
Iram Khursheed ( Department of Educational Development, Family Medicine, Psychiatry, Faculty of Health Sciences, Aga Khan University, Karachi, Pakistan. )
Lubna Baig ( Medical Education, King Saud Bin Abdulaziz University of Health Sciences, Riyadh, Saudi Arabia. )
November 2014, Volume 64, Issue 11
Original Article
Abstract
Objectives: To measure the students\' perceptions of educational environment of a medical school, to compare the perceptions of high, average and low academic achievers, and to explore the relation between these perceptions and their academic achievements in order to identify specific problem areas.
Methods: The cross-sectional study was conducted at Ziauddin University, Karachi, during the mid of the 2010-11 academic year using Dundee Ready Education Environment Measure inventory. Data was collected from 200 undergraduate medical students of all five years. Analysis was performed using both Inventory guidelines on SPSS19.0.
Results: Of the 200 students initially enrolled, completed forms were received from 168(84%). The overall mean score was 117+/-8.3. Mean comparison of their perceptions on the overall score was significantly less (p<0.001) for the low achievers across all 5 years. Moderate positive correlation (r= 0.417) was found between perceptions and academic achievements.
Conclusions: Students\' perceptions of their educational environment were reasonably positive, indicating adequate satisfaction in most areas. Emphasis needs to be paid on the implementation of strong student support system across all medical schools to initiate timely remedial measures where needed. The learning environment should be evaluated regularly for quality improvement purposes.
Keywords: DREEM-inventory, Perception, Educational environment, Medical students. (JPMA 64: 1244; 2014).
Introduction
Educational environment plays a vital role in producing competent healthcare professionals since it influences how, why and what students learn. It is thus regarded as one of the most important factors determining achievements of medical students.1
It has been defined as everything that is happening in the medical school and is said to be influenced by the curriculum which is also a determinant of the behaviour of the medical school\'s students and teachers.2 Educational environment encountered by students has an impact on their perceived well-being, aspirations and academic achievements.3
Students are one of the main stakeholders of medical school curriculum. Their perception provides basis for modification of elements operating in educational environment or climate in order to enhance the learning experiences in relation to the teaching goals. It is therefore pivotal to assess the climate of the institution on a regular basis in order to nurture the areas of excellence and improve the areas needing attention.3
The World Federation for Medical Education (WFME) singles out \'learning environment\' as one of the \'targets\' for what it terms \'the conduction of the evaluation of medical education programmes\'.5 Its importance has been further highlighted by the Standing Committee on Postgraduate Medical Education (SCOPME), stating that a working environment that is conducive to learning is critically important to successful training. The university learning environment is a complex construct that includes a wide range of aspects and diverse foci.6
Dundee Ready Education Environment Measure (DREEM) Inventory has been used all over the world for evaluating the educational environment.7,8 DREEM is a 50-item inventory developed at Dundee for assessing learning environment specifically for medical schools and other health professions. It has been used for many purposes, like identifying the strengths and weaknesses of a teaching programme, comparing the outcomes of a programme delivered at different centres etc.9-11
In Pakistan, no major work is so far done in this regard except for one study published in 2011.12 Evaluation of educational environment of medical institutions should be done on a regular basis. It is, therefore, a need felt at institutional level to get regular analysis of students\' perceptions of the educational environment.
The current study was planned with multiple aims to measure the students\' perceptions of educational environment of a medical school, to compare the perceptions of high, average and low academic achievers, to explore the relation between these perceptions and their academic achievements, and to identify specific problem areas that may need to be set right.
The study was conducted at a university Where problem-based learning is used as one of the main teaching strategies at the undergraduate level as part of the medical curriculum. The five-year training programme consists of two pre-clinical and three clinical years.13
Subjects and Methods
The cross-sectional study was conducted at Ziauddin University (ZU), Karachi, during the mid of the 2010-11 academic year. A questionnaire was distributed at each level of undergraduate medical education. The sample size was estimated by using the following formula:
n = (Z2 × P(1 - P))/e2
Estimated Proportion 0.3, confidence interval (CI) 0.95, desired precision of estimate 0.05 and the total population of students was 400. The sample came out to be 179; we added 20 more for form distribution to account for incomplete forms. We selected 40 out of 100 students from all the five years (first year to final year, batch XI- batch XV), using convenience sampling method. Ethical approval was taken from ZU Ethics Review Committee.
The inventory was administered to the students just after a lecture class. Informed consent was taken after explaining briefly the purpose and process of collecting data. It was ensured that there would be strict confidential coding of their names and roll numbers. Ethical considerations were maintained throughout the process.
The 50-item DREEM-inventory has a maximum score of 200, indicating an ideal educational environment. Allocation of scores on a 5-point Likert scale is defined as; 4=strongly agree, 3=agree, 2=unsure, 1=disagree and 0=strongly disagree, resulting in a maximum score of 200. There are nine negatively expressed items (4, 8, 9 17, 25, 35, 39, 48 and 50) and are scored in the reverse order.
The guidelines for the interpretation of scores on (i) individual items, (ii) subscales and (iii) overall DREEM (Appendix-1A, 1B and 1C) were all followed.
The instrument was piloted with 5 faculty members and 2 students in the final year of study.
Only the completed data-sets with <10% missing data were used, while others were excluded from the study. Missing data was labelled as "uncertain" and scored 2.Data was analysed on SPSS 19.0 using DREEM guidelines.
Academic results (scores) of students were taken from the examination cell under strict confidentiality and entered in the form of students\' percentages with confidential coding of their identity. Based on their percentages, another variable with three sub-groups was created on SPSS. Grouping was done on the basis of cut off-percentages as: low achievers <59.9%; average achievers 60-64.9%; and high achievers >65%.
Normality of data was checked and found to be non-normal data.
Non-parametric one-way analysis of variance (ANOVA) was used to compare means of perceptions of learning environment among high, average and low achievers. Tukey\'s post-hoc test was also used for within-group comparisons.
Spearman´s correlation coefficient was used to perform correlation analysis of the students perceptions of learning environment (mean DREEM overall scores) to that of their academic achievements (academic score in percentages), results were considered statistically significant at p<0.05.
Results
Of the 2000 questionnaires distributed, 168(84%) were included in the final analysis, while 32(16%) forms were excluded owing to >10% missing values.
Overall, high achievers were 78(46.4%), average achievers were 49(29.1%) and low achievers were 41(24.4%).
Cronbach\'s alpha coefficient for the overall DREEM inventory scores was 0.84.The overall mean DREEM score was 117±8.3. High and low scores on individual items and on five subscales were worked out separately (Table-1).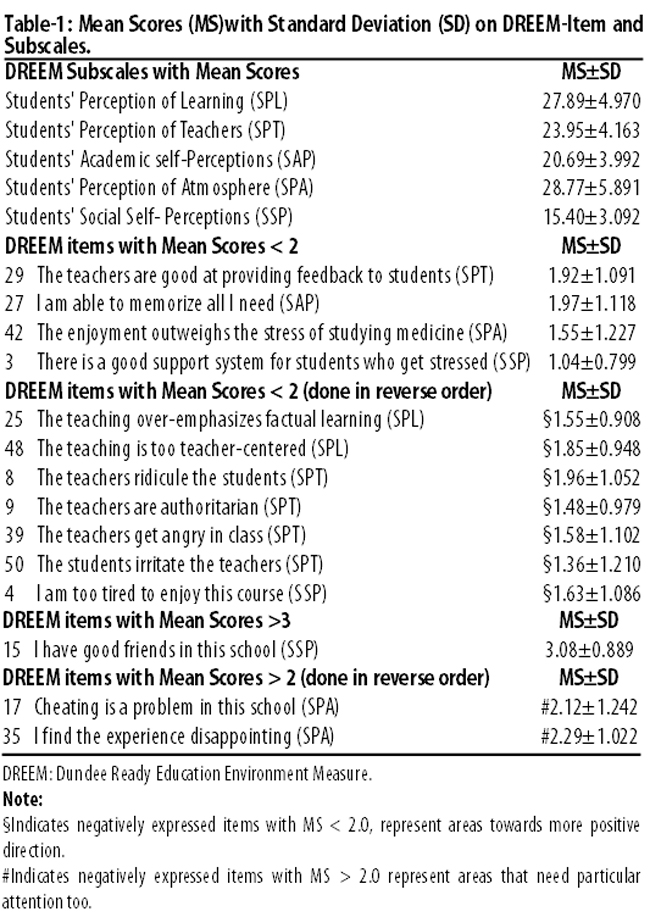
Variations were observed in responses to individual items while identifying specific strengths and weaknesses within the learning environment. Scoring on 11 items (3, 4, 8, 9, 14, 25, 27, 29, 42, 48 and 50) was found less than 2, out of which six items (4,8,9,25,48 and 50) were negatively expressed items and their low scores suggest movement in a positive direction whereas low scoring on the rest of the five items indicates need of particular attention. Moreover, scoring on item15 proved to be one of the strongest areas.
The mean subscale score on Students\' Perceptions of Learning (SPL) 27.89±4.970 showed a more positive approach towards learning.
Except for two negatively expressed items, all other items on SPL showed mean item scores >2.0, indicating that they could be further improved.
The mean subscale score on Students\' Perceptions of Teachers (SPT) was 23.95±4.163 which indicates that it is moving in the right direction. According to mean DREEM-item-score on SPT, all students reported that the teachers were knowledgeable 2.87±0.68 and the clinical teachers were thought to be tolerant with the patients 2.67±0.95. In general, students\' perceptions regarding their teachers showed that their teachers had good communication skills, they gave clear examples, and that the teachers were well prepared for their classes. Scores obtained on DREEM items on SPT indicated that these areas could be further improved. On the other hand, low scores on negatively expressed items, such as \'teachers ridicule the students and are authoritative\', signify that the attitude of teachers is positive. As per students\' perception, the quality of feedback was ineffective 1.92±1.09 and the area needed particular attention. The mean score on Students\' Academic Self-Perceptions (SAP) was 20.69±3.992 indicating that they were feeling more on the positive side. They all believed that they were well-prepared for the profession and were also confident about passing the examinations. All of them felt to a great extent that what they had learnt was relevant for a career in medicine.
The Students\' Perceptions of Atmosphere (SPA) aspect was overall rated quite positive by the students 28.77/48±5.891. They all agree that there were opportunities to develop their interpersonal skills and that the experience gained by them was not disappointing. Cheating was considered a problem area that needed particular attention. Moreover, they felt that the course was not enjoyable enough to reduce the stress of studying medicine. Overall, students found the atmosphere relaxing for them in ward teachings 2.52±1.049, during the lectures 2.58±0.892 and more profoundly during seminars 2.86±0.821.
The mean score on Students\' Social Self-Perceptions (SSP) was 15.40±3.092. It was perceived in general that the support system for students who became stressed was not good 1.04±0.799. Additionally, the students felt bored quite often 1.68±1.095. On the other hand they reported that their social life was going well 2.85±1.009. They agreed that they had good friends in their institution 3.08±0.889 and that the accommodation was pleasant 2.82±0.887.
One-way ANOVA indicated significant differences (F=22.607; p<0.001). In the means of students\' perception of learning environment on DREEM overall scores among the three groups of achievers. The high achievers reported more positive perception of learning environment than the average and low achievers who reported the greatest mean (Table-2).
Tukey\'s post-hoc test revealed that the students\' perception of learning environment was significantly higher (p<0.01) among good achievers (both high and average achievers) compared to the low achievers. There was no statistically significant difference (p<0.101) between high and average achievers.
Spearman correlation showed a significant (p<0.05) and moderately positive correlation (r=0.417) between students\' perceptions of learning environment (mean DREEM overall scores) and their academic achievements (academic score in percentages).
Discussion
Overall mean DREEM score of 117 out of a maximum 200 obtained by the study indicates that the learning environment on the campus was more positive than negative. Moreover, the result is comparable with those obtained from other medical schools with integrated curricula from Kuwait (106/200), the United Arab Emirates (120/200), and England (125/200),14-16 as well as from Punjab, Pakistan (125/200).12
The information obtained from the data demonstrates how the students\' perceptions of their learning environment in the context of this study are related to their academic performance. Study results suggest that the students\' perceptions of learning environment correlate moderately with their academic achievements. Positive self perceptions of competence are related to positive outcomes, including good academic performance.
The curriculum at the study site was integrated and student-centred. It is evident from the mean score of 2.25±0.989 on item number 13. Students from year one to year four are provided with the opportunity to interact with the community by assigning community healthcare tasks. Each task is discussed in large class format initially to make them understand what they actually need to do, which is then followed by the field visit (experiential learning opportunity). Students learn best by doing. Learners should complete the full experimental learning cycle in order to gain a complete understanding of a concept; the steps in the cycle are concrete experience, observation and reflection, forming abstract concepts and testing the concepts in new situations.17
They are also given research tasks to work in small groups. Use of Problem Based Learning (PBL) during the two pre-clinical years makes them able to take part actively in group discussions to solve problems close to real life clinical cases. It is evident from the mean score of 2.8±0.830 on item number 41. Learners should be given opportunities to develop their own understanding through self-directed learning, combined with dialogue with their teachers and peers.17 It is evident that PBL improves the attitudinal outcomes as well as long-term retention of knowledge compared to traditional instruction.18
During their three clinical years, the students learn to take medical history, do clinical examination of real patients and to interact with the patients\' families under direct supervision of clinical coordinators.
Students receive feedback on the level of their active knowledge contribution as part of the PBL process during pre-clinical years and on the level of competence they achieve in clinical encounter during clinical years. This is the area which needed particular attention as evident from the level of dissatisfaction expressed by students regarding feedback they receive from their teachers. This emphasises the need of faculty development to bring improvement in the quality of providing effective feedback.
Scores obtained on item number 10 and 21 reflect their positive self-concept. Self-concept has been defined broadly as "a person\'s self-perceptions formed through experience with and interpretations of his or her environment."19,20 Recent reviews have shown at various levels of analysis, and in various domains, that positive self-concept is moderately correlated to positive outcomes.21
However, when the students\' expectations are not met in reality, they experience disappointment and discomfort which may directly influence the quality of their learning experiences/academic achievements.19
A study conducted in India found significant differences between high and low academic achievers, showing positive perceptions of high achievers regarding teachers, academic atmosphere and social self-perceptions compared to the under-achievers.11
Another study conducted in Malaysia on engineering students, found academic self-confidence one of the mediating variables between positive verbal input and improved cognitive performance.22 A conducive learning environment, for example, comfortable learning rooms, receptive clinical environment and motivated, skilled and approachable teachers, is believed to increase learner motivation, which in turn leads to better engagement in learning, and improved performance.23 Development of higher order skills or meta-competencies is a complex and interrelated process, which is affected by all aspects of the learning environment.24
It is also evident that even within an optimised learning environment there are significant variations in the students\' learning gain. Factors like personal learning styles and motivation could ultimately govern a student\'s achievement.25,26 Positive attitudes and deep approach are closely linked with academic progress.
As educational environment affects students\' achievement, satisfaction and success, it is important to get regular feedback from students regarding their learning experiences.
Use of the DREEM as a monitoring tool may permit timely interventions to take remedial steps regarding problematic educational environments. As evident from literature, when the students\' learning problems remain unaddressed, their learning environment remains unaltered, leading to repetition of failure.27
The main limitation of this study is the convenience sampling method. This may produce somewhat inflated results, as those who were present at the time of the study may have felt more positively (evidenced by the fact that they were in the class) than those who were absent and more likely to produce deflated results. This is because those with less satisfaction may have been keener to take part in order to voice their grievances.
It can be delimited by taking larger sample sizes by selecting all students from all the years of undergraduate medical education.
Conclusion
Students\' perceptions of their educational environment were reasonably positive amongst all batches, indicating adequate level of satisfaction in most areas of the existing curriculum. The establishment of formal student support programmes appropriately within the university is strongly recommended to address issues that may hamper the learning of low academic achievers. Continuous evaluation of learning environment should be emphasised. Further studies are recommended to explore the students\' perceptions of learning environment.
Acknowledgement
The authors are grateful to the Dean of undergraduate medical education, Ziauddin Medical College, Dr Kamran Hameed, as well as the Chief Controller of Examinations, Dr Qamaruddin Barakzai, for their support in data collection.
References
1. Bassaw B, Roff S, McAleer S, Roopnarinesingh S, De Lisle J, Teelucksingh S, et al. Students\' perspectives on the educational environment, Faculty of Medical Sciences, Trinidad. Med Teach 2003; 25: 522-6.
2. Genn J. AMEE Medical Education Guide No 23 (Part 1): Curriculum, environment, climate, quality and change in medical education - a unifying perspective. Med Teach 2001; 23: 337-44.
3. Plucker JA. The relationship between school climate conditions and student aspirations. J Educ Res 1998; 91: 240-6.
4. Till H. Climate studies: can students\' perceptions of the ideal educational environment be of use for institutional planning and resource utilization. Med Teach 2005; 27: 332-7.
5. World Federation for Medical Education. International standards in medical education: assessment & accreditation of medical schools\' educational programmes. A WFME position paper. Med Educ 1998; 32: 549-58.
6. Huang SL FD. Associations of the University Learning Environment with Academic Engagement & Satisfaction among Science Majors in Taiwan. The Asia-Pacific Education Researcher 2011; 20: 291-307.
7. Miles S, Swift L, Leinster SJ. The Dundee Ready Education Environment Measure (DREEM): a review of its adoption and use. Med Teach 2012; 34: e620-34.
8. Zawawi AH, Elzubeir M. Using DREEM to compare graduating students\' perceptions of learning environments at medical schools adopting contrasting educational strategies. Med Teach 2012; 34 (Suppl 1): S25-31.
9. Till H. Identifying the perceived weaknesses of a new curriculum by means of the Dundee Ready Education Environment Measure (DREEM) Inventory. Med Teach 2004; 26: 39-45.
10. Avalos G, Freeman C, Dunne F. Determining the quality of the medical educational environment at an Irish medical school using the DREEM-inventory. Ir Med J 2007; 100: 522-5.
11. Mayya SS, Roff S. Students\' Perceptions of Educational Environment: A Comparison of Academic Achievers and Under Achievers at Kasturba Medical College India. Educ Health (Abingdon) 2004; 17: 280-91.
12. Khan JS, Tabasum S, Yousafzai UK, Fatima M. DREEM ON: Validation of the Dundee Ready Education Environment Measure in Pakistan. J Pak Med Assoc 2011; 61: 885-8.
13. Jaleel A, Rahman MA, Huda N. Problem-based learning in biochemistry at Ziauddin Medical University, Karachi, Pakistan. Biochem Mol Biol Educ 2001; 29: 80-4.
14. Bouhaimed M, Thalib L, Doi SAR. Perception of the Educational Environment by Medical Students Undergoing a Curricular Transition in Kuwait. Med Princ Pract 2009; 18: 204-8.
15. Shehnaz SI, Sreedharan J. Students\' perceptions of educational environment in a medical school experiencing curricular transition in United Arab Emirates. Med Teach 2011; 33: e37-e42.
16. Fidelma D, McAleer S, Roff S. Assessment of the undergraduate medical education environment in a large UK medical school. Health Educ J 2006; 65: 149-58.
17. Kaufman DM. Applying Educational Theory in Practice. In: Cantillon P WD, editor. ABC of Learning and Teaching in Medicine. 2nd ed. Chichester, West Sussex: Wiley-Blackwell; 2010.
18. Norman GR, Schmidt HG. The Psychological Basis of Problem-Based Learning: A Review of Evidence. Acad Med 1993; 67: 557-65.
19. Valentine JC, DuBois DL, Cooper H. The Relation between Self-Beliefs and Academic Achievement: A Meta-Analytic Review. Educ Psychol 2004; 39: 111-33.
20. Marsh HW, Hattie J. Theoretical perspectives on the structure of self-concept. In: Bracken BA (Ed.), Handbook of self-concept: Developmental, social, and clinical considerations Bracken BA, editor. New York: Wiley; 1996.
21. Baumeister RF, Campbell JD, Krueger JI, Vohs KD. Does high self?esteem cause better performance, interpersonal success, happiness, or healthier lifestyles. Psych Sci in the Public Interest 2003; 4: 1?44.
22. Alias M, Hafir NAHM. The relationship between academic self-confidence and cognitive performance among engineering students. Proceedings of the Research in Engineering Education Symposium. In Palm Cove, QLD; 2009.
23. Hutchinson L. Educational environment. BMJ 2003; 326: 810-2.
24. Lizzio A, Wilson K, Simons R. University Students\' Perceptions of the Learning Environment and Academic Outcomes: implications for theory and practice. Stud Higher Educ 2002; 27: 27-52.
25. Yates J, James D. Predicting the "strugglers": a case-control study of students at Nottingham University Medical School. BMJ 2006; 332: 1009-13.
26. Ferguson E, James D, O\'Hehir F, Sanders A, McManus IC. Pilot study of the roles of personality, references, and personal statements in relation to performance over the five years of a medical degree. BMJ. 2003; 326: 429-32.
27. Tooth D, Tonge K, McManus IC. Anxiety and study methods in preclinical students: causal relation to academic performance.. Med Educ 1989; 23: 416-21.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: