
Nuzhat Amer ( Department of Obstetrics and Gynaecology, Armed Forces Hospital, Southern Region, Khamis Mushiat, Saudi Arabia. )
Muhammad Amer ( Department of Ophthalmology, Armed Forces Hospital, Southern Region, Khamis Mushiat, Saudi Arabia. )
Mohamed Kolkailah ( Department of Obstetrics and Gynaecology, Armed Forces Hospital, Southern Region, Khamis Mushiat, Saudi Arabia. )
Magdy Al-Dumairy ( Department of Obstetrics and Gynaecology, Armed Forces Hospital, Southern Region, Khamis Mushiat, Saudi Arabia. )
November 2014, Volume 64, Issue 11
Original Article
Abstract
Objective: To assess the frequency and outcome in pregnant females suspected to have foetal central nervous system anomalies on the basis of ultrasonography.
Methods: The retrospective study was conducted at the Department of Obstetrics and Gynaecology, Armed Forces Hospital, Southern Region, Khamis Mushait, Saudi Arabia, and comprised all women who were diagnosed by ultrasound to have foetal central nervous system abnormalities during anomaly scan at 18-20 weeks between January 2009 and December 2012. Data was retrieved from patient files and reviewed for foetal and maternal outcome.
Results: Of the 31754 live births at the hospital during the study period, 22880(72%) pregnant women were sent for ultrasonography to have foetal central nervous system anomalies checked. Of them, 181(0.57%) women had positive scans. Mean maternal age was 29.8±7 years and the mean gestational age at diagnosis was 24.4±7 weeks. There were 35(19%) primigravida, 108(60%) Para 2 to 5, and 38(21%) more than Para 5. Overall, 102(56.4%) women delivered vaginally, while 50(27.6%) delivered by caesarean section. Mean gestational age at delivery was 37.5±4.2 weeks. Major anomalies included ventriculomegaly 95(52.2%) neural tube defect 31(17.03%), cisterna magna 17(9.34%), and acrania 12(6.6%). No termination of pregnancy was done due to legal and religious reasons.
Conclusion: Antenatal detection of central nervous system anomalies by screening with ultrasonography helps make multidisciplinary management plans.
Keywords: Neural tube defects, Ventricular megaly, Spina Bifida, Ultrasonography, Antenatal screening. (JPMA 64: 1282; 2014).
Introduction
Cerebral anomalies at birth account for 9% of all isolated anomalies and are present in 15.9% of babies with multiple malformations. This raises the importance of antenatal diagnosis. Majority of anomalies can be diagnosed by ultrasonography (USG) and it is the basic screening for pregnant women because of its efficacy, easy availability, low cost and real-time capability. The presence of an interface between cerebrospinal fluid (CSF) and nervous system tissue makes the central nervous system (CNS) particularly suitable for evaluation with ultrasound imaging.1 Foetal CNS anomalies represent an important factor of morbidity and mortality in children.2
Among foetal CNS anomalies are ventriculomegaly (VM) (Figure-1),
agenesis of corpus callosum (ACC), holoprosencephaly, microcephaly, Dandy Walker malformation (DWM), anencephaly (Figure-2)
encephalocele and Spina Bifida (SB) (Figure-3).3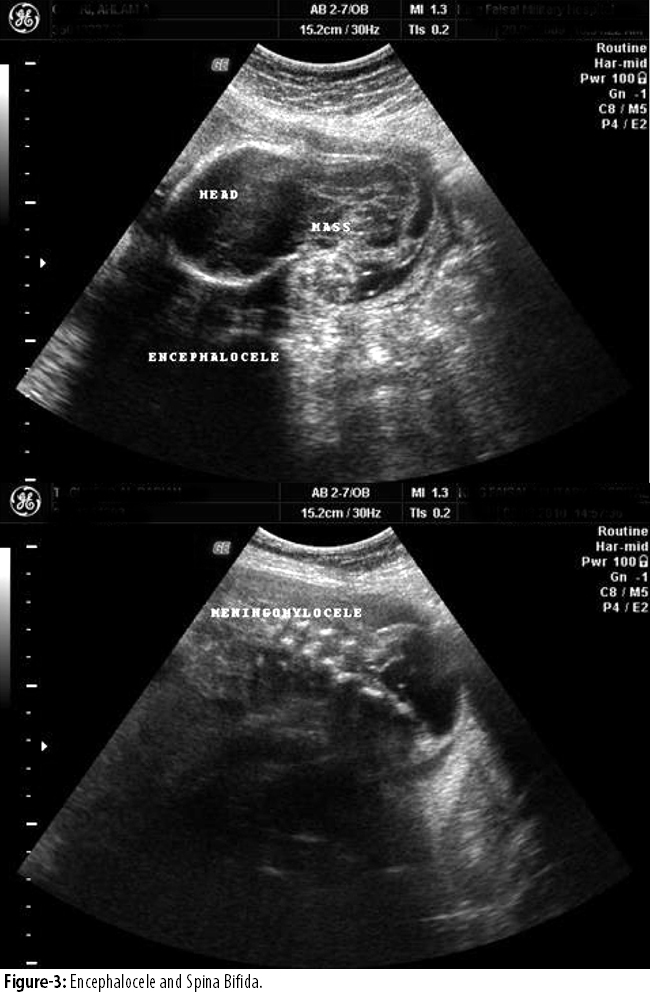
Neural tube defects (NTDs), including anencephaly, SB and encephalocele, are among the most severe and frequent birth defects though they are amenable to preventions with folic acid fortification or supplementation.4 Of all congenital anomalies, NTDs are the easiest to identify prenatally. Gestational age greatly influences the type of NTD that can be detected. First trimester scanning typically quotes detection rate of >90% for anencephaly and 80% for encephalocele, but lower rate (44%) for SB.5 According to foetal anomaly screening programme, 98% detection rate was for anencphaly and 90% for open SB.6 The incidence of SB has fallen over the past six decades in many countries. This decline strongly suggests the importance of environmental and other determinants. However, other factors remain such as consanguinity and racial variables of the parents which are difficult to change.7
VM, indicating the presence of excess of fluid, usually CSF, in the lateral ventricle of the developing brain, can be categorised as mild (10-12mm), moderate (>12-15mm) and severe (>15mm).8 Congenital CNS malformations are relatively common and account for a substantial proportion of miscarriages, still-births, neonatal and infant deaths. The availability of prenatal screening gives the parents choice of preparing for the birth of the baby with congenital disorder or to consider termination of pregnancy.9
Material and Methods
The retrospective study was conducted at the Department of Obstetrics and Gynaecology, Armed Forces Hospital, Southern Region, Khamis Mushait, Saudi Arabia, and comprised all women who were diagnosed by ultrasound to have foetal CNS abnormalities during anomaly scan at 18-20 weeks between January 2009 and December 2012. Data was retrieved from patient records which are kept both manually and electronically. The study site is a regional tertiary care centre where around 8000 deliveries take place every year.
Women who were suspected to have foetuses with CNS abnormalities on USG were followed throughout the antenatal period by USG. Antenatal and postnatal outcome were observed. Anomaly scans were performed by an experienced obstetrics sonologist. All suspected CNS anomalies were discussed with neonatologists and parental counselling was done antenatally for prognosis, and postnatal follow-up was planned.
For the purpose of the study, VM was defined as dilatation of the cerebral ventricles greater than a diameter of 10mm. Holoprosencephaly was defined as a single midline ventricular cavity with failure in the development of midline sagittal structures. Microcephaly was defined as foetal head size being 2 standard deviations (SD) or more below the mean. DWM was defined as agenesis or hypoplasia of the cerebellar vermis, cystic dilatation of the fourth ventricle, and enlargement of the posterior fossa. Arnold Chiari malformation was defined as downward displacement of the medulla, fourth ventricle and cerebellum into the cervical spinal canal, as well as elongation of the pons and fourth ventricle probably due to a relatively small posterior fossa. Encephalocele was defined as herniation of brain tissue and meninges from cranial bone defect. SB was defined as opening in the vertebral column and herniation of spinal cord or meninges from this defect. Choroid plexus (CP) cyst was defined as cyst >1mm in diameter.
All maternal, foetal and neonatal records relevant to the study were reviewed and their outcomes were recorded and analysed using GNU PSPP and Microsoft Excel software.
Results
Of the 31754 live births at the hospital during the study period, 22880(72%) pregnant women were sent for ultrasonography to have foetal CNS anomalies checked. Of them, 181(0.57%) women had positive scans (5.7 per 1000 live births). Mean maternal age was 29.8±7 years and the mean gestational age at diagnosis was 24.4±7 weeks. Mean gestational age at delivery was 37.5±4.2 weeks. There were 35(19%) primigravida, 108(60%) Para 2 to 5, and 38(21%) more than Para 5.
Previous anomaly was present in 23(12%) women; 36(19.8%) took folic acid antenatally in first three months of pregnancy; 47(25.8%) had cousin marriage; and 23(12%) women were known diabetics.
Major anomalies included VM 95(52.2%), NTDs 31(17.03%), cisterna magna 17(9.34%), and acrania 12(6.6%) (Table-1).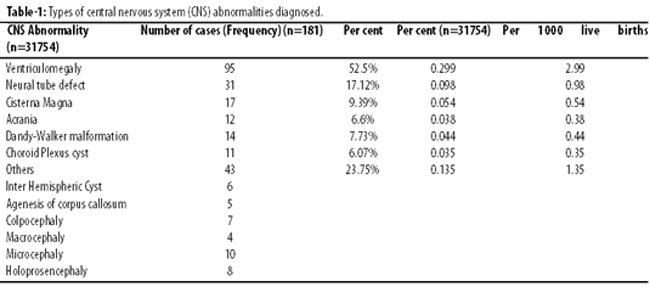
Out of the 95 cases of VM, 52(54.74%) were mild and 29(55%) of them were found to be normal on late scan. Besides, 22(23.16%) were moderate VM, 11(11.58%) were severe VM, and 27(24.42%) had other abnormality along with VM. Ventriculoperitoneal (VP) shunt was performed in 6(6.3%), SB repair was done in 3(3.15%) and in 2(2.1%) Aqueduct stenosis repair was done.
Overall, 102(56.4%) women delivered vaginally, while 50(27.6%) delivered by caesarean section (CS). The outcome in 11(6.08%) women was miscarriage (Table-2),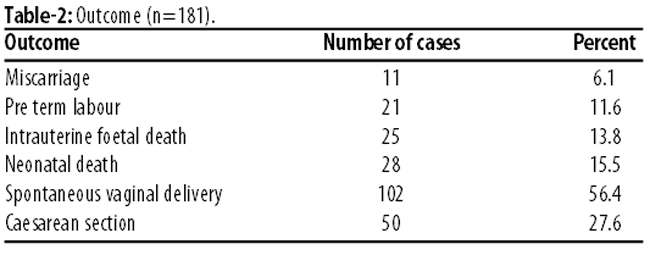
while 18 (9.9%) women did not show up for delivery.
No termination of pregnancy was done due to legal and religious reasons.
Discussion
Ultrasonography is an appropriate method to do foetal imaging for diagnosing CNS anomalies. USG has been proven to be reliable, reproducible and safe for mother and foetus.3 In our study the anomaly spectrum was very large. This affects the gestational age at diagnosis and neonatal outcome. In Saudi Arabia, termination of pregnancy due to foetal anomaly is usually not done due to religious reasons.7,10 This type of practice may influence feto-maternal outcome due to increased maternal morbidity as well as foetal and neonatal mortality. This has a negative effect on the medical and social services due to increased economic burden and workload. Carrying an abnormal baby throughout the pregnancy may affect the psychology of the couple.10
Frequency of CNS anomalies in our study is comparable to another study.3 Frequency of 0.01% (1/1000 live births) in our study for NTD is comparable to other studies from Saudi Arabia.7,11-13
Further, 19% of women with diagnosed foetal CNS anomalies used folic acid in early pregnancy period. In Saudi Arabia, grain fortification with folate and folic acid supplementation is implemented as there is low awareness among population about taking folic acid in peri-conceptional period. Folic acid is not prescribed in time as most of the pregnancies are un-planned and there is low treatment compliance even if folic acid is prescribed.14
Consanguinity of the parents is one the significant risk factors for CNS anomalies. In our study, 25.8% of the parents were cousins.7
It is extremely important that parents are counselled antenatally about the prognosis of the foetus to reduce anxiety in post-natal period. For this, neonatologist can be encouraged to discuss the prognosis with the parents and devise a follow-up plan. Normal neurological development has been reported for prenatally diagnosed and postnatally followed hydrocephaly with callosal agenesis.15 Most common associated anomaly in VM is corpus callosum agenesis and in isolated VM, normal neurological development can be expected but with delayed cognitive and/or motor development.16 In isolated cisterna magna, there can be lower scores to controls on some parameters of memory and verbal fluency, but overall normal cognitive function is expected. This information may be important for counselling of the parents.17 Foetal magnetic resonance imaging (MRI) for VM is helpful for diagnosis, prognosis and decision about postnatal neurosurgical intervention.18-20 In isolated mild VM, postnatal neuro-developmental prognosis is >90%. Prognosis is less favourable for severe VM.8 For our patients, in six neonates out of 9 with severe VM, VP shunt was done.
In very early pregnancy, empty or enlarged cavities or abnormal contours of head and spine are important diagnostic parameters for the detection of CNS anomalies on USG.21 As such, 3D and 4D USG and MRI may help to confirm suspected CNS anomalies detected on routine anomaly scans.22
Conclusion
Prenatal detection of CNS abnormalities with multi-disciplinary approach involving neonatologists, neurosurgeons, paediatric surgeons, expert sonologists and obstetricians will influence the peri-natal outcome as well as increase parents understanding and acceptance for the outcome. Foetal karyotyping should be offered in cases with CNS anomalies to diagnose the genetic cause for further genetic counselling and management. Religious scholars should be approached to explore the possibilities of termination of pregnancy in cases where foetal outcome is expected to increase the burden on medical and social services.
Reference
1. Ben Sira L, Garel C, Leitner Y, Gross-Tsur V. Prenatal imaging of the fetal brain--indications and developmental implications of fetal MRI. Harefuah 2008; 147: 65, 70-93.
2. Adeleye AO, Olowookere KG. Central nervous system congenital anomalies: a prospective neurosurgical observational study from Nigeria. Congenit Anom (Kyoto) 2009; 49: 258-61.
3. Ozkan ZS, Gilgin H, Aygun HB, Deveci D, Simsek M, Kumru S, et al. Our clinical experience about prenatal diagnosis and neonatal outcomes of fetal central nervous system anomalies. J Matern Fetal Neonatal Med 2011; 24: 502-5.
4. Salvador J, Arigita M, Carreras E, Lladonosa A, Borrell A. Evolution of prenatal detection of neural tube defects in the pregnant population of the city of Barcelona from 1992 to 2006. Prenat Diagn 2011; 31: 1184-8.
5. Whitlow BJ, Chatzipapas IK, Lazanakis ML, Kadir RA, Economides DL. The value of sonography in early pregnancy for the detection of fetal abnormalities in an unselected population. Br J Obstet Gynaecol 1999; 106: 929-36.
6. Ward P, Soothill P. Fetal anomaly ultrasound scanning: the development of a national programme for England. Obstet Gynaecol 2011; 13: 211-7.
7. Murshid WR. Spina bifida in Saudi Arabia: is consanguinity among the parents a risk factor? Pediatr Neurosurg 2000; 32: 10-2.
8. Gaglioti P, Oberto M, Todros T. The significance of fetal ventriculomegaly: etiology, short- and long-term outcomes. Prenat Diagn 2009; 29: 381-8.
9. Atkinson DE, Amin F, Russell S, D\'Souza SW. Fetal congenital anomalies diagnosed by ultrasound in Asian and non-Asian women. J Obstet Gynaecol 2008; 28: 678-82.
10. Al-Alaiyan S, Alfaleh KM. Aborting a Malformed Fetus: A Debatable Issue in Saudi Arabia. J Clin Neonatol 2012; 1: 6-11.
11. Magbool G, Al Mulhim I, Uduman S, Al Umran K. Congenital anamolies in liveborn Saudi infants. Emirates Med J 1989; 7: 7-10.
12. Al Awary B, El Lardi A, El Najashi S, El Umran K, Ammar A. Prevalence, at birth of hydrocephalus, myelomeningeocele, Dandy-Walker syndrome, anencephaly and encephalocele in Saudi Arabia. Pan Arab J Neurosurg 1997; 1: 31-5.
13. Asindi A, Al-Shehri A. Neural tube defects in the Asir Region of Saudi Arabia. Ann Saudi Med 2001; 21: 26-9.
14. Safdar OY, Al-Dabbagh AA, Abuelieneen WA, Kari JA. Decline in the incidence of neural tube defects after the national fortification of flour (1997-2005). Saudi Med J 2007; 28: 1227-9.
15. Imataka G, Nakagawa E, Kuwashima S, Watanabe H, Yamanouchi H, Arisaka O. Callosal agenesis followed postnatally after prenatal diagnosis. Congenit Anom (Kyoto) 2006; 46: 160-62.
16. Lee CS, Hong SH, Wang KC, Kim SK, Park JS, Jun JK, et al. Fetal ventriculomegaly: prognosis in cases in which prenatal neurosurgical consultation was sought. J Neurosurg 2006; 105: 265-70.
17. Zimmer EZ, Lowenstein L, Bronshtein M, Goldsher D, Aharon-Peretz J. Clinical significance of isolated mega cisterna magna. Arch Gynecol Obstet 2007; 276: 487-90.
18. Chung R, Kasprian G, Brugger PC, Prayer D. The current state and future of fetal imaging. Clin Perinatol 2009; 36: 685-99.
19. Hankinson TC, Vanaman M, Kan P, Laifer-Narin S, Delapaz R, Feldstein N, et al. Correlation between ventriculomegaly on prenatal magnetic resonance imaging and the need for postnatal ventricular shunt placement. J Neurosurg Pediatr 2009; 3: 365-70.
20. Manganaro L, Savelli S, Francioso A, Di Maurizio M, Coratella F, Vilella G, et al. Role of fetal MRI in the diagnosis of cerebral ventriculomegaly assessed by ultrasonography. Radiol Med 2009; 114: 1013-23.
21. Blaas HG, Eik-Nes SH. Sonoembryology and early prenatal diagnosis of neural anomalies. Prenat Diagn 2009; 29: 312-25.
22. Correa FF, Lara C, Bellver J, Remohi J, Pellicer A, Serra V. Examination of the fetal brain by transabdominal three-dimensional ultrasound: potential for routine neurosonographic studies. Ultrasound Obstet Gynecol 2006; 27: 503-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: