortality rate. In addition, organisational support and culture also affect job satisfaction and decrease burnout, which impact quality of care and lead to good QI initiative. Moreover, safety culture of staff and patients is the key indicator in organisational cultural tool. Besides, organisational culture is correlated with financial performance which helps in higher development in staff training, recognising performance, customer satisfaction, downward communications, openness to change and job satisfaction.28,31
Barriers of QI
Leadership is the key domain of an organisation. There is clear evidence that if leadership will not be strong and consistent at every level, desired outcomes of quality will not be obtained.27 One of the quasi-qualitative and quantitative case studies done in Kraaifontein healthcare shared barriers faced during the implementation of QI. They faced challenges such as lack of top management, active involvement, inconsistent stakeholders, lack of commitment, rigid organisational structure, lack of communication between management and employees etc., which lead to obstacles in employee empowerment and ownership. In addition, lack of a recognition and reward system for team work, poor collection and analysis of data, rigid and punitive culture are also barriers in quality improvement.28,31
Leadership styles can be important barriers in the implementation of QI. Literature demonstrates that leadership styles and transformational leaders are the driving force in bringing necessary changes to attain the vision of the organisation. Studies reveal that autocratic leaders refuse to be challenged by their subordinates. On the contrary, transformational leaders give autonomy and ownership to their subordinates and empower them. Thus, leadership style could be the greatest barrier in QI.28,31
Lack of education and training of employees about TQM
Every employee needs to learn about the process and underlining principles of QI. Knowledge deficit in quality initiative is the biggest resistance to change. For example, if staff has no awareness and importance of quality, they are reluctant to change and get easily burnt out. For example, in our hospital, when the system was changed for medication order from manual to computer, initially staff was not comfortable and was scared in terms of error, but ongoing training made them comfortable and they realised the benefit of the system.28,31
Literature reveals that organisations should create environment that encourage learning and training of QI before its implementation.23,28 Another study suggested that poor education and lack of training were major obstacles during implementation of QI. Knowledge deficit also leads to unwillingness to participate in QI implementation.28,31
Conclusion
In developing countries where healthcare systems need to optimise resources for increased population coverage and scale up the care, quality approaches can suggest workable solutions to using resources appropriately. In this way, best solution could be achieved by improving quality strategy.
Reference
1. Choudhry T M. Maternal Mortality and Quality Of Maternity Care Implications For Pakistan [Thesis For Degree Of Master In Health Promotion]. Karolinska Institute Department of Public Health Science; 2005.
2. Quigley L H, McKee M, Nolte E, Glinos A I. Assuring The Quality Of Health Care In The European Union. A Case Of Action. (Online) 2008 (Cited 2011 Dec 15). Available from URL: http://www.akaz.ba/Agencija/Dokumenti/EU_Quality_Healthcare.pdf.
3. Campbell, SM, Roland, MO, Buetow, SA. Defining quality of care. Social Sci Med 2000; 51: 1611-25.
4. Howie JG, Heaney DJ, Maxwell M. Measuring quality in general practice. Pilot study of a needs, process and outcome measure.Occas Pap R Coll Gen Pract.1997;75:i-xii, 1-32.
5. Papp R, Borbas I, Dobos E, Bredehorst M, Jaruseviciene L, Vehko T, etal. Perceptions of quality in primary health care: perspectives of patients and professionals based on focus group discussions. BMC FamPract 2014; 15: 128.
6. Mohamed N. Quality Improvement Techniques to Control Medication Errors In Surgical Intensive Care Units At Emergency Hospital. J Med Biomed Sci 2010; 2078: 2073.
7. Anon. What is quality? Quality in General Practice.University College London; 2011. Chapter 2; MSc in International Primary Health Care Course Material.
8. Stephenson.The Evidence for Continuous Quality Improvement. (Online) 2009 (Cited 2011 Feb 15). Available From URL: www.racgp.org.au/Content/NavigationMenu/.../qacpd_literaturereview.pdf.
9. Talylor HA, Pronovost PJ, Faden RR, Kass NE, Suqarman J.The Ethical Review Of Health Care Quality Improvement Initiatives: Issue Brief(common wealth fund). (Online) 2010 (Cited 2011 Feb 16). Avaiable from URL: http://www.ncbi.nlm.nih.gov/ pubmed/20726137.
10. Anon. Rewarding Quality Performance: The Role of Nursing. The Alliance for Health Reform. (Online) 2007 (Cited 2011 Feb 17). 2007. Available from URL: www.allhealth.org/.../Quality.../Rewarding_Quality_Performance_Nursing_ 51.pdf.
11. Moss F ,Palmberg M, Plsek P, Schellekens W . Quality improvement around the world: how much we can learn from each other.Qual Health Care 2000;9:63-6.
12. Zeribi K N, Marquez L. Approaches To Healthcare Quality Regulation In Latin America And The Caribbean: Regional Experiences And Challenge. Latin American and Caribbean Regional Health Sector Reform Imitative; Report No: 63.
13. Stephenson.The Evidence for Continuous Quality Improvement. (Online) 2009 (Cited 2011 Feb 15). Available From URL: www.racgp.org.au/Content/NavigationMenu/.../qacpd_literaturereview.pdf.
14. Anon. Rapid PDSA cycles - improving practice processes for the care of patients with diabetes. (Online) 2010 (Cited 2011 Feb 15). Available from URL: www.racgp.org.au/ Content/NavigationMenu/.../Cat1_RapidPDSAcycles.pdf.
15. Woloshynowych, M, Rogers S ,TaylorAdams S, Vincent C. The investigation and analysis of critical incidents and adverse events in healthcare. Health Technol Assess 2005 ;9:1-143.
16. Pham JC , Kim J, Natterman JP, Cover RM, Goeschel CA, Wu AWet al. Recasting the RCA: An Improved Model for Performing Root Cause Analyses. Am J Med Qual; 2010; 25: 186-91
17. Mills PD, Neily J, Luan D, Stalhandske E, Weeks WB. Using aggregate root cause analysis to reduce falls. JtComm J Qual Patient Saf 2005; 31: 21-31.
18. Draper DA, Felland LE, liebhaber A, Melichar L. The Role of Nurses in Hospital Quality Improvement. Research Brief No. 3. (Online) 2008 (Cited 2011 Feb 17). Available from URL: www.hschange.com/CONTENT/972/.
19. Chen K H, Chen L R, Su1S. Applying root cause analysis to improve patient safety: decreasing falls in postpartum women. QualSaf Health Care 2010; 19: 138-43.
20. Brown L D, Franco L M, Rafeh N, Hatzell T. Quality Assurance of Health Care In Developing Countries. (Online) 2006 (Cited 2011 Feb 15). Available From URL: www.qaproject.org/pubs/PDFs/ DEVCONT.pdf.
21. Bengoa R, Kawar R, Key P, Leatherman S, Massoud R, Sturno P. Quality of care: A process for making strategic choices in health systems. World Health Organization Press; 2006, pp 1-50.
22. Dean L G, Comparison of Common Root Cause Analysis Tools and Methods. Apollo Root Cause Anal; A new way of Thinking. (Online) 2010 (Cited 2011 Feb 15). Available from URL: www.apollorca.com/_public/ site/files/ARCA_Appendix.pdf.
23. Parsons S, Winterbottom A, Cross P, Redding D, The quality of patient engagement and involvement in primary care. The King\'s Fund. (Online) 2010 (Cited 2011 Feb 15). Available from URL: forces4quality.org/af4q/download-document/6629/3430. (Cited 12 Feb 2012).
24. Dana B.Continuous Quality Improvement (CQI) Readiness Assessment Process And Tool. American Health association[online] 2004 [cited 2011 Feb 15]; Available from: URL:www.ahcancal.org/ncal/quality/Documents/cqi_rai_tool.pdf
25. Anon. Batter quality, batter Health care. A Safety and Quality Improvement Framework for Victorian Health Services. Metropolitan Health and Aged Care Services. (Online) 2005 (Cited 2011 Feb 15). Available from URL: www.healthcaregovernance.org.au/.../bettrer-quality,-better-healthcare.pdf.
26. Andersen, B, Fagerhaug T. Tools for root cause Identification. Root cause analysis: simplified tools and techniques. 2nd ed. AQS Quality Press; 2006, pp 117-40.
27. Grol R. Improving the quality of medical care: Building bridges among professional pride, payer profit, and patient satisfaction. J Am Med Assoc 2001; 286: 2600-01.
28. Shortell SM, Bennett0 CL, Byck GR. Assessing the impact of Continuous Quality Improvement on clinical practice: What it will take to accelerate progress. Milbank Quart; 1998; 76 (4). DOI: 10.1111/1468-0009.00107.
29. Walshe K, Freeman T. Effectiveness of quality improvement: learning from Evaluations. QualSaf Health Care; 2002; 11: 85.
30. Hughes R G. Tools and Strategies for Quality Improvement and Patient Safety. In: Hughes R G (ed.). Patient safety and quality on evidence hand book for nurses.USA: Rockville; 2008.
31. Mohamed N, Gabr H, Quality Improvement Techniques To Control Medication Errors In Surgical Intensive Care Units At Emergency Hospital. J Med Biomedical Sci 2010; 2078: 2073.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: