
Nazan Karaoglu ( Department of Medical Education & Informatics, Necmettin Erbakan University, Meram Faculty of Medicine, Konya, Turkey. )
Sevgi Pekcan ( Department of Paediatrics, Necmettin Erbakan University, Meram Faculty of Medicine, Konya, Turkey. )
Yasemin Durduran ( Department of Community Health, Necmettin Erbakan University, Meram Faculty of Medicine, Konya, Turkey. )
Haluk Mergen ( Uludag University Family Health Center, Bursa, Turkey. )
Dursun Odabasi ( Department of Paediatrics, Ministry of Health, Konya Meram Research & Training Hospital, Konya, Turkey. )
Rahmi Ors ( Department of Paediatrics, Necmettin Erbakan University, Meram Faculty of Medicine, Konya, Turkey. )
February 2015, Volume 65, Issue 2
Original Article
Abstract
Objective: To assess levels of anxiety, depression, loneliness, burnout and job satisfaction among paediatric Residents, and how they influence each other.
Methods: The cross-sectional study was conducted at Necmettin Erbakan University, Meram, and Konya Meram Education and Research Hospital, Turkey from January to June 2011, and comprised paediatric Residents and their counterparts from other departments who formed the control group. While maintaining confidentiality, a questionnaire was used to collect data that had elements of the University of California, Los Angeles, Loneliness Scale, Hospital Anxiety and Depression Scale, Maslach Burnout Inventory and Minnesota Job Satisfaction Questionnaire. SPSS version 13 was used for statistical analysis.
Results: Overall there were 74 Residents in the study; 43(58%) working with the paediatrics department, and 31(42%) in the control group. Overall mean age was 27.60±2.25 years. Residents who were not satisfied with the city they were living in, with their professional career and who would not choose the same career given a second chance were feeling more lonely and had higher loneliness scores (p<0.05). In contrast, anxiety among female Residents who were unsatisfied with their professional career and working conditions was significantly high (p<0.05). Positive correlation was detected between the burnout levels of Residents and their anxiety, depression and loneliness scores (r=0.74; r=0.65; r=0.36). In terms of intrinsic, extrinsic and total job satisfaction, there was an obvious negative correlation (r=-0.57; r=-0.54; r=-0.61).
Conclusion: Working conditions and professional liability were the main factors affecting the Residents. Informed decision and career willingness may help them feel better.
Keywords: Loneliness, Anxiety, Depression, Burnout, Job satisfaction, Paediatric, Residency. (JPMA 65: 183; 2015).
Introduction
It is known that medical profession puts pressure on physicians from the beginning of education years.1-3 This leads to anxiety, depression, loneliness, and burnout in physicians and affects their psychological well-being, job and life satisfaction. Personal facts like successes and expectations; professional facts like work environment and conditions; social facts like status and prestige contribute to job and life satisfaction.4-7 Loneliness, which is defined as the perception of one\'s social relations at under-expected levels, also triggers negatively biological stressors.8-10 Life satisfaction is closely related to loneliness, depression and suicidal attempts.8,11 In addition, feelings about job is related to both physical and psychological well-being.5,12,13 Job satisfaction is a positive feeling achieved when expectations are met.14 Contrary to job satisfaction, the burnout is a negatively affecting process, a response to chronic feelings and personal stresses about job. The burnout has three dimensions: emotional burnout, depersonalisation, and decrease in success. It shows itself as the loss of wish, energy, idealism and aim.15-18 It could be influenced by conditions, environment, job satisfaction, personal factors and income.12,16,17,19-23 Burnout is generally expresses itself in idealistic and highly motivated persons. Such people have high expectations of their profession and profound and long-term sustenance of such feelings results in stress, alienation, anxiety and depression.18,24 Medical education accepts idealistic and motivated students by selection and motivates them for the true diagnosis and treatment during all their practice years. Naturally, the stress and anxiety levels of the physicians become high. In more than half of the family physicians in a study, anxiety was found over the cut-off level.25 The irony is that the wellness, the mood in other words, the psychological health of the physician deteriorates. There have been a number of studies in this regard done with family physicians, general practitioners, obstetricians, gynaecologists and psychiatrists.2,5-7,12,16,17 Also, there have been such studies involving Residents and Lecturers, but there are very few studies analysing the mood, working conditions and their correlations in paediatrics residents.14 In these studies, mainly depression was analysed, but other parameters were not touched altogether. In this study, we planned to analyse the anxiety, depression, loneliness, burnout and job satisfaction levels in paediatrics Residents, and to compare their interactions with the Residents of other departments.
Subjects and Methods
The cross-sectional study was conducted at Necmettin Erbakan University, Meram, and Ministry of Health\'s Konya Meram Education and Research Hospital, Turkey, from January to June 2011, and comprised paediatric Residents and their counterparts from other departments who formed the control group.
All the Residents were randomly selected from among those who were present at the time of the study and volunteered to take part after giving verbal consent. While maintaining confidentiality, a questionnaire was used to collect data that had elements of the University of California, Los Angeles (UCLA) Loneliness Scale, Hospital Anxiety and Depression Scale (HADS), Maslach Burnout Inventory (MBI) and Minnesota Job Satisfaction Questionnaire (MJBQ). All the subjects filled the questionnaire by themselves. In case the questionnaire was not fully filled, it was excluded from the study. However, partially filled demographic sections were included.
The first section of the questionnaire included socio-demographic information and had 23 questions seeking among other things the name of the department, presence of night shifts, duration of residency, work environment, effective factors in career preference, feelings of the subject at that time, presence of a known psychiatric disorder etc.
The second section comprised the UCLA Loneliness Scale, which was validated in Turkish by Demir.26,27 The UCLA is a Likert type scale which has 10 straight and10 reverse items. Minimum and maximum possible scores are in between 20 and 80. A high score is estimated to be the indicator of loneliness. The internal consistency Cronbach coefficient was reported as 0.96, which was found to be 0.87 in our study.
The third section was based on HADS that had 14 items: 7 for anxiety, and 7 for depression.28 Odd numbered questions were for anxiety; even numbered for depression. In its Turkish validity and reliability study, the cut-off levels for depression and anxiety were 7 and 10 respectively.29 The minimum and maximum scores of the two sub-scales are 0 to 21. In our study, the internal consistency coefficient Cronbach was 0.89.
The fourth section used MBI which consisted of 22 items.30 Burnout was investigated in three sub-scales: emotional burnout, depersonalisation and decrease in personal accomplishment. Originally it is a seven-grade Likert scale, but the Turkish version of the scale was transformed to five, in which 0 represented \'never\', and 4 represented \'always\'.18,31 Emotional burnout sub-scale included 8 items (1st, 2nd, 3rd, 6th, 8th, 13th, 16th and 20th items) concerning fatigue, weariness, and decrease in emotional energy. Depersonalisation sub-scale consisted of 6 items (5th, 10th, 11th, 15th, 21st and 22nd items) which described the lack of emotion in oneself during serving and giving care. Decrease in personal accomplishment sub-scale included 8 items (4th, 7th, 9th, 12nd, 14th, 17th, 18th and 19th items) reflecting the emotion of proficiency and success. High scores of emotional burnout and depersonalisation and low scores of personal accomplishment meant burnout. In our study, the scale\'s Cronbach was 0.63.
The fifth section was the Turkish adaptation of MJSQ, which was an assessment tool for job satisfaction.32,33 It consisted of 20 items concerning internal (1st, 2nd, 3rd, 4th, 7th, 8th, 9th, 10th, 11st, 15th, 16th, 20th), external (5th, 6th, 12nd, 13rd, 14th, 17th, 18th, 19th) and general job satisfaction. General satisfaction is calculated by the division of total scores by 20; internal satisfaction score by 12 and external satisfaction score by 8. For every item, there were 5 choices between 1\'not at all\' and 5\'very satisfied\'. There were no reverse items. Minimum and maximum scores were between 20 and 100 points. The Cronbach of the scale in our study was 0.88.
SPSS version 13 was used for statistical analysis. While frequency and percentage were used for demographic data, chi-square and Fishers\'s exact test were used for the comparison of categorical variables. Mean scores were analysed by student-t test in dichotomous groups with normal distribution, and by Mann-Whitney-U test in non-normal distribution. In multiple groups one-way analysis of variance (ANOVA) and Kruskal-Wallis tests were used. Normal distribution of variables was determined with Kolmogorov-Smirnov test. Significance was accepted when p value was lower than 0.05.
Results
Overall, there were 74 Residents in the study;43(58%) working with the paediatrics department, and 31(42%) in the control group. The 43 paediatrics Residents represented 79% of the total 54 available in the two study sites. Of the total study population, 44(59.5%) were females and 30(40.5%) were males. The overall mean age was 27.60±2.25 years. The length of residency was 1 to 60 months (median=8 months; interquartile range [IQR] =23.75) (Table-1).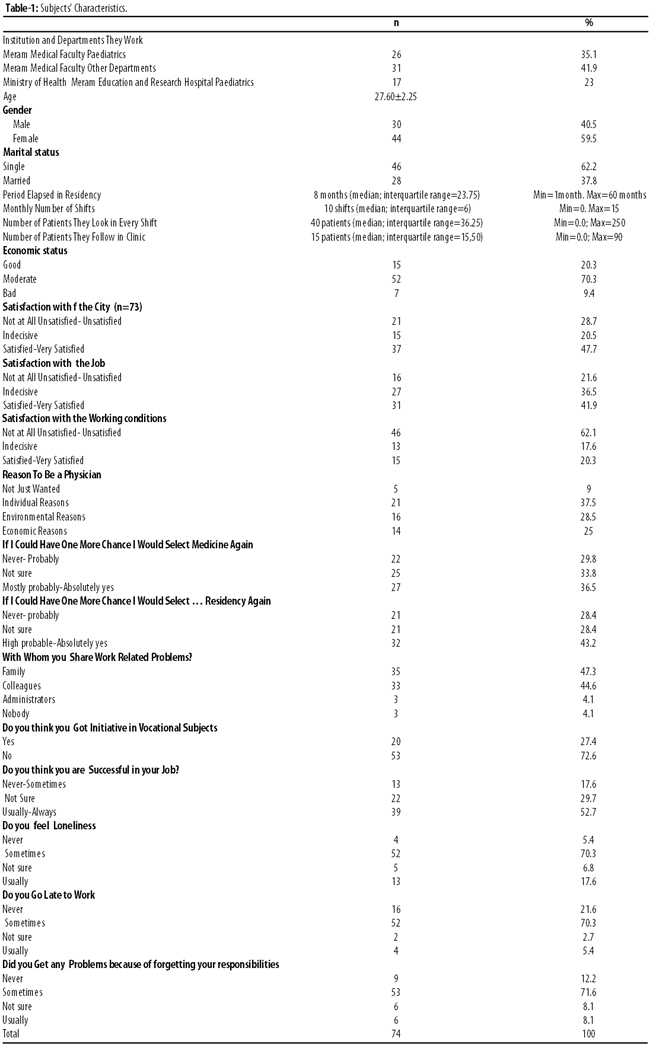
UCLA scores were high in Residents who were not satisfied with the city and the career they chose, who were feeling alone frequently and who would not like to select the same career if they were given a second chance (p<0.05). Anxiety score was high in female Residents who were unhappy with the career and working conditions (p<0.07) (Table-2).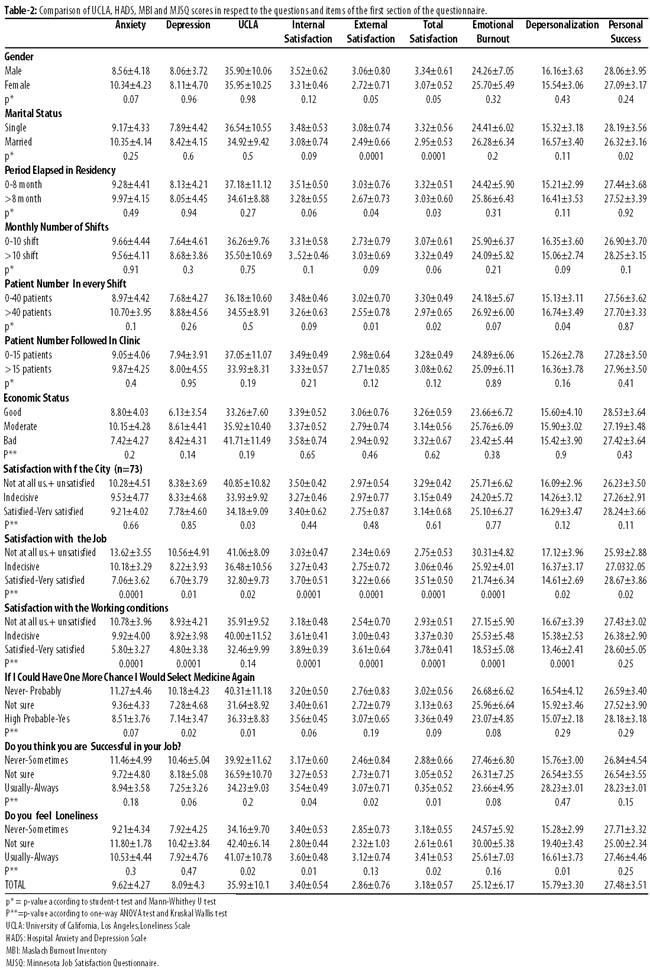
In comparison of the four scales, the paediatrics Residents had significantly low internal satisfaction scores compared with the controls (p=0.03) (Table-3).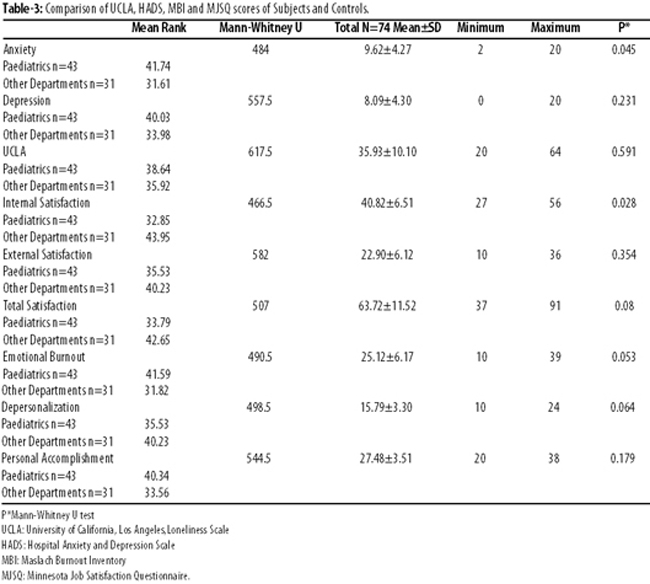
Only internal satisfaction of Residents working in the Ministry of Health Education and Research Hospital was significantly higher than the Residents working in Meram Faculty of Medicine (p=0.04) (Table-4).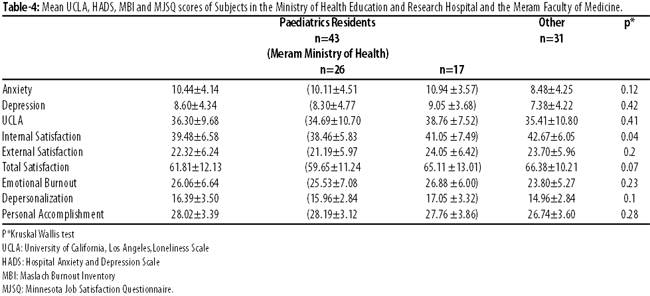
In relation to questions about professional attitudes, responsibilities and related outcomes, there were no significant differences in all the four scores (p>0.05).
Negative correlations were found between working time and internal satisfaction (r=-0.25), external satisfaction (r=-0.29) and total satisfaction (r=-0.30). Positive correlations were found between emotional burnout level of the Residents and anxiety, depression and UCLA scores (r=0.74; r=0.65; r=0.36respectively), and negative correlations were found for internal, external and total job satisfaction (r=-0.57; r=-0.54; r=-0.61respectively).
Discussion
The stakes in the medical profession are high and so are the disappointments. Working conditions contribute in both positive and negative ways, and may influence the overall outcome.1,7,16,20 This study is important for targeting a special physician group which had graduated from medical school but was still getting education in a residency programme. Besides, comparison between two groups of paediatrics Residents and with a control group also added to the significance of the study. Paediatrics residents were selected because of their hard, tiring work schedule and academic curricula. Moreover, the study compared loneliness, anxiety, depression, burnout and job satisfaction as five main groups while they could be subjects of separate and different studies.
Loneliness was 43% in a study at the same university and men were the loneliest.8 In our study there was no gender-based differences in terms of loneliness. In a previous study at the same university, mean anxiety and depression scores were 7.66±3.21 and 5.77±3.4 respectively, and male students were more depressive.4 Mean anxiety score was 9.62±4.27, mean depression score was 8.09±4.3 in this study and though the anxiety scores of female residents were higher than male residents, the difference was not significant. In addition, there was no difference between genders in respect to depression also.
Usually, studies in this area determined that personal accomplishment, job satisfaction and depersonalisation scores were higher in males and emotional burnout scores were higher in females.6 In the study, we could not find any difference among internal, external and total satisfaction, emotional burnout, depersonalisation and personal accomplishment in respect of gender. The majority of the subjects were satisfied with their jobs (78.4%) and nearly half of them would select medicine again if they could have one more chance. Residents who noted that they would never select medicine as a career if they could have one more chance to decide, had high depression and loneliness scores which supports our claim.
Marital status, job\'s requirements, work environment, shifts, social status of the job, length of service and personal characteristics are important for burnout and job satisfaction.16,7 Job satisfaction of married physicians was reported to be higher.22 In a study with teaching staff, emotional burnout was found to be more frequent among singles while depersonalisation was more frequent among married lecturers. Interestingly, the latter were found to perceive themselves successful. Authors also noted a significant difference between elapsed time in the profession and emotional burnout, depersonalisation and personal accomplishment scores. But some other studies found no relationship between marital status and emotional burnout.20 In our study, there were no relationship between married and single Residents in terms of anxiety, depression, loneliness, internal satisfaction, emotional burnout and depersonalisation. Single Residents had significantly high scores in external and total satisfaction and personal accomplishment perception. Having no marital responsibility allows them to concentrate better on their job than the married Residents and they could find more time for themselves and could cope with job problems more easily.
A study denoted that with age and length of service, job satisfaction also increases because work-related thoughts, perception and attitudes become healthier over time.22 Contrary, to these findings, external and total satisfaction was significantly higher in residents of 0 to 8 months in our study. It could be related to a confidence that they were successful in the TUS medical specialty examination. The most challenging condition of Turkish medical training is to be a Resident via earning high scores at the national TUS exam which is a very, very competitive one. However, seniority and work experience could be seen as a valuable source against emotional burnout. In another study, employees working 5 years and less had much more work-related tension than employees working greater and equal to 10 years.34 It noted an increase in work-related stress, emotional burnout and depersonalisation and a decrease in depersonalisation and personal accomplishment with age. Authors reported that work-related tensions increase while job satisfaction decreases.
In our study, number of shifts had no effect but when the number of patients became more than 40 during a shift, external and total satisfaction of the Residents decreased and depersonalisation increased significantly. The Residents experienced difficulties uniquely during night shifts because number of patients in the clinic they give care to was found to be ineffective in their well-being.
In a study, job satisfaction was found high among physicians who noted that the medical career was their own choice and thought that they did the \'right\' thing. Again in the same study, the job satisfaction of the physicians who had career goals and objectives was also high.22 Similarly, in our study, satisfaction with city, career and working conditions were influencing the Residents. While Residents who were not satisfied with the city had only high UCLA loneliness score; Residents who were not satisfied with their professional career had high anxiety, depression, loneliness, and emotional burnout and depersonalisation scores. In addition, they had low internal, external, total satisfaction and personal accomplishment scores. In terms of working conditions, those who were not satisfied with conditions had significantly high anxiety and depression scores and had significantly low internal, external and total satisfaction scores. Those Residents\' emotional burnout and depersonalisation were apparent, but there was no difference between personal accomplishments.
Burnout is a dangerous situation, especially in professions requiring mutual human relationship. Emotional burnout is the feeling of being emotionally overloaded and the depletion of resources of the individual.15,18,19 Physical burnout, insomnia, alcohol and drug abuse, besides health and familial problems, absenteeism, decreased morale and desire could lessen job satisfaction and organisational loyalty. On the other hand, use of initiative, giving feedback, rewarding, social support, providing of career development opportunities for individuals lessens emotional burnout.18,19 In this study, no difference was found in respect to anxiety, depression, loneliness, burnout, job satisfaction in Residents who didn\'t think they possess initiative, who were late for work and who had problems because of forgetting their responsibilities. It can be related to the viewpoint of our Residents about seeing themselves still as a student who had limited responsibility.
We found that depersonalisation, which is the most problematic dimension of burnout, occurred when the number of patients was greater than 40 in a shift and especially in Residents who were not satisfied with their career and working conditions. Compared with other Residents, it is important that paediatrics residents had higher depersonalisation scores, but it was not significant. However, paediatrics residents are not in close relationship with a sick child only, but also with the family. The depersonalisation of these residents may make them inattentive to the needs of patients and their relatives. Similarly, reduction of internal, external, total satisfaction, burnout, depersonalisation and personal accomplishment should be a warning for residency education. Trials to make more informed career choice and to ensure that it gets done will pre-empt the chance of producing unhappy and dissatisfied physicians.
Decrease in personal accomplishment represents reduction of proficiency and productivity of the individual. It is associated with impairment and depression in fulfilling the requirements of the job. Lack of social support and opportunities for individuals\' self-development worsen this situation.15 Indeed, in a study evaluating the relationship between job satisfaction and career vocational factors, the right choice in choosing a career, following regular publications, were noted to be related with job satisfaction. The authors noted that job satisfaction increases when climbing to the high points of the career, when the physicians think that they selected the right job and when there was an increasing interest in issues of the field.22 In a study pointing out that participation to post-graduation continuous medical education (CME) and having good communication with patients was important for avoiding work stress. It also cited that family physicians in Canada had 64% job satisfaction besides a high stress and burnout.7 In a multi-centre study involving European family physicians, burnout was related with personal issues, increased workload, low job satisfaction, which even led to the desire of quitting the profession and take recourse to alcohol, tobacco and drug usage.16
Loneliness impairs the capacity to cope with stress, causing damage in the feelings of self-value and self-efficacy.10 In our study, we found that Residents who said that they often or always felt themselves lonely had high loneliness scores contrary to their high internal and total satisfaction scores and low depersonalisation score. The perception of loneliness and social support, self-efficacy and individualisation with the changing social structure could suggest that many physicians have different perceptions. We believe that this point needs to be investigated more in detail through further studies.
In one study where physicians of paediatrics, internal medicine, paediatrics subspecialty and internal medicine subspecialty participated, work stress was found to be the lowest in paediatricians while burnout was found to be two times higher in paediatrics sub-specialty physicians than in paediatricians.14 This situation could be caused by the additional medical responsibilities upon educational responsibilities. Unfortunately, in our study there was no comparison of specialists with general practitioners, to let us make comments on the issue. However, recent studies performed among specialists and general practitioners reported a general burnout and a decrease in job satisfaction among all practicing physicians. In our study, we found no difference among other department\'s Residents and paediatrics Residents except internal satisfaction scores.
Conclusion
The study determined that the influence of working condition is not unique to paediatricians. Burnout and job satisfaction must be included in institutional, social and health policy-making machineries, and ways to cope with them must be taught. Though small in scale, the study is indicative of current trends and what can be done in the future.
References
1. Hull SK, DiLalla LF, Dorsey JK. Prevalence of health-related behaviors among physicians and medical trainees. Acad Psychiatry 2008; 32:31-8.
2. Bugdayci R, Kurt AÖ, Sasmaz T, Öner S. Mersin ?li\'nde Pratisyen ve Uzman Hekimlerde Depresyon Sikligi ve Etkileyen Faktörler. Toplum Hekimligi Bülteni 2007; 26: 32-6.
3. Alvi T, Assad F, Ramzan M, Khan FA. Depression, anxiety and their associated factors among medical students. J Coll Physicians Surg Pak 2010; 20: 122-6.
4. Nogueira-Martins LA, Neto RF, Macedo PCM, Cítero VA, Mari JJ. The mental health of graduate students at the Federal University of São Paulo: a preliminary report. Braz J Med Biol Res 2004; 37: 1519-24.
5. Becker JL, Milad MP, Klock S. Burnout, depression, and career satisfaction: Cross-sectional study of obstetrics and gynecology residents. Am J Obstet Gynecol 2006; 195: 1444-9.
6. Woodside JR, Miller MN, Floyd MR, McGowen KR, Pfortmiller DT. Observations on burnout in family medicine and psychiatry residents. Acad Psychiatry 2008; 32:13-9.
7. Lee FJ, Stewart M, Brown JB. Stress, burnout, and strategies for reducing them. What is the situation among Canadian family physicians? Can Fam Physician 2008; 54:234-5.
8. Karaoglu N, Avsaroglu S, Deniz ME. Yalniz misin? Selcuk Üniversitesi ögrencilerinde yalnizlik düzeyi ile ilgili bir calisma. Marmara Med J 2009;22: 19-26.
9. Steptoe A, Owen N, Kunz-Ebrecht SR, Brydon L. Loneliness and neuroendocrine, cardiovascular, and inflammatory stres responses in middle-aged men and women. Psychoneuroendocrinol 2004; 29: 593-611.
10. NausheenB, Gidron Y, Gregg A, Tissarchondou HS, Peveler R. Loneliness, social support and cardiovascular reactivity to laboratory stress. Stress 2007; 10: 37-44.
11. Swami V, Chamorro-Premuzic T, Sinniah D, Maniam T, Kannan K, Stanistreet D, et.al. General health mediates the relationship between loneliness, life satisfaction and depression. A study with Malaysian medical students. Soc Psych Psych Epid 2007; 42: 161-6.
12. Bressi C, Porcellana M, Gambini O, Madia L, Muffatti R, Peirone A et al. Burnout among Pschiatrists in Milan: a multicenter survey. Psychiatr Serv 2009; 60: 985-8.
13. Pines AM, Kanner AD. Nurses\' burnout: lack of positive conditions and presence of negative conditions as two independent sources of stress. J Psychosoc Nurs Ment Health Serv 1982; 20: 30-5.
14. Shugerman R, Linzer M, Nelson K, Douglas J, Williams R. Paediatric Generalists and Subspecialists: Determinants of Career Satisfaction. Paediatrics 2001; 108 ; e40.
15. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol 2001; 52: 397-422.
16. Soler JK, Yaman H, Esteva M, Dobbs F, Asenova RS, Katic M et al. Burnout in European family doctors: the EGPRN study. Fam Pract 2008;25:245-65.
17. Putnik K, Houkes I. Work related characteristics, work-home and home-work interference and burnout among primary healthcare physicians: A gender perspective in a Serbian context. BMC Public Health 2011; 11: 716.
18. Capri B. Tükenmislik ölceginin Türkce uyarlamasi: gecerlik ve güvenirlik calismasi. Mersin Üniversitesi Egitim Fakültesi Dergisi 2006; 2: 62-77.
19. Schaufeli WB, Bakker AB, Van Rhenen W. How Changes in Job Demands and Resources Predict Burnout, Work Engagement, and Sickness Absenteeism. J. Organiz. Behav 2009; 30:893-917.
20. Yürür S. Ögrenilmis güclülük, kidem ve medeni durumun duygusal tükenmedeki rolü: kaynaklarin korunmasi teorisi kapsaminda bir analiz. Atatürk Üniversitesi Iktisadi ve Idari Bilimler Dergisi, 2011; 25:107-26.
21. Ataoglu A, ?cmeli, C, Özcetin A. Hekimlerde mesleki is doyumu. Abant Izzet Baysal Üniversitesi Tip Fakültesi Dergisi 2000; 2; 17-34.
22. Sevimli F, Iscan ÖF. Bireysel ve is ortamina ait etkenler acisindan is doyumu. Ege Acad Review 2005; 5: 55-64.
23. Sutherland JV, Cooper CL. Job stress, satisfaction, and mental health among general practitioners before and after introduction of a new contract. BMJ 1992; 304: 1545-8.
24. Pines AM. Treating career burnout: A psychodynamic existential perspective. J Clin Psychol 2000; 56: 633-42.
25. Karaoglu N, Bulut S, Baydar A, Carelli F. Aile hekimlerinde durumluk ve sürekli anksiyete düzeyi: Bir vaka kontrol calismasi. Türkiye Aile Hekimligi Dergisi 2009; 13: 119-26.
26. Russell D, Peplau LA, Cutrona CE. The revised UCLA Loneliness Scale: Concurrent and discriminant validity evidence. J Pers Soc Psychol 1980; 39: 472-80.
27. Demir A. UCLA Yalnizlik ölceginin gecerlik ve güvenirliligi. Psikoloji Dergisi 1989; 7: 14-8.
28. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983; 67: 361-70.
29. Aydemir Ö. Validity and reliability of Turkish version of Hospital Anxiety and Depression Scale. Türk Psikiyatr Derg 1997; 8: 280-7.
30. Maslach C, Jackson SE. The measurement of experienced burnout. J Occup Behaviour 1981; 2: 99-113.
31. Ergin C. Doktor ve hemsirelerde tükenmislik ve Maslach ölceginin uyarlanmasi. VII. Ulusal Psikoloji Kongresi Bilimsel Calismalari. Bayraktar R, Dag ?(Editörler). Ankara: Türk Psikologlar Dernegi Yayini, 1993; pp 143-54.
32. Weiss DJ, Dawis RV, England GW, Lofguist LH. Manual for the Minnesota Satisfaction Questionnaire. Minnesota studies in vocational rehabilitation. Industrial Relations Center, Minneapolis University of Minnesota; 1967.
33. Baycan AF. Analysis of several affects of job satisfaction between different occupational groups (thesis). Bogazici university institue of social science, 1985.
34. Sünter AT, Canbaz S, Dabak S, Öz H, Peksen Y. Pratisyen hekimlerde tükenmislik, ise bagli gerginlik ve is doyumu düzeyleri. Genel Tip Derg 2006;16:9-14.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: