
Ali Khawaja ( Medical College, The Aga Khan University Hospital, Karachi, Pakistan. )
Hira Shahzad ( Medical College, The Aga Khan University Hospital, Karachi, Pakistan. )
Murtaza Kazmi ( Section of Pulmonary and Critical Care Medicine, Department of Medicine, The Aga Khan University Hospital, Karachi, Pakistan. )
Ali Bin Sarwar Zubairi ( Section of Pulmonary and Critical Care Medicine, Department of Medicine, The Aga Khan University Hospital, Karachi, Pakistan. )
November 2014, Volume 64, Issue 11
Original Article
Abstract
Objective: To evaluate the clinical course and outcomes in patients with acute severe asthma in a tertiary care setting.
Methods: The retrospective cross-sectional study was conducted at the Aga Khan University Hospital, Karachi, and comprised data of patients of age 16 and above who were admitted with a diagnosis of acute severe asthma from January 2000 to December 2013.These patients had undergone clinical evaluation to assess the severity of illness as well as the complications and eventual outcomes. SPSS 16 was used for statistical analysis.
Results: Of the 50 patients in the study, 41 (82%) were females. The overall mean age was 53.1±20.3 years. Ventilator support was required by 37(74%) patients. Presence of acidaemia was associated with the need for invasive ventilation (p<0.033) which in turn was associated with increased hospital stay (p<0.043). Complications were observed in 37(74%) patients, the most common being respiratory failure in 35(70%) and arrhythmias in 8(16%). Use of both non-invasive and invasive ventilation was found to be significantly associated with development of complications (p<0.001and p<0.009). A total of 4(8%) patients died. Presence of acidaemia was found to be significantly associated with mortality (p<0.032).
Conclusion: Overt acidaemia at initial presentation in patients with acute severe asthma was significantly associated with higher rates of invasive ventilation leading to increased hospital stay, complications and higher mortality rate.
Keywords: Acute asthma, Severe asthma, Adults. (JPMA 64: 1292; 2014)
Introduction
Asthma is a chronic inflammatory condition of the airways characterised by symptoms of reversible airflow obstruction and bronchospasm. Despite recent advances in the diagnosis and treatment, the prevalence of asthma has increased in the last two decades, leading to increased morbidity and utilisation of resources.1,2 According to the Centre for Disease Control and Prevention (CDC), the proportion of people with asthma has increased by 15% in the United States and accounts for around $56 billion every year.3 Around 10% of the world\'s population is currently suffering from asthma, 5% of which is classified as severe disease.4 It is considered to be a public health problem all over the world. However, higher rates of mortality have been observed in low and lower-middle income countries.2 This may be attributed to multiple risk factors such as poor compliance, incorrect perception of the use of inhalers, non-affordability of medications, lack of follow-ups, non-availability of healthcare facilities and overall lower socioeconomic status and level of education.2,5,6
Acute severe asthma, previously known as status asthmaticus, is defined as an asthma exacerbation which is unresponsive to the conventional treatment with bronchodilators and steroids, leading to respiratory failure that can be potentially fatal.7,8 It accounts for one of the most common causes of visits to the emergency department (ED) and around one-fifth of all the episodes managed in urgent care centres are considered to be severe.7 Hence, failure to recognise the severity and delay in treatment may lead to high rates of morbidity and mortality. Patients with acute severe asthma may require intensive care monitoring, mechanical ventilation and prolonged hospitalisation, resulting in further economic burden especially in developing countries. Furthermore, these patients are at risk for developing serious and often fatal complications, including asphyxia due to mucus plugging, pneumo-thorax, pneumo-mediastinum, pneumo-pericardium, cardiac arrhythmias, electrolyte and metabolic disturbances and even myocardial infarction (MI) and anoxic brain injury.7,9,10
Knowledge regarding predictors of morbidity and mortality in these patients is, therefore, imperative in making decisions regarding initial management, treatment during hospital stay and follow-up. Although much work has been done in assessing the clinical course and outcomes of patients with acute severe asthma, majority of the data available is from the Western population, while data from South Asia remains scarce. The aim of this study was to review the clinical course, prognostic factors, complications and outcomes in patients with acute severe asthma in our setting.
Patients and Methods
The retrospective cross-sectional study was conducted at the Aga Khan University Hospital (AKUH), Karachi, and comprised patient data from January 2000 till December 2013. AKUH is a major tertiary care hospital serving more than 10 million people of Karachi and the surrounding region. With an operational strength of 650 beds, the facility serves over 42,000 in-patients and over 500,000 out-patients annually. Established since 1985, it is one of the few teaching hospitals in South Asia accredited with the Joint Commission for International Accreditation.
The medical record numbers of patients are saved and coded according to the diagnoses at the institution. After obtaining approval from the institutional ethics committee and in compliance with the International Helsinki Declaration, data of all patients of age 16 years and above who were admitted with the diagnosis of acute severe asthma was extracted using the medical record numbers. All the patients had been admitted either to a \'high dependency unit (HDU)\' or an \'intensive care unit (ICU)\'.Patients who were less than 16 years of age or had underlying lung diseases, including chronic obstructive pulmonary disease (COPD), bronchiectasis and interstitial lung disease (ILD), were excluded an so were patients who had a history of smoking for more than 10 pack years.
The recorded data included demographics of the patients including age, gender and co-morbid conditions, while clinical parameters included patients\' medications and arterial blood gases (ABG) at the time of presentation, use and type of mechanical ventilation, the course and length of hospital stay, complications and eventual outcome of the patient. Acute physiology and chronic health evaluation (APACHE) II scores were calculated in order to assess the severity of the illness.11
Statistical analysis was conducted using SPSS 16.Descriptive analysis was performed for demographic and clinical characteristics and results were presented as mean ± standard deviation (SD) for quantitative variables and frequencies and percentages for qualitative variables. The differences in baseline characteristics between different groups were assessed by using the Chi-square test or Fisher exact test where appropriate, whereas for contrasts of continuous variables, independent sample t-test was used to assess the difference of means. The p-values were two sided and <0.05 was considered statistically significant.
Results
Of the 50 patients in the study, 41(82%) were females. The overall mean age was 53.1±20.3 years. The mean pH value at the time of presentation was 7.33±0.11 (range: 6.96 - 7.56). Respiratory acidosis (pH<7.35) was observed in 22(44%) patients (Table-1).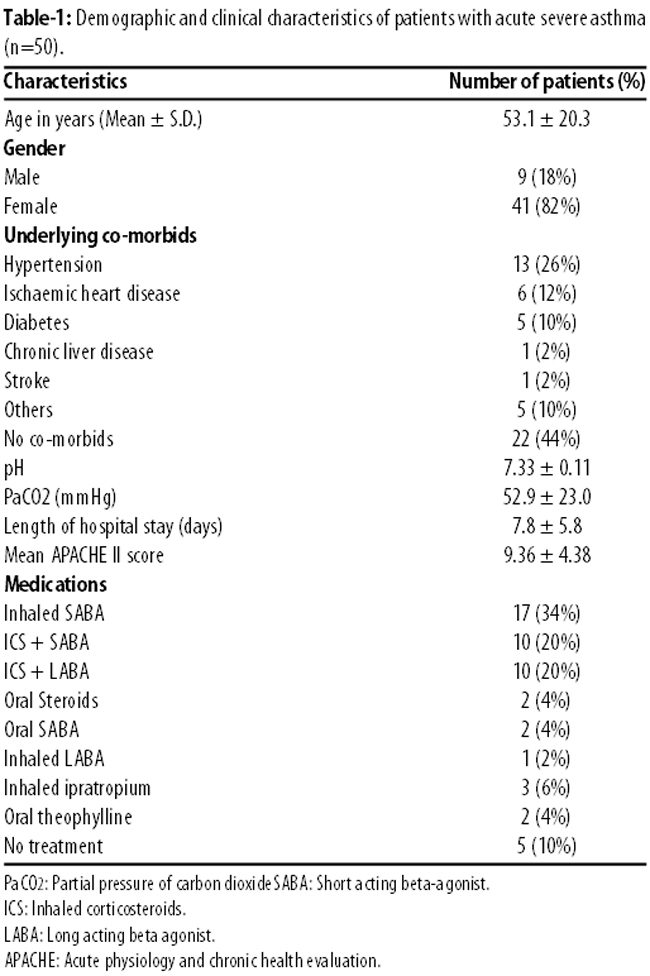
Of the total, 37(74%) patients required ventilator support; 18(36%) required non-invasive ventilator support, while 19(38%) needed intubation. Five (10%) patients who were initially intubated required non-invasive ventilator support following extubation. Presence of acidaemia was significantly associated with the need for invasive ventilation (p<0.033). The mean duration of hospital stay was higher in patients who required ventilator support as compared to those who did not (Table-2).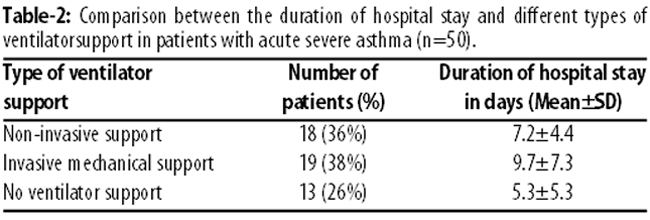
Complications were observed in 37 (74%) patients, the most common being respiratory failure in 35(70%), arrhythmias in 8(16%) and sepsis in 5(10%) patients, while pneumothorax occurred in 1(2%) patient. The rate of development of complications was higher in patients with a higher APACHE II score (Table-3).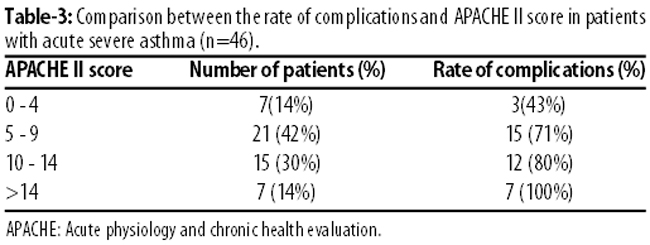
Four (8%) patients died during the hospital stay; 2(4%) because of sepsis, 1(2%) due to acute MI with resulting cardiac arrest, and 1(2%) due to respiratory failure (Table-4).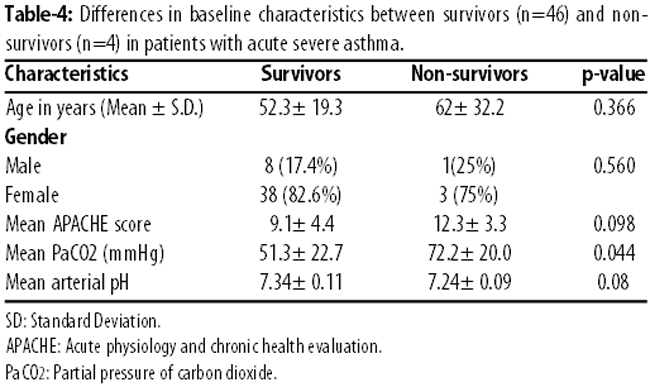
Mean Partial pressure of carbon dioxide (PaCO2) was significantly higher in non-survivors (p<0.044), while although pH was lower in patients who did not survive, this was not statistically significant (p<0.08).
The use of both non-invasive and invasive ventilator support was significantly associated with developing complications (p<0.0001 and p<0.009) while invasive ventilator support was significantly associated with a hospital stay of more than 7 days (p<0.032) (Table-5).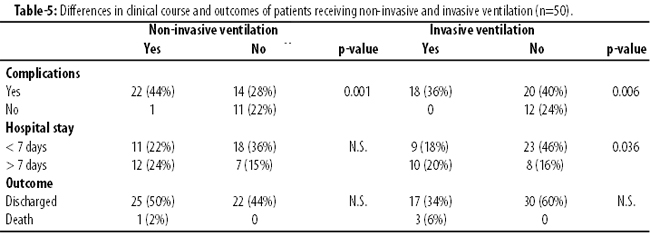
Discussion
Asthma is a common disease and its incidence is expected to rise in the next few decades. Although only 5% of the asthmatics are considered to have severe disease, but they account for almost 60% of the allotted budget to asthma.4,12 To the best of our knowledge, this is the first study to be reported on clinical outcomes of acute severe asthma in our patient population.
In the current study, presence of acidaemia on initial presentation was a significant predictor of poor prognosis. It was associated with the need for intubation and longer duration of hospital stay leading to complications and mortality. Similar findings in patients admitted to ICU with severe asthma have been observed in the literature. A study reported a higher level of PaCO2 (63.8±21.3 vs 47.8±19.1mm Hg; p<0.01) and a lower pH (7.09±0.12 vs 7.27±0.12; p<0.0001) in non-survivors compared to the survivors9 while another study reported hypercapnea to be an independent factor associated with in-hospital mortality (Odds Ratio [OR]: 1.62; 95% Confidence Interval [CI]: 1.37-1.91).13 Another study also reported higher rate of mechanical ventilation requirement in patients with lower arterial pH (p<0.001) which was also related to a high mortality rate.14
Invasive mechanical ventilation was needed in 37% patients while the mortality rate in the present study was 6.5% which is comparable to previously reported studies. The in-hospital mortality for all asthmatics has been reported to be around 1% to 5%15 while it varies widely between 0% and 40% for patients with severe asthma requiring mechanical ventilation.9,13-18 The wide variation is most likely due to the differences in the level of healthcare facilities, differences in approach by the physicians over time and the fact that different patient populations have been reported in these studies.
In our study, three of the non-survivors were females whereas only one was male. Although this did not reach statistical significance, but this was attributed to the small sample size and majority of our patient population being females. Female gender predilection in acute severe asthma, however, has been reported in the past.9,13,18 This might be due to a possibility that the pathogenesis of severe asthma depends on gender-specific hormonal, anatomical and biochemical factors.13,19 Furthermore, differences in the perception of dyspnoea and severity might also vary between the two genders with males presenting later in the course of the disease as compared to their female counterparts.20
The most common complications encountered in our patients were respiratory failure, sepsis and arrhythmias. Sepsis and acute respiratory distress syndrome (ARDS) have been encountered as frequent complications in patients admitted to the ICU with severe asthma.13,15 Furthermore, pneumothorax and non-pulmonary organ failure are also not uncommon.13,15 However, the latter were not encountered in our patients frequently. Complications were more frequent in patients who required mechanical ventilation possibly because it runs the risk of causing barotrauma to the lung parenchyma. Complications lead to increased duration of hospital stay which in turn puts the patients at risk for developing nosocomial infections and, hence, sepsis.
It is important to assess the severity of illness in order to make appropriate decisions regarding therapeutic management and determining the outcome of the patient. APACHE II scores have been used to predict the clinical outcome in patients admitted to the ICUs in the past with higher scores predicting poorer prognosis.11 Earlier studies reinforced the utilisation of this score in patients with severe asthma and reported increased duration of hospital stay and high mortality rate with higher APACHE II score.9,21 Although our results did not reach statistical significance, mean APACHE II score was found to be higher in non-survivors. Further prospective studies from our setting would better assist in determining the usefulness of this score in patients with acute severe asthma.
There are several limitations of this study. Firstly, the sample size was relatively smaller compared to previous studies. However, this was inherent due to the stringent inclusion criteria in which long-term smokers and patients with COPD were excluded. Although this reduced the sample size, the potential confounding factor of COPD as discussed earlier13 was eliminated. Furthermore, exclusion of these patients might also be a contributing factor to a high proportion of females in this study since smoking is more common in the males in our society. Secondly, due to the retrospective nature of the study, multiple risk factors such as level of education, socioeconomic status, perception of medications and prognostic factors such as ventilator parameters could not be evaluated. Lastly, this was a single-centre study and could not be generalised to the entire population.
Conclusion
Mortality related to acute severe asthma remains a concern. Presence of overt acidaemia at initial presentation is associated with a need for mechanical ventilation which is in turn associated with a longer duration of stay at the hospital and development of complications. Presence of acidaemia also leads to a poorer prognosis and higher mortality rate. However, prospective studies with larger study populations are needed to further validate the findings.
References
1. To T, Stanojevic S, Moores G, Gershon AS, Bateman ED, Cruz AA, et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health 2012; 12: 204.
2. The Global Asthma Report 2011. Paris, France: The International Union. Against Tuberculosis and Lung Disease, 2011.
3. Asthma\'s Impact on the Nation. Data from the CDC National Asthma Control Program. (Online) (Cited 2013 February 24). Available from URL: http://www.cdc.gov/asthma/impacts_nation/AsthmaFact Sheet.pdf.
4. Dennis RJ, Solarte I, Rodrigo G. Asthma in adults. Clin Evid (Online) 2011; pii: 1512.
5. Lee PY, Khoo EM. How well were asthmatic patients educated about their asthma? A study at the emergency department. Asia Pac J Public Health 2004; 16: 45-9.
6. Al-Jahdali H, Anwar A, Al-Harbi A, Baharoon S, Halwani R, Al Shimemeri A, et al. Factors associated with patient visits to the emergency department for asthma therapy. BMC Pulm Med 2012; 12: 80.
7. McFadden ER Jr. Acute severe asthma. Am J Respir Crit Care Med 2003; 168: 740-59.
8. Papiris SA, Manali ED, Kolilekas L, Triantafillidou C, Tsangaris I. Acute severe asthma: new approaches to assessment and treatment. Drugs 2009; 69: 2363-91.
9. Afessa B, Morales I, Cury JD. Clinical course and outcome of patients admitted to an ICU for status asthmaticus. Chest 2001;120: 1616-21.
10. Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical review: severe asthma. Crit Care 2002; 6: 30-44.
11. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985; 13: 818-29.
12. Siddiqui S, Gonem S, Wardlaw AJ. Advances in the management of severe asthma. Semin Respir Crit Care Med 2012; 33: 666-84.
13. Gupta D, Keogh B, Chung KF, Ayres JG, Harrison DA, Goldfrad C, et al. Characteristics and outcome for admissions to adult, general critical care units with acute severe asthma: a secondary analysis of the ICNARC Case Mix Programme Database. Crit Care 2004; 8: R112-21.
14. Stow PJ, Pilcher D, Wilson J, George C, Bailey M, Higlett T, et al; Australian & New Zealand Intensive Care Society Adult Patient Database Management Committee. Improved outcomes from acute severe asthma in Australian intensive care units (1996-2003). Thorax 2007; 62: 842-7.
15. Louie S, Morrissey BM, Kenyon NJ, Albertson TE, Avdalovic M. The critically ill asthmatic--from ICU to discharge. Clin Rev Allergy Immunol 2012; 43: 30-44.
16. Braman SS, Kaemmerlen JT. Intensive care of status asthmaticus: a 10 year experience. JAMA 1990; 264: 366-8.
17. Webb AK, Bilton AH, Hansen GC. Severe bronchial asthma requiring ventilation: a review of 20 cases and advice on management. Postgrad Med J 1979, 55: 161-70.
18. Mirza TA, Fillimban A, Maimini O, Khiyat EY, Dhafar KO, Farooq MU, et al. Predictors of asthma severity during the pilgrimage to Mecca (Hajj). Pol Arch Med Wewn 2011; 121: 327-31.
19. Skobeloff EM, Spivey WH, St. Clair SS, Schoffstall JM. The influence of age and sex on asthma admissions. JAMA 1992, 268: 3437-40.
20. Rubinfeld AR, Pain MCF. Perception of asthma. Lancet 1976; 24: 882-4.
21. Gehlbach B, Kress JP, Kahn J, DeRuiter C, Pohlman A, Hall J. Correlates of prolonged hospitalization in inner-city ICU patients receiving noninvasive and invasive positive pressure ventilation for status asthmaticus. Chest 2002; 122: 1709-14.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: