
Mahjabeen Sharif ( Pharmacology Department, Army Medical College, Rawalpindi. )
Bushra Tayyaba Khan ( Pharmacology Department, Army Medical College, Rawalpindi. )
Khalida Ajmal ( Wah Medical College, Wah Cantt. )
Mohammad Asim Anwar ( Pakistan Atomic Energy Commission Hospital, Islamabad. )
August 2014, Volume 64, Issue 8
Original Article
Abstract
Objective: To study the magnitude of insulin-mediated airway hyper-reactivity and to explore the protective effects of salbutamol in inhibiting the insulin-induced airway hyper-responsiveness on tracheal smooth muscle of guinea pigs in vitro.
Methods: The quasi-experimental study was conducted at the Pharmacology Department of Army Medical College, Rawalpindi, in collaboration with the Centre for Research in Experimental and Applied Medicine from December 2011 to July 2012. It used 18 healthy Dunkin Hartely guinea pigs of either gender. Effects of increasing concentrations of histamine (10-8-10-3M), insulin (10-8-10-3 M) and insulin pre-treated with salbutamol (10-6 M) were observed on isolated tracheal strip of guinea pig in vitro by constructing cumulative concentration response curves. The tracheal smooth muscle contractions were recorded with Transducer on Four Channel Oscillograph. Mean and standard error of mean were calculated. SPSS 16 was used for statistical analysis.
Results: Histamine and insulin produced a concentration-dependent reversible contraction of isolated tracheal muscle of guinea pig. The mean of maximum amplitudes of contraction with histamine, insulin and insulin pre-treated with salbutamol were 92.5±1.20mm, 35±1.13mm and 14.55±0.62mm respectively. Salbutamol shifted the concentration response curve of insulin to the right and downwards.
Conclusions: Salbutamol significantly reduced the insulin mediated airway hyper-reactivity in guinea pigs, suggesting that pre-treatment of inhaled insulin with salbutamol may have clinical implication in the amelioration of its potential respiratory adverse effects such as bronchoconstriction.
Keywords: Histamine, Inhaled insulin, Oscillograph, Tracheal muscle. (JPMA 64: 932; 2014).
Introduction
Insulin is administered through subcutaneous injections.1 Non-invasive, inhalational insulin is an attractive alternative to parenteral insulin.2 Clinical trials have shown that glucose-lowering activity of inhaled insulin is comparable to subcutaneous insulin, but with improved patient compliance.3 Its regular use is associated with fewer hypoglycaemic episodes and less risk for weight-gain as compared to subcutaneous insulin.4 Unfortunately, it was withdrawn from the market due to its respiratory adverse effects such as increased bronchial reactivity, cough, dyspnoea and bronchoconstriction. Insulin has long been recognised as a pro-inflammatory and pro-contractile hormone.5 The most likely mechanism of inhaled insulin-induced bronchoconstriction is that insulin modulates the mast cells degranulation and the subsequently increased release of histamine and contractile prostaglandins are responsible for allergic inflammation of airways.6 Some experimental evidences also reveal that it is likely to be vagally mediated, and the increased release of acetylcholine is responsible for airway hyper-responsiveness.6
Extensive research has been done to ameliorate the airway hyper-responsiveness mediated by inhaled insulin. Experimental and clinical evidences have also shown that salbutamol prevents the allergen-induced bronchial reactivity by inhibiting the release of contractile prostaglandins and histamine from mast cells via b2 receptors.7 Previous studies also reveal that salbutamol inhibits vagally-mediated cholinergic neurotransmission through heterogeneous b2 receptors and inhibits acetylcholine release.7 Keeping in view these pharmacological effects of salbutamol, the present study was designed to evaluate the efficacy of salbutamol against insulin-mediated airway hyper-reactivity of guinea pig in vitro. Considerable evidences have suggested a causal relation between our experimental setup using isolated tracheal smooth muscle and pulmonary delivery of insulin as in both cases airway smooth muscle are directly exposed to high concentration of insulin.6
The objective of the study was to determine the magnitude of insulin-induced airway hyper-reactivity and its treatment with salbutamol. Histamine is commonly used for provocative studies on airway smooth muscles. Histamine-mediated enhanced myogenic tone of airways is taken as gold standard for in vitro studies.8 To evaluate the extent of insulin-induced airway hyper-reactivity, histamine-mediated airway hyper-responsiveness was taken as standard (control) in our study and was compared to insulin-mediated tracheal smooth muscle contraction.8
Materials and Methods
The quasi-experimental study was conducted at the Pharmacology Department in collaboration with the Centre for Research in Experimental and Applied Medicine (CREAM), Army Medical College, Rawalpindi, from December 2011 to July 2012. A total of 18 healthy Dunkin Hartely guinea pigs of either gender weighing 500-700g were included through non-probability convenient sampling and were randomly divided into three equal groups using random numbers table. After approval from the institutional ethics committee, the animals were killed by cervical dislocation.8 The trachea was dissected out and the tracheal chain was prepared with smooth muscle in the centre and cartilaginous portions on both sides. The tracheal strip was attached to the hook of oxygen tube of tissue bath containing oxygenated krebs-Henseleit solution at 37°C.9 Tracheal contractions were recorded with Research Grade Isometric Force Displacement Transducer (Harvard Model No 72-4494) on four-channel oscillograph (Harvard Model No 50-9307).10
In group 1, cumulative dose-response curves of histamine were constructed with varying concentrations(10-8 to10-3M).11 When maximum response with 10-8 M concentration was obtained, the subsequent doses were added without washing the previous dose. Four-channel oscillograph was used for recording tracheal muscle contraction. This group served as control group 1 and dose-response curve of histamine was compared with that of insulin to determine the magnitude of insulin-mediated contraction, because in research studies histamine-mediated airway smooth muscle contraction is commonly taken as standard (100 percent) Ref Needed.8
In group 2, cumulative concentration-response curve of insulin was obtained using varying concentrations ranging from 10-8 to 10-3 M and the same procedure was repeated as described for histamine.6
In group 3, salbutamol sulphate (10-7 M) was added to the organ bath. After 15 minutes, cumulative dose-response curve was constructed by using varying concentrations of insulin (10-7 to 10-3 M).12
The arithmetic means of amplitudes of contractions and standard errors of mean (SEMs) were calculated using SPSS version 16. Student t test was used to determine the difference between two observations and p value of less than 0.05 was considered significant.
Results
Insulin-induced contraction of the tracheal smooth muscle was evident at a concentration of 10-7 M.However, a significant enhancement of insulin-induced contractions was observed at 10-5M, 10-4 M and 10-3 M (Figure).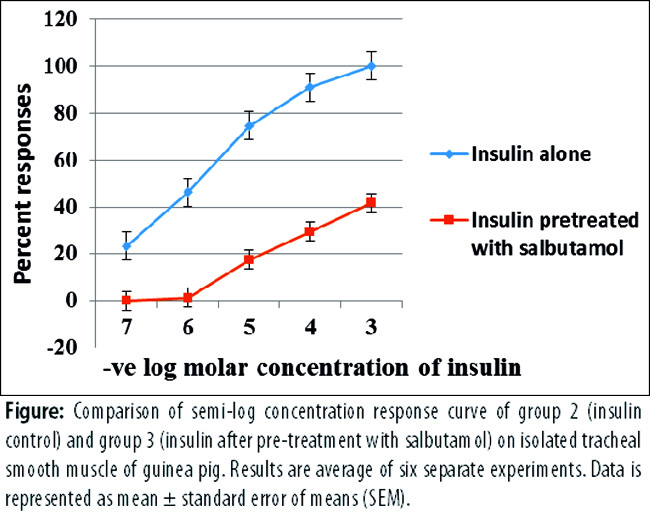
Changes in tracheal smooth muscle contractions were measured by taking the amplitudes of tracheal smooth muscle contraction. Amplitudes of contraction with maximum dose of histamine and insulin (10-3 M) were 92.5±1.20mm and 35±1.13mm respectively (Table-1).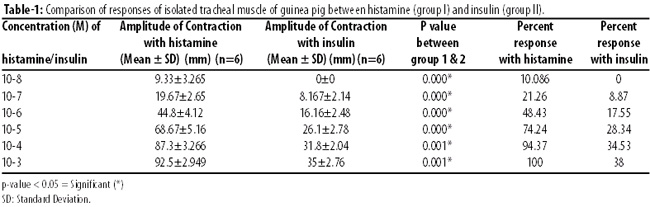
Histamine and insulin significantly enhanced the myogenic airway smooth muscle tone. To evaluate the extent of insulin-induced airway hyper responsiveness, the percentage responses for groups 1 and 2 were also calculated. Maximum constrictor response of insulin was 38 percent of maximal histamine response.
The insulin-induced tracheal smooth muscle contraction was significantly reduced in salbutamol-treated group from 35±1.13mm to 14.55±0.62mm. The means of amplitudes of contractions with varying doses of insulin when compared between group 2 and 3 were found to be statistically significant (Table-2).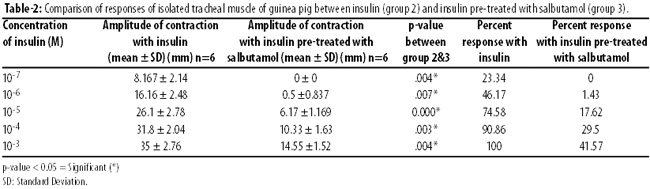
Maximum constrictor response of insulin in the presence of salbutamol (group 3) was reduced by 41.57 percent compared with insulin group. Insulin concentration response curve in the presence of salbutamol was shifted to the right and downwards, indicating a profound inhibitory effect of salbutamol on airway hyper-reactivity induced by insulin.
Discussion
The study was conducted to observe the protective effects of salbutamol against insulin-mediated airway hyper-reactivity on tracheal muscle of guinea pig in vitro. Histamine and insulin increased the airway reactivity in a dose-dependent manner. The magnitude of insulin-mediated airway hyper-reactivity was evaluated by comparing it with histamine-mediated tracheal tissue contraction as histamine-provoked airway hyper-responsiveness is taken as standard (control) for experimental studies. The maximum insulin-induced tracheal tissue contraction was 38 percent of histamine-mediated contraction (control) in contrast to 33 percent contraction which was reported in an in vitro study using the same experimental setup.6 Our results are also in accordance with in vivo studies in which airway reactivity of diabetic rats was increased after the administration of insulin due to the increased release of prostaglandins and histamine from mast cells. 13
Next, we studied the effect of salbutamol in the amelioration of insulin-induced tracheal contractions. The maximum percent response of insulin in the presence of salbutamol was reduced to 41.57 percent of insulin control. So salbutamol significantly ameliorated insulin-mediated airway hyper-reactivity. The protection offered by salbutamol is presumably through the inhibition of release of contractile prostaglandins and histamine from mast cells of isolated tracheal strip.7 The beneficial effects of salbutamol may be due to the inhibition of cholinergic neurotransmission through heterogenous b2 receptors and subsequently, decreased release of acetylcholine leads to decreased airway reactivity.14 Our observations are also supported by clinical trials in which pre-treatment of inhaled insulin with terbutaline enhanced the absorption of inhaled insulin due to the inhibition of bronchoconstriction mediated by insulin in human volunteers.15
The current study provides a clue that salbutamol can attenuate the pro-contractile effect of insulin. So pre-treatment with salbutamol may ameliorate respiratory adverse effects of inhaled insulin therapy in diabetic patients.
Conclusion
Insulin can mediate reversible contraction of isolated tracheal smooth muscle of guinea pig which was significantly inhibited by pre-treatment with salbutamol. As such, salbutamol can become a useful therapeutic agent for the amelioration of insulin-induced airway hyper-reactivity and bronchoconstriction.
Acknowledgement
We are grateful to the National University of Sciences and Technology (NUST), Islamabad for financial support.
References
1. Young RJ,Mcadam F. Treatment of Type 1 and Type 2 Diabetes Mellitus with insulin Detemir, a long acting insulin analog. Clin Med Insight Endocrinol Diabetes 2010; 3: 65-80.
2. Mollema ED, Snock FJ, Heina RJ. Phobia of self injecting and self-testing in insulin treated diabetes patients: opportunities for screening. Diabet Med 2007; 18: 671-4.
3. Bellary S, Barnett HA. Inhaled insulin (Exubera): combining efficacy and convenience. SAGE J 2007; 3: 179-85.
4. Defronzo RA, Bergenstal MR, Cefalu TW, Phillips SL, Belanger A, Bohannon NJet al. Efficacy and safety of inhaled insulin (Exubera) compared with subcutaneous insulin therapy in patients with type I diabetes: results of a 12-week, comparative trials. Diabetes Care 2005; 27: 2622-7.
5. Rosenstock J, Lorber LD, Gnudi L, Howard PC, Bilheimer WD, Chang CP, et al. Prandial inhaled insulin plus basal insulin glargine versus twice daily biaspart insulin for type 2 diabetes: a multicentre randomized trial. Lancet 2010; 375: 2244-53.
6. SchaafsmaD, Gosens R, Ris JM, Zaagsma J, Meurs H,Nelemans SA. Insulin induces airway smooth muscle contraction. Br J Pharmacol 2007; 150: 136-42.
7. Heikki K, Vesa K, Minna P, AnttiT,Hannu T. Determinants of the bronchodilation response to salbutamol on histamine-induced bronchoconstriction. Cell Physiol Biochem 2006; 100: 1760-6.
8. Hajare R, Darrhekar MV, Shewale A, Patil V. Evaluation of antihistaminic activity of piper betel leaf in guinea pig. AJPP 2011; 5: 113-7.
9. Dekkers GB, Schaafsma D, Tran T, Zaagsma J, Meurs H. Insulin-induced laminin expression promotes a hypercontractile airway smooth muscle phenotype. Am J Respir Cell Mol Biol 2009; 41: 494-504.
10. Juskova M, Franova S, Sadlonova V. Acute bronchodilator effect of quercetin in experimental allergic asthma. Bratisi Lek Listy 2011; 11: 9-12.
11. Amira E, Aziz EA, Sayed EN,Mehran GL. Anti-asthmatic and anti-allergic effects of thymoquinone on airway-induced hypersensitivity in experimental animals. JAPS 2011; 11: 109-17.
12. Yan H, Deshpande AD, Misior MA, Miles CM, Saxena H, Riemer CE, et al. Anti-mitogenic effects of ?-agonists and PGE2 on airway smooth muscle are PKA dependent. FASEB J 2011; 25: 389-97.
13. Ma YL, He QY. Study of the role of insulin and insulin receptors in allergic airway inflammation of rats. Zhonghua Yi Xue Za Zhi 2005; 85: 3419-24.
14. Barisione G, Baroffio M, CrimiE,Brusasco A. Beta- Adrenergic Agonists. Pharmaceuticals 2010; 3: 1016-44.
15. Peterson HA, Korsatko S, Kohler G, Wutte A, Olschewski H, Sparre T, et al. The effect of terbutaline on the absorption of pulmonary administered insulin in subjects with asthma. BJCP 2010; 69: 271-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: