
Bibi Nooreen Begum ( Institute of Clinical Psychology, University of Karachi, Pakistan. )
Shazia Hasan ( Humanities Department, COMSAT Institute of Information Technology, Lahore, Pakistan. )
November 2014, Volume 64, Issue 11
Original Article
Abstract
Objective: To explore the difference between anxiety and depression among infertile and fertile women.
Methods: The study was conducted in 2009 and comprised fertile and infertile women. The sample of infertile women was drawn from the Liaquat National Hospital, Patel Hospital, Infertility Concept and Zainub Hospital, located in urban areas of Karachi, while fertile women were drawn from the general population in urban Karachi. All the subjects had at least 10 years of education and were in the age range of 20-35 years. They two groups were further divided into two sub-groups of working and non-working women. Institute for Personality and Ability Testing Depression and Anxiety scales were used to assess depression and anxiety. SPSS 14.0 was used to analyse the data.
Result: Of the 120 subjects, the two groups had 60(50%) each. The mean age of fertile women was 27.48±160.75 and that in the infertile group was 27.36±160.75. Depression among fertile women was 21.85±10.98 compared to 32.01±12.49 among the infertile women. Corresponding values for anxiety was 24.45±9.63 and 36.20±12.51.The difference was significant.
Conclusion: Women with infertility experience a greater psychological impact.
Keywords: Fertility, Infertility, Anxiety, Depression. (JPMA 64: 1287; 2014).
Introduction
Reproducing and upbringing of children has been a part of life since the beginning of mankind, and it became more strengthened throughout history by way of myths, religions, cultures, traditions, arts and literature. Parenthood and children are incontrovertibly among the most desired goals and life plans in adulthood universally. Motherhood is an important and different aspect of life for many of the mothers in different social and personal areas of their lives.1
Surveys in the community worldwide have used duration of marriage ranging from one year to five years to set up infertility.2 However, the recommended definition that is functional in research and in clinical practice with respect to different perspectives is the one proposed by World Health Organisation (WHO). Infertility, according to WHO, is based on 24 months of struggle to get pregnant.3
There are some theories related to infertility such as Grief and Bereavement theory. Grief and loss is the result of infertility. Not having children leads to losses such as the loss of individual; physical and mental well-being of couples; life goals, position, reputation, regard, self-confidence; and loss of privacy and grief.4 Another theory includes chronic infertility-specific grief model5 objecting to the principle of conventional grief and loss theory to infertility because it does not address the long-term infertility problem with persistence. It acknowledged infertility as a chronic sorrow for the individual with infertility, characteristically involving abundant losses for a wide range and longer period of time.
When we are talking about the rate of infertility throughout the world, WHO estimated between 60 million and 168 million in 1994; and one in ten couples usually has primary or secondary infertility.6 Majority of such people live in the developing world.7 As far as prevalence of infertility is concerned, its rate is high up to 21.9%; primary infertility 3.5% and secondary infertility 18.4%.8 It is generally accepted that infertility rates are not estimated correctly. Some of the reasons could be hindrances faced to measure the prevalence; imperfect measurement methods; and unknown kinds of the condition of infertility in the result of cultural biases.9
There are various causes of infertility and are mainly derived from preventable causes, physiological dysfunctions and issues that are not explained. Few of the causes that contribute to infertility10 are endocrineological, anatomical, genetic and immunological reasons.9 A study carried out on 8500 infertile couples by WHO indicates 37 percent female factor in developed countries among infertile couples, 8 percent male factor infertility, and 35 percent is the combination of male and female factor infertility.10 Some of the causes of infertility prevalence other than physiological conditions include factors of lifestyle, infection, environmental and occupational hazards and advancing maternal age.9 Excessive exercise, obesity, weight-loss, weight-gain, eating disorders, malnutrition, and caffeine, alcohol or nicotine consumption are included in the lifestyle factors that play a crucial role in preventing infertility.
Infertility-affects individual\'s different domains of life such as personal life, societal aspect and also intimate relationships. The experience of infertility affects psychological life of an individual most frequently and these effects are mentioned in the empirical researches and literature as emotional reactions, psychological distress, feelings of loss of control, effect on self-esteem, identity, and beliefs, and effect on social relationships. Grief and depression is more related to the feelings of disappointment, helplessness, loss and sadness. A study11 indicated that women with children are less prone to symptoms of depression whereas depressive symptoms are depicted in women with infertility. Similarly, another study12 showed clinically significant relationship between infertility and depression and two times more depression was found in women with infertility problem compared to the control group.
Further, a study13 found that infertility is associated with dysfunction in sexual relationship, anxiety, depression, difficulties in marital life, and problem in identity.
Anxiety, worry, anguish and desperation are other kinds of emotional reactions to infertility. These responses may be the result of apprehensions related to sexual inadequacy, body image or marital relationships. Effect of infertility is related to some factors such as depression, somatisation and anxiety.14
As far as depression-related infertility is concerned, there is no dearth of researches. Prevalence of depression and anxiety among those who are taking treatment for their infertility is identified by one study.15 Using structured clinical interviews, it reported that criteria for major depressive disorders were met in 17% of the women. Similarly, it found women meeting criteria for mood disorder and dysthymia (26.8% and 9.8%, respectively) as well. Results also indicate anxiety (23%) as the most diagnosed disorder among selected sample. This study was conducted on 112 infertility diagnosed women following treatment, and the measures applied were Mini International Neuropsychiatric Interview (MINI) as well as Hospital Anxiety and Depression Scale (HADS).
The current study was conducted to explore the difference between anxiety and depression among infertile and fertile women.
Subjects and Methods
The study was conducted in 2009 and comprised fertile ad infertile women. The sample of infertile women was drawn from the Liaquat National Hospital, Patel Hospital, Infertility Concept and Zainub Hospital, located in urban areas of Karachi, while fertile women were drawn from the general population in urban Karachi. All the subjects had at least 10 years of education, belonged to all the three socioeconomic classes and were in the age range of 20-35 years. They two groups were further divided into two sub-groups each of working and non-working women.
Infertile women as those suffering for 1 to 5 years from primary infertility and fell under the medical definition of infertility were included. Fertile women were those whose duration of the marriage was from 1 to 5 years.
None of the subjects had medical history of any significance, neither in women nor in their husbands.
The Institute for Personality and Ability Testing (IPAT) Anxiety Scale was introduced in 1957. It is a 40-item scale and the administration time is 15 to 20 minutes. The scale is brief and applicable to the lowest educational levels. The age range of administration of this scale is 15 years and above. The scores derived from the scale are reliable enough for research purposes and group comparison. Each question in the scale has three possible answers, \'Yes\', \'No\' and \'Uncertain\'. The scale gives an accurate estimate of the anxiety level and the test scores have been shown to correlate quite well with the pure anxiety factor, correspond with the actual clinical judgments of anxiety level, and relate to other well-known questionnaire measures of anxiety.16
The IPAT Depression Scale was developed by Krug and Laughlin in 1976. A forced choice technique is used for responding. This is a 40-item scale and it was derived from factor analysis of the primary pathology factors of the Clinical Analysis Questionnaire. The scales comprise multiple choice items offering three possible answers: \'Yes\', \'No\' and \'Uncertain\'. These scales are simple, thus applicable to all educational levels. These scales cover the age ranging from 15 years and above. Reliability for the scale was calculated on more than 2,000 subjects in homogeneous groups. Internal consistency reliability yielded coefficients alpha ranging from 0.85 for adult normals to 0.93 for samples of depressives and clinical patients. The validity and reliability regarding IPAT Anxiety and Depression Scales in Pakistan, was declared positive by a study that was conducted in 1992 and also used the Slosson Oral Reading Test (SORT).17,18
Relevant ethical approvals were obtained for the current study from all concerned, including the institutions and the respondents who were assured of confidentiality.
After data collection on IPAT Depression and Anxiety scales, scoring was done according to the standard procedures given in the respective manuals.16
Data was analysed using SPSS 12. T-test was applied in order to examine the differences in infertile and fertile scores on depression and anxiety.
Results
Of the 120 subjects, the two groups had 60(50%) each. The mean age of fertile women was 27.48±160.75 and that in the infertile group was 27.36±160.75 (Table-1).
Depression among fertile women was 21.85±10.98 compared to 32.01±12.49 among the infertile women. Corresponding values for anxiety was 24.45±9.63 and 36.20±12.51. The difference was significant (Table-2).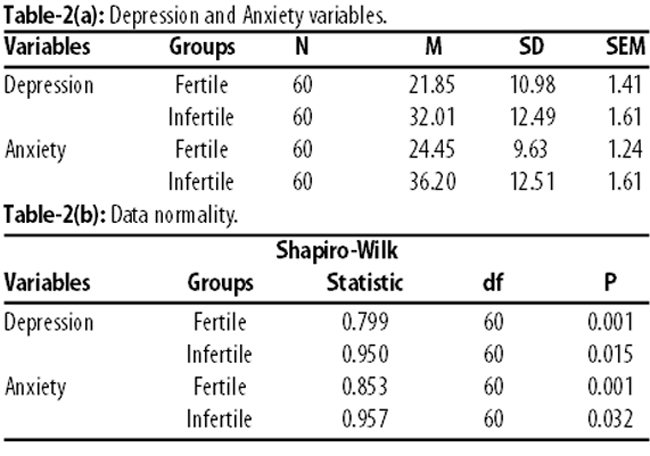
Infertile women had the greater level of depression and anxiety (Table-3)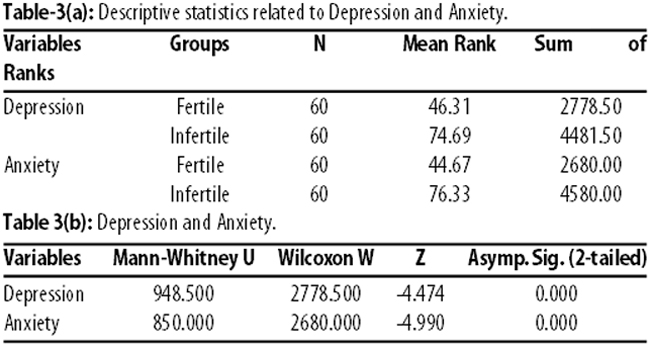
compared to the fertile women. Similarly, the level of anxiety among infertile women was significantly higher than the fertile women (p<0.001).
Discussion
The study, which was conducted to explore the difference between anxiety and depression among infertile and fertile women, revealed that infertile women scored significantly high on the variable of depression and anxiety compared to the fertile women. These findings confirm that women with infertility have higher level of depression and anxiety compared to fertile women.19
Whenever problem of infertility arises, most of the people consider it as only the problem of women. Women are always blamed for not having children. In cultures like Pakistan it seems the woman has also learned to attribute the flaw towards her own self and takes the responsibility. According to a study,20 emotional distress occurs when making infertility problem limited to gender.
Experiences of infertility is a very upsetting thing that happens to an individual. During this up-setting situation, the person needs encouragement, support and care. Lack of such kind of favour from husband or other related individuals or significant others lead to emotional disturbances. This is also justified by researchers who reported that the reaction of society, either favourable or unfavourable, in social networks of infertile women can also determine the psychological issues among them.21
Infertility-related problems are also associated with the support from society. It has the main role to overcome problems and psychological stress. Lack of social support might increase distress. Studies indicate that lack of support from society leads to poor emotional adjustment.22 Support from society sometimes seems to be positive and suitable for individual, but it is not always true. When this support does not fulfil the needs of women, it leads to lack of satisfaction and is also linked with negative emotional reactions.
After identifying the inability of pregnancy by some resources, gradually things required for comfortable life of an individual is destroyed by family or husband. This leads to poor quality of life, and deprivation of things for a quality is associated with psychological frustration and other problems, as shown in literature as well.23 A woman with children has acceptance at home as well as in society. She always feels proud to be a mother. Due to this ability she has a respectable role in her society. She is accepted with her abilities other than reproduction and also given charge and responsibility to control circumstances. When a woman fails to reproduce, it affects her psychological state badly. Gradually a time comes when she feels as if she has no control on her body.
Guilt feelings and self-blame may lead to depression. Infertile woman might feel guilty because she is incapable to give birth owing to some past behaviour, especially involvement in sex in early ages, any premarital relationship or abortion. Few of the previous researches also support this.24
After knowing about the infertility, the woman always tries to solve the problem. She usually gets relevant information. She tries her best to make use of the available services. But problem of infertility is a complicated issue and has painful procedures. Support during these conditions is very necessary, and lack of companion might result into psychological consequences. Anxiety is associated with stages of treatment of infertility among infertile persons.25
Conclusion
Findings suggest that fertile women and infertile women have difference regarding their psychological well-being. There is clinically significant difference between depression and anxiety among women with infertility problem and fertile women. Social and work status appeared as an insignificant predictor of depression and anxiety.
References
1. Arendell T. Conceiving and investigating motherhood: the decade\'s scholarship. J Marriage Fam 2000; 62: 1192-207.
2. Dutta S, Guha R. A Clinico-anatomical study on the common etiological factors pertaining to primary infertility in females using some common investigative procedures. J Anat Soc India 2007; 56 Suppl 2: 14-7.
3. Larsen U. Infertility in Central Africa. Trop Med Int Health 2003; 8: 354-67.
4. Lukse MP, Vacc NA. Grief, depression, and coping in women undergoing infertility treatment. Obstet Gynecol 1999; 93: 245-51.
5. Unruh AM, Mc Grath PJ. The psychology of female infertility: Toward a new perspective. Health Care Women Int 1985; 6: 369-81.
6. Butler P. Assisted reproduction in developing countries-facing up to the issues. Progress in Reproductive Health Research 2003; 63: 1-8.
7. Vayena E, Rowe P, Peterson H. Assisted reproductive technology in developing countries: why should we care? Fertil Steril 2002; 78 Suppl 1: 13-5.
8. Tahir F, Shahab M, Afzal M, Subhan F, Sultan S, Kazi BM, Dil AS. Male reproductive health: an important segment towards improving reproductive health of a couple 2004. In: Chaudhry MA, Desousa M. Population research and policy development in Pakistan. Islamabad: Population Association of Pakistan, 2004; 227-48.
9. Daar A, Merali Z. World Health Organization. Infertility and social suffering: the case of ART in developing countries. (Online) (Cited 2014 May 22). Available from URL: http://www.who.int/reproductive-health/ infertility/5.pdf.
10. World Health Organization (WHO). Technical Report Series. Recent Advances in Medically Assisted Conception 1992; 820: 1-111.
11. Guz H, Ozkan A, Sarisov G, Yanik F. Psychiatric symptoms of Turkish infertile women. J Psychosom Obstet Gynaecol 2003; 24 Suppl 4: 267-71.
12. Domar AD, Clapp D, Slawsby E, Orav J, Freizinger M. The impact of group psychological interventions on distress in infertile women. Health Psychology 2000; 19: 568-75.
13. Anderson KM, Sharpe M, Rattray A, Irvine DS. Distress and concerns in couples referred to a specialist infertility clinic. J Psychosom Res 2003; 54: 353-5.
14. Wischmann T, Stammer H, Scherg H, Gerhard I, Verres R. Psychosocial characteristics of infertile couples: A study by the Heidelberg Fertility Consultation Service. Hum Reprod 2001; 16: 1753-61.
15. Chen TH, Chang SP, Tsai CF, Juang KD. Prevalence of depressive and anxiety disorders in an assisted reproductive clinic. Hum Reprod 2004; 19: 2313-8.
16. Kurg ES, Schier HI, Cattell BR. Hand book for the IPAT anxiety Scale. Institute for personality and ability testing. Illinos: Inc Champaign; 1976.
17. Ahmed ZF, Munaf S. The relationship between anxiety and depression. Pak J Psychol 1991; 22: 15-25.
18. Slosson MA, Richard L. Slosson Oral Reading Test (SORT). Slosson Educational Publications, INC; 1963.
19. Jacob MC, McQuillan J, Greil AL. Psychological distress by type of fertility barrier. Hum Reprod 2007; 22: 885-94.
20. Gonzalas LO. Infertility as a transformational process: a framework for psychotherapeutic support of infertile women. Issues Ment Health Nurs 2000; 21: 619-33.
21. Akizuki Y, Kai I. Infertile Japanese women\'s perception of positive and negative social interactions within their social networks. Hum Reprod 2008; 23: 2737-43.
22. Verhaak CM, Linsten AM, Evers AW, Braat DD. Who is at risk of emotional problems and how do you know? Screening of women going for IVF treatment. Hum Reprod 2010; 25: 1234-40.
23. Aarts JW, van Empel IW, Boivin J, Nelen, WL, Kremer JA, Verhaak CM. Relationship between quality of life and distress in infertility: a validation study of the Dutch Fertility Quality of Life. Hum Reprod 2011; 26 Suppl 5: 1112-8.
24. Lee TY, Sun GH, Chao SC. The effect of an infertility diagnosis on the distress, marital and sexual satisfaction between husbands and wives in Taiwan. Hum Reprod 2001; 16 Suppl 8: 1762-7.
25. Gerrity DA. Five medical treatment stages of infertility: Implications for counselors. The Family J 2001; 9 Suppl 21: 140-50.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: