
Leili Hafizi ( Department of Obstetrics and Gynecology, Women's health research Center, Mashhad, IRAN. )
Nezhat Mousavifar ( Department of Obstetrics and Gynecology, Women's health research Center, Mashhad, IRAN. )
Nahid Zirak ( Department of Anesthesia, Imam Reza Hospital, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, IRAN. )
Nayereh Khadem ( Department of Obstetrics and Gynecology, Women's health research Center, Mashhad, IRAN. )
Sousan Davarpanah ( Department of Obstetrics and Gynecology, Women's health research Center, Mashhad, IRAN. )
Mohsen Akhondi ( Department of Anesthesia, Imam Reza Hospital, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, IRAN. )
February 2015, Volume 65, Issue 2
Original Article
Abstract
Objectives: To determine treatment efficacy of curettage on endometrial polyp.
Methods: The quasi-experimental pre-and-post study was conducted in 2011-12 at the gynaecology department of Imam Reza Hospital, Mashhad, Iran, and comprised patients who underwent hysteroscopy for endometrial polyp. Location, size, number and base condition of the polyps were recorded before the patient underwent curettage. Hysteroscopy was then performed and the condition of the remaining polyps was compared with initial findings. Also, the remaining polyps were resected. SPSS 13 was used for statistical analysis.
Results: There were 51 patients in the study with a mean age of 33.14±8.19 years (range: 23-59 years). Besides, there were 82 polyps; 38(46.3%) having a narrow base, and 44(53.7%) having a wide base. The mean polyp size was 2.39±2.63cm.After performing curettage, 23(28.0%) polyps were removed completely, 39(47.6%) had size reduction, and 20(24.4%) had no change in size. Curettage could not significantly remove polyps (p<0.001).Polyps smaller than 2cm were more likely to have been removed compared to the bigger ones (p=0.003).Polyps with wide base were more significantly removed than those with narrow base (p<0.001).Further, those with wide base and also smaller than 2cm were removed more significantly than others (p<0.001).The location of polyps had no effect on removal probability by curettage (p=0.114).
Conclusion: Curettage was not found to be a reliable method for endometrial polyp removal. If hysteroscopy is not accessible, , the size of the polyp should be determined by vaginal sonograghy to estimate the probability of its removal by curettage.
Keywords: Endometrial polyp, Hysteroscopy, Dilatation and curettage, Polyp resection, Polyps/pathology, Polyps/surgery. (JPMA 65: 148; 2015).
Introduction
Normally, every woman periodically undergoes uterine bleeding in reproductive ages that lasts 4.7 days on average, and the amount of bleeding is around 35ml. Any kind of abnormal bleeding requires assessment and examination. Abnormal uterine bleeding is one of the common reasons for referral to gynaecology clinics and its conventional investigation methods include endometrial biopsy, diagnostic curettage and hysteroscopy.1
In the past, abnormal uterine bleeding was usually treated using curettage or hysterectomy and endometrial polyps were identified in histological analyses. Endometrial polyp is observed in 25% of patients with abnormal uterine bleeding, and from 1% to 12% (2.6%-3%) in asymptomatic women. Increased age during reproductive years is a risk factor for endometrial polyp, so that most amount of endometrial polyps is observed in women from 40 to 50 years of age (2.8%-7%). Also, prevalence of endometrial polyp is higher in women suffering from high blood pressure, overweight, uterine myoma and cervical polyp; average 8.2% (4%-13%).2 Although prevalence of malignancy in endometrial polyp is affected by factors like age and menopausal status, but this has been estimated to be 1% to 3%. Moreover, endometrial polyp could affect fertility results depending on its size, number and location, which is especially important in infertile patients.
Endometrial polyp is mostly diagnosed by trans-abdominal or trans-vaginal sonography (especially, sonohysterography), hysterosalpingography or hysteroscopy. Its definitive treatment is resection by hysteroscopy.
Unfortunately, in Iran, considering that hysteroscopy is not available in most hospitals and also most gynaecologists are not skilled enough in this field, endometrial polyps are often managed by curettage, which is an operation without direct view and a physician is not certain about definitive removal of polyps. Thus, if curettage cannot remove polyps completely, it will cause recurrent issues and may lead to invasive treatments such as hysterectomy, which can result in greater cost, mortality and morbidity. So, each patient with the diagnosis of endometrial polyp should be referred for hysteroscopy as a simple procedure with minimal complications and relatively low cost, while offering a definite treatment of the polyp.
On the other hand, curettage is considered an operation with less cost than hysteroscopy which could be performed with the least amount of facilities. Thus, if curettage is capable of completely removing endometrial polyps, extra costs and patient referral for hysteroscopy would be prevented.
Unfortunately, only few papers are available in this field and published data provide contradictory information. The current study was planned as an attempt to compare efficacy of curettage in endometrial polyp removal with hysteroscopy.
Subjects and Methods
The quasi-experimental pre-and-post study was conducted in 2011-12 at the gynaecology department of Imam Reza Hospital, Mashhad University of Medical Sciences, Iran, and comprised patients who underwent hysteroscopy for endometrial polyp.
The sampling method used was objective-based and field data collection method was applied. The data collection tool was observation-based checklist.
On the basis of literature3 the sample size with curettage sensitivity of 86.8% and 95% confidence interval (CI) was calculated to be 50 patients.
The study population comprised patients diagnosed with endometrial polyp during hysteroscopy without any other pathology. Those excluded were the ones with any pathology other than polyp in the uterine cavity, abnormal shape of uterine cavity, coagulation disorder, water and electrolyte disorder, patients with high anaesthetic risks, presence of active haemorrhage, lack of consent on the part of a patient and severe haemorrhage after the initiation of curettage.
All the patients were studied in terms of coagulation and electrolyte disorders; and the capability of general anaesthesia was assessed by an anaesthesiologist.
Before hysteroscopy, the process was verbally described to the patients and they signed informed consent forms. Curettage was free of charge for the patients. All demographic information including age, laboratory results, clinical symptoms and reason for referral was collected in a proforma. The patients underwent hysteroscopy by Olympus surgical hysteroscope with 7.5cm diameter and normal saline medium with pressure 100 to 110mmHg. Hysteroscopy was done under general anaesthesia in the lithotomy position. First, cervical dilation was done by metallic dilators (up to number 8). Then, the hysterscope was passed through the cervix. In case endometrial polyp was observed during hysteroscopy, the patient was included in the study. Number, size (<2cm or <2cm), location of polyps (according the location of its base in the uterine cavity) and the shape of their base (narrow or wide) were recorded. The polyp\'s size was measured by a scaled hysteroscope. Then, curettage was performed by a gynaecology resident in her 3rd or 4th academic year (expert in performing curettage) who had not seen the patient\'s hysteroscopy and was not aware of the location and number of polyps. The only knowledge on their part was about polyps in the uterus. In order to perform curettage, first ring forceps were used and then each uterine wall - anterior, posterior, right and left laterals -- was carved three times from the uterine fundus to the cervical internal ostium by curette number 5. In case the surgeon performing curettage found it necessary, one wall was carved more by the curette. Hysteroscopy was then performed again and location, size and number of the remaining polyps after curettage were recorded. The remaining polyps were completely removed by clamp, scissor or resectoscope during hysteroscopy. In case resectoscopy was needed, 1.5% glycine was used as medium. Performance of curettage added about 10 minutes to operation time and, depending on the number of polyps, variable haemorrhage resulted which was slight in most cases. In case operation time was needed to be shortened according to the anaesthesiologist\'s diagnosis, curettage performance was omitted and the patient was excluded from the study.
The collected data was analysed using SPSS 13 through Chi-square test. Confidence interval of 95% was considered statistically significant. P-value less than 0.05 was taken as statistically significant.
Results
There were 51 patients in the study with a mean age of 33.14±8.19 years (range: 23-59 years). The mean duration of menstruation cycle was 12.68±5.45 days. (range: 8-30 days) Mean number of pregnancies was 1.96± 0.86 (range: 0-12). Miscarriage existed in 12(23.53%) patients.
There were 82 polyps; 38(46.3%) having a narrow base, and 44(53.7%) having a wide base. The mean polyp size was 2.39±2.63cm. In terms of location in the uterus, 23 (28%) were located on posterior wall, 14 (17.1%) each on fundus and anterior walls, 11 (13.4%) on right lateral wall, 8(9.8%) on left lateral wall, 7 (8.5%) on left cornua and 5(6.1%) on right cornua.
After performing curettage, 23(28.0%) polyps were removed completely, 39(47.6%) had size reduction, and 20(24.4%) had no change in size. Curettage could not significantly remove polyps compared with hysteroscopy (p <0.001).
Polyps smaller than 2cm were more likely to have been removed compared to the bigger ones (p=0.003) (Table-1).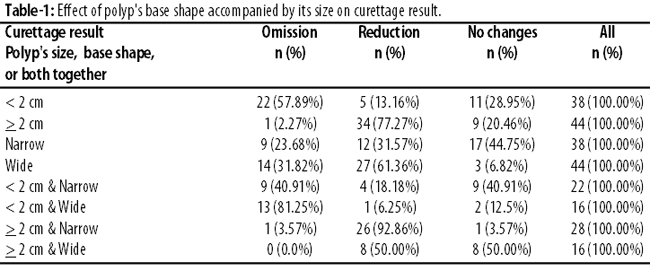
Polyps with wide base were more significantly removed than those with narrow base (p<0.001). Further, those with wide base and also smaller than 2cm were removed more significantly than others (p<0.001).
Among all polyps, 22(26.83%) were <2cm with narrow base, 16(19.51%) were <2cm with wide base, 16(19.51%) were >2cm with narrow base, and 28(34.15%) were >2cm with wide base. The chance of polyp removal was not significantly different among the four groups (p =0.23).
The location of polyps had no effect on removal probability by curettage (p=0.114) (Table-2).
The most common reason for patient referral was infertility 37(72.5%) (Table-3)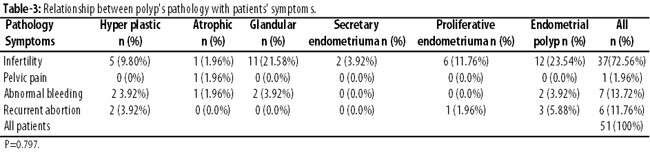
Pathology report of polyps in 17(33.4%) cases was only reported as endometrial polyp, which did not merit studying. Among the determined pathologies, glandular, hyperplastic, proliferative and atrophic were reported in 13(25.5%), 9(17.6%), 7(13.7%) and 3(5.9%) patients respectively. There were no relationship between the pathology of polyp and patient\'s complaint (p=0.797).
Discussion
The study tried to determine treatment efficacy of curettage on endometrial polyps.
In an earlier study, hysteroscopy was described as an accurate method for diagnosis and treatment of intrauterine pathology.4 Another study confirmed that hysteroscopy was more sensitive than dilation and curettage for studying endometrial cavity.5
In literature, hysteroscopy has been described as a healthy and effective method for diagnosis and treatment of intrauterine diseases and as the first maintenance treatment line for benign symptomatic diseases of the uterus.6
In the present study, hysteroscopy was used for diagnosing endometrial polyp. One study stated that, in spite of cost difference between fractional curettage with hysteroscopy, considering its significant failure, this method was not commonly recommended for diagnosing local uterine lesions and endometrial polyps.7 In contrast to the present study, one study comparing suction curettage, vaginal sonography and hysteroscopy to diagnose endometrial polyp, reported curettage as successful in more than 80% patients.8
One study introduced sonohysterography as an effective diagnostic tool for endometrial cavity lesions, especially when hysteroscopy was not available. These results were also confirmed by another study1 which demonstrated that diagnostic power of sonohysterography was comparable to that of hysteroscopy, and vaginal sonohysterography was a highly accurate, simple and fast diagnostic method without any complications. It was also recommended for primary assessment of patients suffering from abnormal haemorrhage.9 The same conclusion was confirmed by one other study.10 However, another study showed that hysteroscopy was superior to sonohysterography in diagnosis of uterine cavity lesions, especially because of providing simultaneous possibility for treatment.11 One study which compared sonohystrography with diagnostic curettage, sonohystrography was identified as a valuable method in studying abnormal uterine haemorrhage.12
In this study, curettage was not considered a reliable method for endometrial polyp removal, but there have been other studies stating success of curettage up to 68.8%.3 A critical review of literature concluded that resection of endometrial polyp by hysteroscope was the most effective treatment and provided accurate histological specimen, while blind curettage had low diagnostic and therapeutic value and was not recommended.13
In view of our findings, we recommend that if performing hysteroscopy is not possible, it is better to determine polyp size by doing more accurate diagnostic methods like sonohystography. If the size is smaller than 2cm, curettage could be used with high reliability. Otherwise, the patient should be made aware of the probability of incomplete removal of the polyp and possible relapse of symptoms followed by curettage.
Conclusion
Curettage could only remove 28% endometrial polyps and was not a reliable method. If hysteroscopy is possible, endometrial polyp treatment should be definitely done by hysteroscopy to ensure complete removal.
Acknowledgments
We are grateful to the Vice-Chancellor of research and Women\'s Health Research Centre, Mashhad University of Medical Sciences, for financial and material support, and to all those who helped us in this paper which is based on a gynaecology residency thesis.
References
1. Kimiaei P, kalantari M. Efficacy of vaginal sonohystrography in the diagnosis of uterine abnormalities. Pejouhandeh Quart Res J 2000; 5:77-83.
2. Dordevic B, Milosevic J, Stanojevic Z. Prevalence and characteristics of endometrial polyps in patients with abnormal uterine bleeding. Vojnosanitetski pregled Military-medical and pharmaceutical review 2008;65:349-52.
3. Liberis V, Dafopoulos K, Tsikouras P, Galazios G, Koutlaki N, Anastasiadis P, et al. Removal of endometrial polyps by use of grasping forceps and curettage after diagnostic hysteroscopy. Clinic Experiment Obstet Gynecol 2003; 30: 29-31.
4. Vahdat M, Aghaee M, Amin S. The Survey on Ten Years Management with Hysteroscopyof Patients referred to Rasool Akram Teaching Hospital in Tehran. Iran J Obstet Gynecol Infertil 2009;12:1-6.
5. Bedner R, Rzepka-Gorska I. Hysteroscopy with directed biopsy versus dilatation and curettage for the diagnosis of endometrial hyperplasiaand cancer in perimenopausal women. Europ J Gynaecol Oncol 2007;28:400-2.
6. Sayyah Melli M, Nazer L. Hysteroscopic evaluation and treatment of uterine diseases in 301 patients. Med J Tabriz Univ Med Sci 2006; 28:71-6.
7. Moradan S, Ghorbani R, Zanganeh M. Comparison of Fractional D&C with uterine Pathology in Determining the Causes of Abnormal Uterine Bleeding in women of Premenopausal and Postmenopausal Stage. Iran J Obstet Gynecol Infertil 2006; 9:73-8.
8. Maia H, Maltez A, Calmon LC, Marques D, Oliveira M, Coutinho E. Comparison between suction curettage, transvaginal sonography and hysteroscopy for the diagnosis of endometrial polyp. Gynaecol Endoscop 1998; 7:127-32.
9. Anastasiadis PG, Koutlaki NG, Skaphida PG, Galazios GC, Tsikouras PN, Liberis VA. Endometrial polyps: prevalence, detection, and malignant potential in women with abnormal uterine bleeding. Europ J Gynecol Oncol 2000; 21:180-3.
10. Yildizhan B, Yildizhan R, Ozkesici B, Suer N. Transvaginal ultrasonography and saline infusion sonohysterography for the detection of intra-uterine lesions in pre- and post-menopausal women with abnormal uterine bleeding. J Int Med Res 2008; 36:1205-13.
11. Soguktas S, Cogendez E, Kayatas SE, Asoglu MR, Selcuk S, Ertekin A. Comparison of saline infusion sonohysterography and hysteroscopy in diagnosis of premenopausal women with abnormal uterine bleeding. Eur J Obstet Gynecol Reprod Biol 2012;161:66-70.
12. Hajishafieha M, Zobeiri T, Boroomand F, Oroji R, Rajabpoor M. A comparative study of sonohysterography with diagnostic curettage in patients with abnormaluterine bleeding. Urmia Med J 2006; 17:181-7.
13. Salim S, Won H, Nesbitt-Hawes E, Campbell N, Abbott J. Diagnosis and anagement of endometrial polyps: a critical review of the literature. J Minim Invasive Gynecol 2011;18:569-81.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: