
Cuneyt Kirkil ( Firat University, Medical Faculty, Department of General Surgery, Elazig, Turkey. )
Nurullah Bulbuller ( Ataturk Teaching and Education Hospital, Department of General Surgery, Antalya,Turkey. )
Yavuz Selim Ilhan ( Firat University, Medical Faculty, Department of General Surgery, Elazig, Turkey. )
Erhan Aygen ( Firat University, Medical Faculty, Department of General Surgery, Elazig, Turkey. )
Serdar Coskun ( Gazi State Hospital, Department of General Surgery, Samsun, Turkey. )
Baris Gulturk ( Harput State Hospital, Department of General Surgery, Elazig, Turkey. )
March 2015, Volume 65, Issue 3
Original Article
Abstract
Objective: To analyse outcomes of variable management strategies for the treatment of Acute Cholecystitis in relation to morbidity, mortality and conversion to open surgery.
Methods: The retrospective study was conducted at Firat University Hospital, Turkey and comprised records of Acute Cholecystitis patients admitted between 2005 and 2011. Patients were divided into subgroups according to admission time as well as American Society of Anaesthesiologists score. The outcomes of early cholecystectomy, interval cholecystectomy, delayed cholecystectomy, \'cooling-off\' therapy and percutaneous cholecystostomy were evaluated. Mortality, morbidity, and conversion to open surgery were calculated as measures of success. Data was analysed using SPSS.
Results: Of the 1557 patients, 1052(67.6%) were female. The overall mean age was 42.4±14.7 years. Success rates of \'cooling-off\' therapy and percutaneous cholecystostomy were 89.3% and 96.3%, respectively. The conversion rate following delayed cholecystectomy was 30%, which was higher than that of both early and interval cholecystectomy (0.2% and 0%, respectively; p<0.001 each). Mortality and morbidity rates of delayed cholecystectomy (57.1% and 7.1%, respectively) were also significantly higher than early and interval cholecystectomy (5% and 0.1%; 5.6 and 0%, respectively).
Conclusion: Early laparoscopic cholecystectomy and interval cholecystectomy shared similar outcomes and rates of efficacy. Percutaneous cholecystostomy was a successful treatment option for high-risk patients, while delayed cholecystostomy correlated to the highest rates of conversion to open surgery, mortality and morbidity.
Keywords: Cholecystitis, Laparoscopic, Cholecystostomy. (JPMA 65: 277; 2015).
Introduction
The standard treatment for Acute Cholecystitis (AC) is laparoscopic cholecystectomy (LC). Classification of LC varies according to the timing of the procedure, with three distinct time periods of therapy defined: early cholecystectomy (EC), interval cholecystectomy (IC) and delayed cholecystectomy (DC). The classification is dependent on symptom presentation as well as physician recommendations regarding the need for and/or urgency of treatment. Although minimally invasive, LC is ultimately a surgical procedure requiring judgment and rigorous clinical oversight to ensure that the most appropriate treatment method is selected.
In the light of literature,1 it is widely accepted that early intervention is a favourable treatment method. Prospective studies have indicated early LC (treatment performed within 72 hours of symptom onset) offers significant advantages over either IC or DC. These advantages include decreased rates of conversion to open surgery (CONV), decreased length of hospital stay, and decreased overall morbidity.2,3 Despite these well-recorded benefits, LC is not always a viable treatment method.
In instances where a patient\'s physiological stability and overall health is precarious in nature, or alternatively where the patient refuses consent for surgery, medical therapy known as \'cooling-off\' is implemented. \'Cooling-off\' is a non-invasive conservative therapy, but the outcomes of the procedure are not definitive, with many non-responsive patients requiring immediate surgical intervention. In the light of such circumstances, percutaneous cholecystectomy (PC) is performed to address urgent decompression of an inflamed gallbladder. This is particularly common among high-risk patients.
The present study was planned to analyse results of various management strategies applied in the treatment of AC.
Patients and Methods
The retrospective study was conducted at Firat University Hospital, Turkey and comprised records of Acute Cholecystitis patients admitted between 2005 and 2011. Patients were divided into subgroups according to admission time as well as American Society of Anaesthesiologists (ASA) score. Following institutional approval from the Chief Physician\'s Office, patient records were retrieved. In all cases, AC was assessed according to three-pronged diagnostic criterion: acute upper abdominal pain with tenderness under the right costal margin; fever of more than 37.5ºC, leukocytosis of more than 10K/uL, or both; ultrasonography evidence (thickened gall bladder wall, oedematous gallbladder wall, presence of gallstones, ultrasonographic Murphy\'s sign, and pericholecystic fluid collection). Patients with cholangitis, pancreatitis, or choledocholithiasis were excluded.
A treatment algorithm was applied to the patients whose records were obtained for evaluation (Figure-1).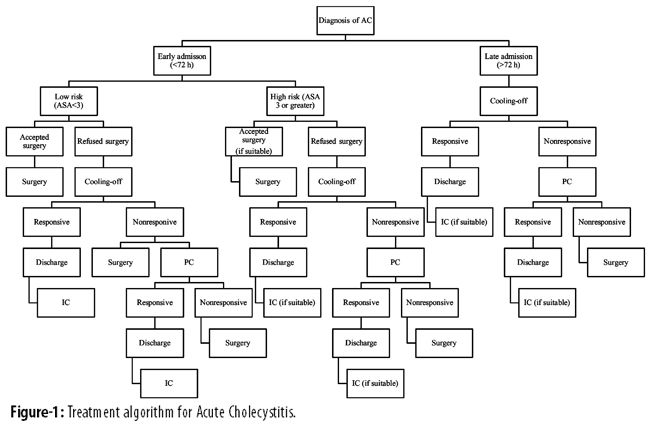
Patients with ASA score of 3 or more were categorised as high-risk patients. Hospital admission within 72 hours following symptom onset was classified as early admission, and anything outside of this time frame was considered late admission. For those undergoing \'cooling-off\' therapy, treatment was delivered with intravenous (IV) hydration and IV antibiotics to address enteric micro-organism activity. All surgical procedures were performed under general anaesthesia, and PC catheters were inserted under sonographic visualisation using percutaneous transhepatic approach. Success of either \'cooling-off\' or PC therapy was defined as clinical improvement within 48-72 hours. IC procedures were executed according to life expectancy, medical co-morbidities and after obtaining consent of the patient and the family.
Analysis of patient records included evaluation of both initial therapies prescribed as well as all subsequent treatment methods deemed necessary to achieve full AC recovery. Of specific consideration was identifying those patients who underwent IC or PC procedures following \'cooling-off\'. The records of these patients were assessed according to the following characteristics and sub-classifications: age, gender, admission time, ASA score, additional systemic diseases, treatment methods, treatment-related complications, and mortalities. Patients who required IC or PC therapy as an additional treatment procedure, but did not return to the same health facility where their initial therapy had been conducted, were contacted via telephone wherever possible.
The Mann-Whitney U test was used to compare median parametric data of two groups (comparisons for early admission versus late admission, high risk versus low risk, and early laparoscopic cholecystectomy versus interval laparoscopic cholecystectomy); chi-square tests were used to compare non-parametric data of the same two groups. Kruskal-Wallis test followed by post-tests was used for the comparison of non-parametric data between three groups (early, delayed, and interval cholecystectomies). All calculations were performed using the SPSS 12. Value of p<0.05 was considered statistically significant.
Results
Of the 1557 patients, 1052(67.6%) were female. The overall mean age was 42.4±14.7 years. The median age of high-risk patients was 72 years (range: 38-82 years), and it was 41 years (range: 24-59 years) for low-risk patients (p<0.05). Differences in admission time between low-risk and high-risk patients was not statistically significant (p>0.05). The management plans used for patients with AC was noted (Figure-2).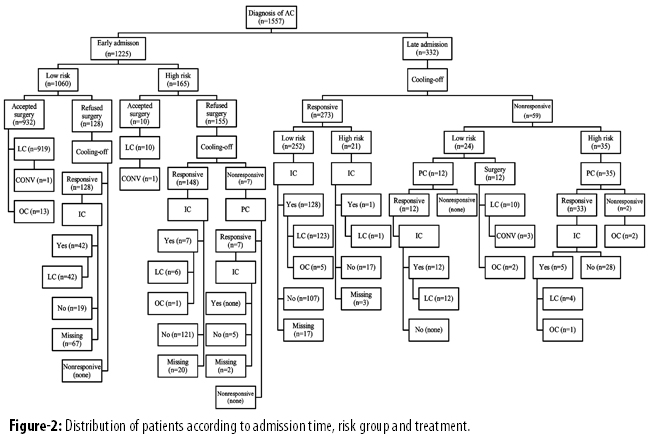
The rates of open cholecystectomy (OC), CONV, surgical complications and morbidity according to the timing of treatment were also noted (Table-1).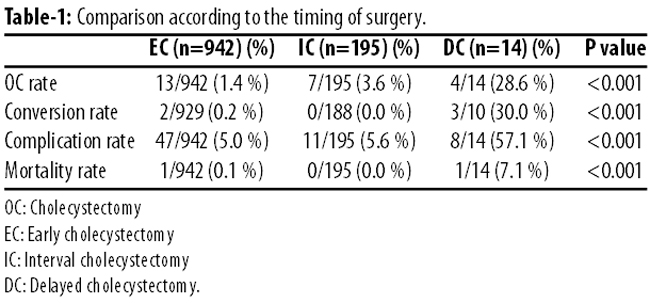
Of the 1,225 patients admitted early, 942(76.(%) underwent EC. Of these patients, 927(98.4%) completed treatment laparoscopically; CONV was required for only two patients (two of 929 patients 0.2%). Besides, (47 of 942 patients 5%) who underwent EC had complications, but these were minor in nature, like wound infection, haematoma and spontaneously-resolved bile leakage. An aberrant bile duct injury was found in 1(0.1%) patient and the damaged organ was attended with nasobiliary drainage. Only 1(0.1) case of mortality was recorded among EC patients. The patient in question had a recorded history of ventricular premature beats, and suffered a fatal arrhythmia intra-operatively.
\'Cooling-off\' therapy was successful in 549(89.3%) of 615 patients. The success rates of \'cooling-off\' were higher in low-risk and early-admission groups (Table-2).
PC was performed on 54(8.7%) patients who were non-responsive to \'cooling-off\', with a success rate of 96.3% (52 of 54 patients) achieved. Of the 54 PC patients, 1(1.85%) mortality was recorded; the patient had previously been diagnosed with Guillain-Barré syndrome (GBS), immediately placing the individual in the high-risk group for general anaesthesia. The patient was first treated via PC, but when a recovery response could not be established, DC was executed. Extubation could not be achieved adequately and the patient suffered progressive respiratory complications, ultimately resulting in mortality on day 12 of postoperative care.
DC treatment, at least seven-day time gap between symptom presentation and surgical intervention in an acute exacerbation, was performed on 12(1.95%) low-risk patients who were non-responsive to \'cooling-off\'. Of them, 2(16.66%) patients who did not respond to PC treatment also underwent DC (inclusive of pre-diagnosed GBS candidate), resulting in a total DC sample size of 14(2.27%). Surgical procedure was started as laparoscopically for ten patients. The conversion rate of DC patients was 30% (three of 10 patients). The rates of CONV and OC for DC patients were higher than EC and IC patients (p<0.001 each). Further, 8 of 14 patients (57.1%) patients treated with DC revealed signs of complications. The conditions requiring additional surgery included a main bile duct stricture, a wound dehiscence and a retained foreign body located in the abdominal cavity. The GBS patient, who was initially treated with PC therapy, was the only (7%) recorded mortality of the DC group. Mortality and morbidity rates of DC patients were significantly higher than EC and IC patients (p<0.001 each).
A total of 601(38.6) patients were treated with either \'cooling-off\' therapy or PC. Of tem, 109(18.13%) patients could not be contacted to verify if treatment beyond \'cooling-off\' or PC had been required to achieve stabilisation. It was established that 195 of the original 601(32.44%) underwent IC (operative treatment conducted >2 months following successful \'cooling off\' therapy). Execution of IC for low-risk patients was 59.1% (182 of 300 patients), while the rate recorded for high-risk patients was 7.1% (13 of 184 patients) (p<0.001). Of the 195 IC patients, 188(96.4%) underwent surgery laparoscopically; the conversion rate for this sample group was zero. Eleven (5.6%) IC patients experienced complications, but these events were minor in nature, like wound infection, haematoma and spontaneously-resolved bile leakage, and did not require additional intervention. There was no statistical significance between the type of surgery, rates of conversion to OC, morbidity or mortality for patients who underwent EC and those treated with IC (p>0.05; p>0.5; p>0.5; and p>0.5, respectively).
Discussion
According to the most recent recommendations for AC treatment, as presented in the Tokyo Guidelines For Management of Acute Cholecystitis (TG13), EC within 72 hours of symptom onset is recommended for patients with Grade I (mild) AC.4 In instances where the patient elects conservative treatment as opposed to surgery, if a recovery response to the initial treatment is not achieved within 24 hours, and if the time frame observed remains within 72 hours of symptom onset, TG13 recommends EC or biliary drainage. TG13 advises patients with Grade II (moderate) and Grade III (severe) AC at high surgical risk to undergo immediate biliary drainage. Patient data analysed in the present study related to the period 2005-2011, and the treatment algorithm was established prior to the TG13 guidelines, but is compatible and strongly aligned to the current recommendations.
The effectiveness of LC in the treatment of AC has been acknowledged for two decades.5 Today, most authors agree that early LC and IC share the same clinical outcomes as well as similar measurements of safety insofar as surgical procedures for the treatment of AC are concerned.6,7 In the present study, the results of LC patients closely mirrored IC patients when treatment was performed within 72 hours of symptom onset; the data revealed an IC conversion rate of zero, with all associated postoperative therapies contributing few complications. This is a strong indication that the already documented benefits of early LC can also be achieved with IC. It was also found that DC patients correlate more closely to high rates of OC, CONV, and morbidity when compared to early LC or IC patients. The results indicate that when either immediate LC treatment is absent or recommendations to proceed to IC are excluded, the success rate of AC therapy is markedly reduced. One study8 reported a figure of 26% for patients that failed to respond to conservative treatment, and were subsequently required to undergo urgent cholecystectomies of heightened complexity as a result of delays in treatment activity. The combined data highlights the fundamental obstacle faced by high-risk patients: eliminate surgical complications by electing \'cooling-off\' therapy while simultaneously increasing the likelihood of severe medical risks arising if initial non-operative treatment is unsuccessful, or follow a non-conservative pathway and accept the prospective compounding health issues associated with any surgical procedures. To address this point, great advances have been achieved and experience expanded in the field of laparoscopic surgery, with new techniques defined to prioritise safety and efficacy of LC treatment in patients with subacute cholecystitis.9 A study10 described a dissection technique between the outer and inner subserosal layers of the gallbladder, reporting that the surgery was successfully completed laparoscopically in all the 39 patients with subacute cholecystitis. Another study11 also reported that early LC can be performed with exceptional accuracy and with high rates of success in subacute cholecystitis patients where symptoms commenced within 72 hours, but not more than 7 days, before admission. The high CONV and morbidity rates recorded for patients of the present study who underwent DC could be attributed to the timing of the surgery (>7 days post-symptom onset).
Patients with AC are traditionally treated with the application of \'cooling-off\' therapy when surgery is deemed unsuitable, but there are still many physicians strongly advocating surgical intervention as the primary care method for AC patients. A study12 reported the results of a programme whereby 82% of medically treated AC cases were resolved. The programme elected the use of emergency surgery in high-risk elderly patients rather pursuing conservative therapy in order to minimise morbidity risk. Furthermore, a study13 advocated that symptomatic gallstones should be removed at the first emergency presentation, arguing that recurrent painful symptoms for AC patients are as traumatic and debilitating as one hospital visit per patient awaiting operation. Despite the many evidence-based claims that encourage the application of surgical intervention for the treatment of AC, the effectiveness of conservative therapies should not be overlooked. As already noted, the techniques applied in conservative treatment methods are progressing in both sophistication and safety, with success rates growing every day. The overall success rate of \'cooling-off\' therapy in the present study was found to be higher than data in English literature (89% vs. 74-82%).8,12 All of the 128 patients medically treated in low-risk group were symptomatically relieved.
The rationale for surgical treatment of traditional diseases is no longer discussed.14,15 Rather than evaluating the outcomes of conservative versus non-conservative AC therapies, focus should be directed towards ascertaining the appropriate therapy for each demographic or sub-class of patients. One study16 supports this view, commenting on rates of AC treatment success according to age. The study reported that patients of the category 65+ years demonstrated significantly higher rates of conversion to OC and postoperative complications than those in younger age groups. Furthermore, while surgical risk following general anaesthesia in patients with ASA classification 3 is recorded at 1.7%,17 LC performed on elderly patients with major co-morbidity, or those patients who are seriously ill, can result in mortality rates of up to 4.5%. This is an unaccepted mortality rate,18 hence PC has been proposed and accepted as an alternative to emergency cholecystectomy for nearly two decades.19
While there is some evidence to suggest PC is better tolerated than cholecystectomy for the elderly or otherwise seriously ill patients, a study places this theory under scrutiny. The study details wide-ranging values in relation to patient conditions and outcomes, reporting success and mortality rates of PC to the values of 57%-100% and 0%-60%, respectively.20 This would suggest that the data confirming the reliability and accuracy of PC treatment is less than exact, but further review indicates that the studies in question included large numbers of patients with unclear diagnoses (including sepsis of unknown origin); excluding such cases presents a different set of statistics for assessing the rates of success and mortality associated with PC treatment. Specifically, it was found that in cases where diagnosis was unclear, the success rate was lower (72%) and a mortality rate higher (34%). Overall success and mortality rates of the present study were 86% and 15% respectively. In addition, \'cooling-off\' therapy and PC treatment reduced conversion rates from 30% to zero when compared with DC cases. One study reported similar findings with conversion rates reduced from 9.6% to 3.3% following PC treatment.21 The high success and low mortality rates of PC in the present study support the argument: "correct diagnosis of AC maximises patient recovery success following PC".21
Results of the present study provide unambiguous statistics regarding outcomes of the currently available health management strategies for the treatment of AC: LC and IC are equally safe and effective treatment options; low-risk patients and those categorised as early admission are most responsive to \'cooling-off\' therapy; PC is a successful treatment option for high-risk patients; DC therapy is correlated with the highest rates of CONV, OC, mortality and morbidity. The algorithm applied to the 1,557 patients assessed is considered sound, well-established and well-documented, but it is acknowledged that retrospective studies do not provide the strength of evidence generated by prospective, randomised and controlled studies. The highly anticipated results of CHOCOLATE trial22 will prove critical for determining the benefit and future applications of PC.
Conclusion
Early laparoscopic cholecystectomy and interval cholecystectomy shared similar outcomes and rates of efficacy. Percutaneous cholecystostomy was a successful treatment option for high-risk patients, while delayed cholecystostomy correlated to the highest rates of conversion to open surgery, mortality and morbidity.
References
1. Koo KP, Thirlby RC. Laparoscopic cholecystectomy in acute chlecystitis. What is the optimal timing for operation? Arch Surg 1996; 131: 540-5.
2. Lo CM, Liu CL, Fan ST, Lai ECS, Wong J. Prospective randomized study of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg 1998; 227: 461-7.
3. Uchiyama K, Onishi H, Tani M, Kinoshita H, Ueno M, Yamaue H. Timing of cholecystectomy for acute cholecystitis with cholecystolithiasis. Hepatogastroenterol 2004; 51: 346-8.
4. Mayumi T, Someya K, Ootubo H, Takama T, Kido T, Kamezaki F, et al. Progression of Tokyo Guidelines and Japanese Guidelines for management of acute cholangitis and cholecystitis. JUOEH 2013; 35: 249-57.
5. Rattner DW, Ferguson C, Warshaw AL. Factors associated with successful laparoscopic cholecystectomy for acute cholecystitis. Ann Surg 1993; 217: 233-6.
6. Yamashita Y, Takada T, Kawarada Y, Nimura Y, Hirota M, Miura F, et al. Surgical treatment of patients with acute cholecystitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg 2007; 14: 91-7.
7. Saeb-Parsy K, Mills A, Rang C, Reed JB, Harris AM. Emergency laparoscopic cholecystectomy in an unselected cohort: a safe and viable option in a specialist centre. Int J Surg 2010; 8: 489-93.
8. Johansson M, Thune A, Blomqvist A, Nelvin L, Lundell L. Management of acute cholecystitis in the laparoscopic era: results of a prospective, randomized clinical trial. J Gastrointestinal Surg 2003; 7: 642-5.
9. Ota A, Kano N, Kusanagi H, Yamada S, Garg A. Techniques for difficult cases of laparoscopic cholecystectomy. J Hepatobiliary Pancreat Surg 2003;10:172-5.
10. Honda G, Iwanaga T, Kurata M. Dissection of the gallbladder from the liver bed during laparoscopic cholecystectomy for acute or sub acute cholecystitis. J Hepatobiliary Pancreat Surg 2008;15: 293-6.
11. Yüksel O, Salman B, Yilmaz U, Akyürek N, Tatlicioglu E. Timing of laparoscopic cholecystectomy for subacute calculous cholecystitis: early or interval -a prospective study. J Hepatobiliary Pancreat Surg 2006;13:421-6.
12. Sánchez-Beorlegui J, Lamata-Hernández F, Lagunas-Lostao E, Monsalve-Laguna E, Peñalva-Segura P. Choice of therapeutic approach for acute cholecystitis in the elderly. Rev Gastroenterol Mex 2010; 75: 149-57.
13. Anwar HA, Ahmed QA, Bradpiece HA. Removing symptomatic gallstones at their first emergency presentation. Ann R Coll Surg Engl 2008; 90: 394-7.
14. Turhan AN, Kapan S, Kütükçü E, Yigitbas H, Hatipoglu S, Aygün E. Comparison of operative and non operative management of acute appendicitis. Ulus Travma Acil Cerrahi Derg 2009;15: 459-62.
15. Hansson J, Körner U, Ludwigs K, Johnsson E, Jönsson C, Lundholm K. Antibiotics as first-line therapy for acute appendicitis: evidence for a change in clinical practice. World J Surg 2012; 36: 2028-36.
16. Cui W, Zhang RY, Sun DQ, Gong RH, Han TQ. Early laparoscopic cholecystectomy for acute gallbladder disease in Chinese elderly. Hepatogastroenterology 2010; 57: 409-13.
17. List WF, Kröll W, Filzwieser G. Perioperative risk in critically ill surgical patients. Anaesthesist 1985; 34: 612-8.
18. Kirshtein B, Bayme M, Bolotin A, Mizrahi S, Lantsberg L. Laparoscopic cholecystectomy for acute cholecystitis in the elderly: is it safe? Surg Laparosc Endosc Percutan Tech 2008; 18: 334-9.
19. Patterson EJ, McLoughlin RF, Mathieson JR, Cooperberg PL, MacFarlane JK. An alternative approach to acute cholecystitis. Percutaneous cholecystostomy and interval laparoscopic cholecystectomy. Surg Endosc 1996; 10: 1185-8.
20. Winbladh A, Gullstrand P, Svanvik J, Sandström P. Systematic review of cholecystostomy as a treatment option in acute cholecystitis. HPB (Oxford) 2009; 11: 183-93.
21. Tsumura H, Ichikawa T, Hiyama E, Kagawa T, Nishihara M, Murakami Y, et al. An evaluation of laparoscopic cholecystectomy after selective percutaneous transhepatic gallbladder drainage for acute cholecystitis. Gastrointest Endosc 2004; 59: 839-44.
22. Kortram K, van Ramshorst B, Bollen TL, Besselink MGH, Gouma DJ, Karsten T, et al. Acute cholecystitis in high risk surgical patients: percutaneous cholecystostomy versus laparoscopic cholecystectomy (CHOCOLATE Trial): study protocol for a randomized controlled trial. Trials 2012; 13: 7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: