
Seyfettin Ciftci ( Department of Urology, University of Kocaeli, Kocaeli, Turkey. )
Bahattin Ozkul ( Department of Radiology, University of Kocaeli, Kocaeli, Turkey. )
Murat Ustuner ( Department of Urology, University of Kocaeli, Kocaeli, Turkey. )
NagihanInan ( Department of Radiology, University of Kocaeli, Kocaeli, Turkey. )
Mustafa Melih Culha ( Department of Urology, University of Kocaeli, Kocaeli, Turkey. )
December 2014, Volume 64, Issue 12
Case Reports
Abstract
Gunshot wound injury to the external genitalia is relatively uncommon. However, if a testis is affected in such a case, early surgical exploration should be carried out. A 16-year-old boy presented with right testicular rupture. Tunica albugineal defect could not be closed primarily. We used a Tutoplast® processed bovine pericardium to repair the defect of tunica albuginea. At his 3-month follow-up visit, there was no complication. Doppler blood flow of testis was normal. In this case, preservation of testis tissue was obtained with early exploration and repair of the big tunica albugineal defect with Tutoplast® processed pericardium.
Keywords: Testis trauma, Tunica albuginea defect, Processed pericardium.
Introduction
Gunshot wound injury (GWI) of testis is relatively rare.1 However, in case of such an injury, tunica albuginea of testis is probably damaged and needs repair. Testis rupture, also known as fractured testis, is tear of the tunica albuginea resulting in the extrusion of the seminiferous tubules. Rupture of testis is an emergent situation because of infection and the risk of a testis loss, and surgical exploration is needed in most cases.2 Sometimes, extruded seminiferous tubules and large tissue defect of tunica albuginea do not allow primary closure of the testis. A viable testis should be salvaged by covering a graft over the defect to preserve hormonal status. We present a case of GWI of the right testis with a big tunica albugineal defect that could not be closed primarily and had to be repaired with Tutoplast® (Tutopatch®, Tutogen Medical GmbH, Germany) processed bovine pericardium successfully.
Case Report
A 16-year-old male patient presented to the emergency department after a GWI of the penis, right testis and thigh with a low-velocity handgun. He had no previous medical history. The patient expressed extreme pain and swollen tender right testis and penis. Physical examination revealed swelling, bruising and tenderness of the right hemiscrotum and also haematoma and ecchymosis on the penis. The entrance wounds of the bullets were on the right dorsolateral aspect of penis and lateral aspect of right hemiscrotum. Exit wounds were located on the left lateral aspect of the penile shaft and anterior aspect of right hemiscrotum. There were also 2 entrance and 2 exit wounds on lateral and medial aspects of the right upper thigh, respectively. The left testis was normal. A scrotal Doppler ultrasonography scan (DUSS) revealed a haematoma in the right hemiscrotum and a heterogeneous echogenicity of the right testis with a good vascular flow of both testes. However, it was insignificant about rupture of tunica albuginea. All laboratory parameters were unremarkable.
The patient underwent a corporal repair of penis and exploration of right hemiscrotum through a transvers scrotal incision. There was haematoma, ruptured tunica albuginea and extruded seminiferous tubules in the right hemiscrotum. Haematoma was evacuated, but the ruptured testis could not be closed primarily because extruded seminiferous tubules and a big tissue defect of tunica albuginea did not allow the apposition of the tunica albugineal edges. All nonviable extruded seminiferous tubules were excised. A graft of Tutoplast® (Tutopatch®, Tutogen Medical GmbH, Germany) processed bovine pericardium was wrapped around the extruded seminiferous tubules and sewn to the free edges of the tunica with 4.0 absorbable sutures (Figure-1).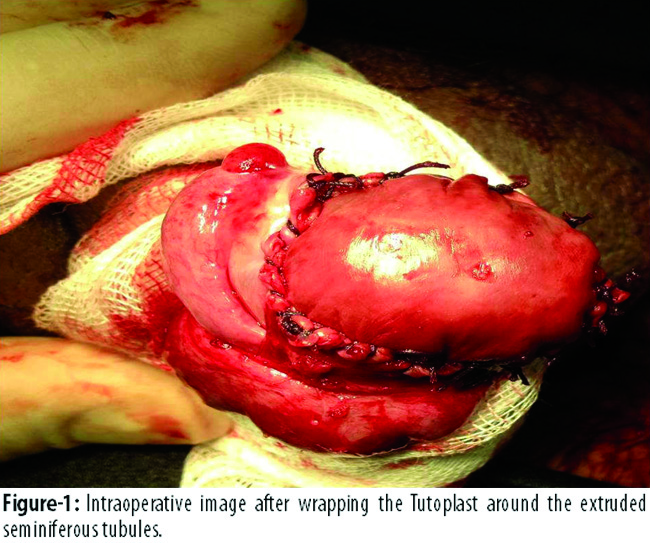
Dartos and then skin were closed separately without drainage catheter. The patient was discharged at postoperative day 2 without any complication.
Follow-up DUSS at first month showed a viable testis with no atrophic changes. At postoperative third month, DUSS demonstrated a good arterial blood flow (Figure-2A)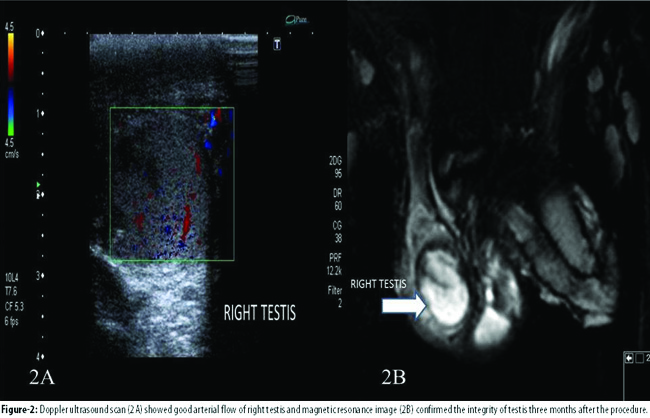
and magnetic resonance imaging (MRI) revealed normal integrity and volume of the right testis (Figure-2B). Physical examination was also normal. No complications were detected during the follow-up period.
Discussion
Severe injuries of the external genitalia of male are rare due to the well-protected location and high-degree mobility of the penis and the testes. The peak incidence of the scrotal trauma is between the years of 15 and 40, and also it accounts for only less than 1% of all traumatic injuries.3 GWI of the external genitalia of the male are also very uncommon.1 However, if scrotum has been affected with a GWI, tunica albuginea of the testis may be ruptured. Early exploration has a higher testis salvage rate compared to the delayed.4 Delay of diagnosis can cause irreversible damage to the testes. Conservative management has a high risk of complications, such as infection, causing orchiectomy or testicular atrophy.5 Viable testicular tissue should be salvaged to preserve endocrine function. However, orchiectomy is needed when the testis is completely shattered or avulsed.
After diagnosis or strong suspicion of testis rupture, early surgical exploration and repair of the testis should be performed. In some cases, big defect of tunica albuginea or extruded seminiferous tubules could not allow the apposition of the edges of the testis capsule. In such cases, organic or synthetic graft has to be used to cover the defect. In case of viable extruded seminiferous tubules achieving closure of the testis capsule, tunica vaginalis can be used to wrap around the extruded tubules and can be sewn with absorbable sutures. In literature, we are aware of only a few publications that demonstrate the use of tunica vaginalis as a graft to repair the disrupted testis.6-9 Free tunica vaginalis grafts have been described and give a better outcome than synthetic grafts.6,7 One study6 reported repair of 9testicular rupture cases. In 2 of them, a polytetrafluoroethylene Gore-Tex patch graft was used to cover the tunica albugineal defect, but both the testes became infected. In the remaining 7 patients, a free graft of tunica vaginalis was harvested and sewn to the edges of tunica albuginea. At two weeks after the operation, all the 7 patients had normal blood flow on DUSS. However, only 4 of them had normal arterial blood flow on DUSS at the third-month follow-up. So, the study recommended the use of free graft of tunica vaginalis and to avoid the use of synthetic grafts due to high risk of infection. We did not see any infection of the testis or graft and arterial blood flow of the affected testis was normal at the first and third months of follow-up. Furthermore, success of the tunica vaginalis graft is limited because of the lack of intrinsic blood supply. There are 2 publications that recommend the use of vascularised tunica vaginalis graft.8,9 One of them8 reported an adult case of testicular rupture that was repaired with vascularised tunica vaginalis graft successfully. The other study9 also used the same technique in a 16-year-old paediatric patient successfully. Tunica vaginalis may be a good alternative to wrap the extruded seminiferous tubules and repair the tunica albuginea. However, free graft of tunica vaginalis may be devitalised and lead to infection and loss of testis. Vascularised graft of tunica vaginalis may be a solution to this problem, but there is not sufficient data that support it. Furthermore, there is not sufficient data that has long term follow-up period.
The use of Tutoplast® was first described by a study in the surgical management of the Peyronie\'s disease.10 After that, Tutoplast® has been described in penile surgeries by other authors.11,12 However, we could not find any publications that demonstrate its use to repair the defect of tunica albuginea of testis.
One study10 did not define any infection and rejection in their series. Another13 reported 40 patients with Peyronie\'s disease and they were repaired with human cadaveric pericardial graft. It did not report any complication of graft-related adverse events with 22-month follow-up period. Other studies11,14,15 have published the long-term results of Tutoplast graft in the correction of Peyronie\'s disease. There were no reported complications in any of the series. In contrast, there is a reported case of Tutoplast-related graft contraction and inclusion cyst in a 40-year-old male 18 months after the correction of penile curvature with Tutoplast.16 In addition, only one bovine pericardium-related foreign body reaction was reported in a child after chordee repair.17 To our knowledge, there is no other rejection or foreign body reaction related to the Tutoplast in penile surgery even in long-term studies. During short-term follow-up, we did not see infection, rejection or contraction related to the graft in our case.
In this report, we described the use of Tutoplast® as an alternative graft to cover the big defect of tunica albuginea that did not allow the apposition of the testis capsule. To our knowledge, this is the first report of this technique for the management of testicular rupture. Furthermore, it was a paediatric patient and testis needed to be preserved because of a long life expectancy. After 3 months of the operation, the patient was asymptomatic and there was no evidence of any complication. Furthermore, volume of the affected testis did not decrease in comparison to the other side. Integrity and blood flow of the testis were normal 3 months after the surgery.
Conclusion
The use of Tutoplast® processed pericardium has not been demonstrated in testicular surgery. To our knowledge, this is the first case in literature of testis rupture that was repaired with Tutoplast cadaveric pericardium. The use of Tutoplast® should be kept in mind in testicular rupture cases when tunica albuginea may not be closed primarily because of big defect. This technique may represent a valuable adjunct in managing major testicular ruptures.
References
1. Brandes SB, Buckman RF, Chelsky MJ, Hanno PM. External genitalia gunshot wounds: a ten-year experience with fifty-six cases. J Trauma 1995; 39: 266-71.
2. Bandi G, Santucci RA. Controversies in the management of male external genitourinary trauma. J Trauma 2004; 56: 1362-70.
3. Buckley JC, McAninch JW. Use of ultrasonography for the diagnosis of testicular injuries in blunt scrotal trauma. J Urol 2006; 175: 175-8.
4. Cass AS. Testicular trauma. J Urol 1983; 129: 299-300.
5. Chandra RV, Dowling RJ, Ulubasoglu M, Haxhimolla H, Costello AJ. Rational approach to diagnosis and management of blunt scrotal trauma. Urology 2007; 70: 230-4.
6. Ferguson GG, Brandes SB. Gunshot wound injury of the testis: the use of tunica vaginalis and polytetrafluoroethylene grafts for reconstruction. J Urol 2007; 178: 2462-5.
7. Kapoor D, Leech J, Yap W. Use of tunica vaginalis patch graft for repair of traumatic testicular rupture. Urology 1992; 40: 374-5.
8. Molokwu CN, Doull RI, Townell NH. A novel technique for repair of testicular rupture after blunt trauma. Urology 2010; 76: 1002-3.
9. Jian PY, Nelson ED, Roth DR. Use of a vascularized tunica vaginalis flap for repair of testicular rupture in a pediatric patient. Urology 2012; 79: 1363-4.
10. Hellstrom WJ, Reddy S. Application of pericardial graft in the surgical management of Peyronie\'s disease. J Urol 2000; 163: 1445-7.
11. Palese MA, Burnett AL. Corporoplasty using pericardium allograft (tutoplast) with complex penile prosthesis surgery. Urology 2001; 58: 1049-52.
12. Leungwattanakij S, Bivalacqua TJ, Reddy S, Hellstrom WJ. Long-term follow-up on use of pericardial graft in the surgical management of Peyronie\'s disease. Int J Impot Res 2001; 13: 183-6.
13. Levine LA, Estrada CR. Human cadaveric pericardial graft for the surgical correction of Peyronie\'s disease. J Urol 2003; 170: 2359-62.
14. Usta MF, Bivalacqua TJ, Sanabria J, Koksal IT, Moparty K, Hellstrom WJ. Patient and partner satisfaction and long-term results after surgical treatment for Peyronie\'s disease. Urology 2003; 62: 105-9.
15. Chung E, Clendinning E, Lessard L, Brock G. Five-year follow-up of Peyronie\'s graft surgery: outcomes and patient satisfaction. J Sex Med 2011; 8: 594-600.
16. Thiel DD, Broderick GA, Wu KJ. Inclusion cyst and graft contraction in Tutoplast human cadeveric pericardium following Peyronie\'s grafting: a previously unreported complication. Int J Impot Res 2005; 17: 550-2.
17. Pais VM Jr, Jiang Z, Fung LC. Foreign body reaction to bovine pericardium: a previously unreported complication of pediatric chordee repair. J Urol 2002; 168: 702-3.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: