
Muhammad Kashif Shaikh ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Bashir Hanif ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Kaleemullah Shaikh ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Waqar Khan ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
Jai Parkash ( Department of Cardiology, Tabba Heart Institute, Karachi, Pakistan. )
July 2014, Volume 64, Issue 7
Original Article
Abstract
Objective: To validate the global registry of acute coronary event (grace) risk score in a Pakistani population at Tabba Heart Institute Karachi in patients with non ST-Elevation Myocardial Infarction (NSTEMI) and Unstable Angina (UA).
Methods: In this prospective Observational registry study, 530 adults hospitalized patients with a diagnosis of Non-ST-Elevation Myocardial Infarction and unstable angina were enrolled between March 2012 and August 2012 at the Tabba Heart Institute, Karachi, Pakistan. For each patient, the grace risk score was calculated and its discrimination evaluated and correlated with in-hospital mortality using the Kendall\'s tau-b bivariate correlation test. Each patient was grouped either into high, intermediate or low risk groups according to their GRS.
Results: A total of 530 patients with NSTEMI and UA were included; the overall mean grace risk score in our population was 131.87±41.56. The GRACE Risk Score showed good discrimination, with Area under the ROC curve of 0.803 (95% CI 0.705-0.902, P < 0.001). During the in-hospital stay, total of 19 (3.6%) patients died, and out of those 15 (8.4%) patients belonged to high risk group.
Conclusion: GRACE RS strongly validates the in-hospital mortality among our patient population presenting with a wide spectrum of complications. However, more multicentre registries on a larger population with long term follow up are required to study detailed trends in our population.
Keywords: Global registry, ST-Elevation Myocardial Infarction, Unstable Angina, Pakistani population. (JPMA 64: 807; 2014).
Introduction
Acute Coronary Syndrome (ACS) refers to a spectrum of clinical presentations ranging from ST-Segment Elevation Myocardial Infarction (NSTEMI) to presentations found in Non ST-Elevation Myocardial Infarction (NSTEMI) or in Unstable Angina (UA). Patients with NSTEMI and UA carry varying risks of death and recurrent cardiac events, in short-term as well as long-term follow-up.1,2 Life-threatening cases of NSTEMI must be differentiated from other less serious cases. Several risk scores have been devised to assess the risk of serious complications in patients with NSTEMI and US. Most commonly used risk scores3-7 include Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using Integrilin Therapy (PURSUIT RS).5 Thrombolysis in Myocardial Infarction risk scores (TIMI)6 and Global Registry of Acute Cardiac Events risk score (GRACE)6 scores. This study evaluates the validation of Grace Risk Score (GRACE) and in-hospital mortality in patients with NSTEMI and UA at Tabba Heart Institute, Karachi.
The Global Registry of Acute Coronary Events is an international database designed to track outcomes of patients presenting with acute coronary syndromes, including NSTEMI and UA. The components of the Grace Risk Score (range 2 to 372) are age, heart rate, systolic blood pressure, Killip class, cardiac arrest, serum creatinine, ST-segment deviation, and cardiac biomarker status.
The Grace Risk Score, developed from a large multinational prospective patient registry, has been extensively validated and shown to be a strong predictor of in-hospital mortality across the spectrum of the population with Acute Coronary Syndrome.7-13 Because of the substantial regional variation and temporal changes in patient characteristics and management patterns, the objective of this study was to evaluate validation between the Grace Risk Score and In-hospital mortality in patients presenting with NSTEMI AND UA in Pakistani population at Tabba Heart Institute Karachi.
Patients and Methods
A prospective, observational study was conducted at Tabba Heart Institute after taking approval from Institutional Review Board. All patients (n=530) managed at Tabba Heart Institute from March 2012 to August 2012 with NSTEMI and UA were included in the study. Based on the medical data from the admission, in-hospital stay and discharge letters we derived the GRS values for each patient. All patients of age 20 or above with a presumptive diagnosis of NSTEMI and UA, defined as symptoms consistent with cardiac ischaemia and at least one of the following: abnormal cardiac biomarkers, electrocardiogram changes consistent with NSTEMI or UA, and/or a documented history of coronary artery disease were included while those with symptoms precipitated by a secondary comorbidity (eg, anaemia, thyrotoxicosis, non-cardiac trauma and non ischaemic cardiomyopathy), patients expiring in emergency room, patients declining further evaluation and patients who did not meet the inclusion criteria were excluded.
The components of the GRS were recorded on presentation.7 The acute risk of the in-hospital mortality and the assignment to the respective risk groups was calculated prospectively for these patients using the online calculator.14 The median of Grace Risk Scores was computed and its correlation with the In-hospital mortality was assessed. Further the study patients were grouped into three sub-groups according to their Grace Risk Scores: low-risk group (GRS <108), intermediate-risk group (GRS 109-140), and high-risk group (GRS >141). Statistical analysis was performed using SPSS version 15.0 (SPSS, Inc, Chicago, IL). The Kendall\'s tau-b bivariate correlation test was used to assess the correlation coefficient between the risk groups and In-hospital mortality.
Results
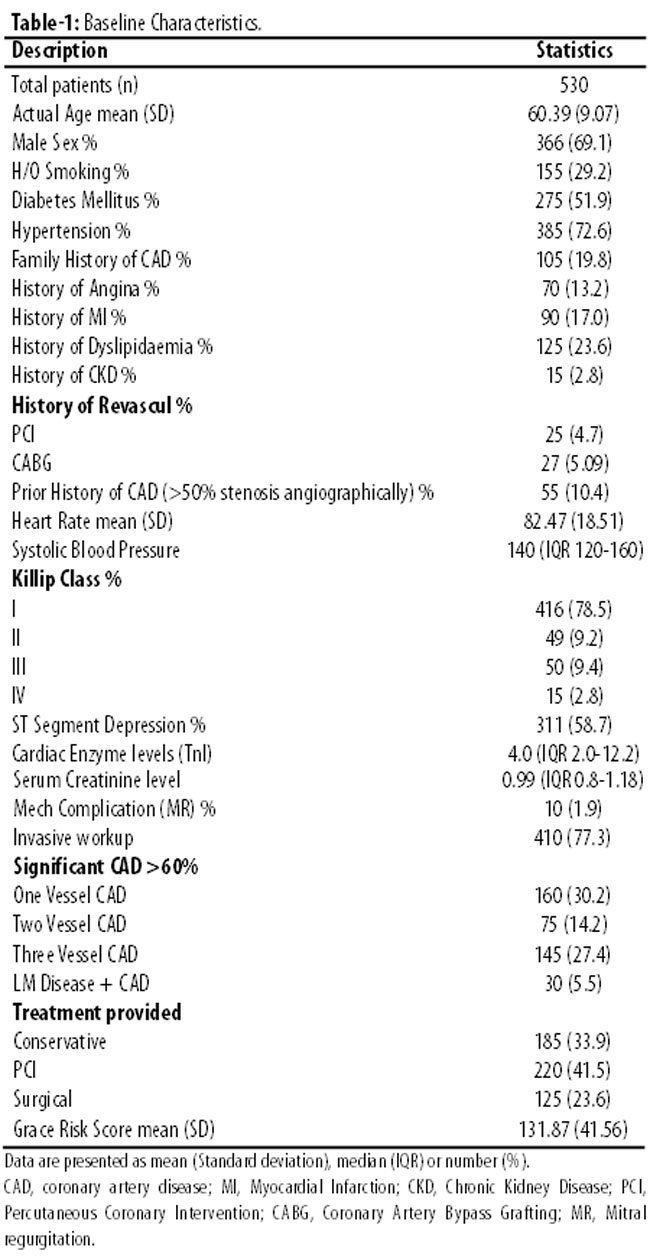
Table-1 shows the baseline characteristics, medical history and presenting clinical features of the study population and GRACE risk score. A total of 530 patients(n) with Non ST-Elevation Myocardial Infarction and Unstable Angina, were studied. The mean age was 60±0.07 years, majority were of males (366, 69.1%) and most patients had history of hypertension (385, 72.6%), diabetes mellitus (275, 51.9%), Smoking (155, 29.2%) and family history of coronary artery disease (105,19.8%). Not all the characteristics of our GRACE population resembled exactly with the original GRS derivation cohort, but somewhat close resemblance was observed in many characteristics.
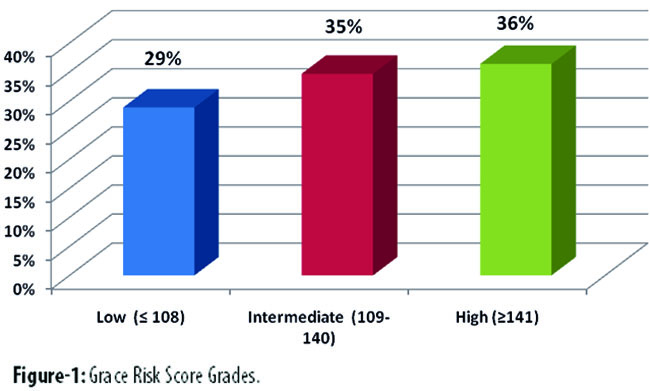
According to the calculated grace risk score, the overall mean Grace Risk Score in the population was 131.87±41.56 (Table-1). Study population was stratified according to the three risk groups, low risk group (GRS <108), intermediate group (GRS 109-140) and High risk (GRS >140) by GRACE risk score: 153 (28.9%) were classified as low risk, 184 (34.7%) as intermediate risk and 193 (36.4%) as high risk. (Table-2, Figure-1).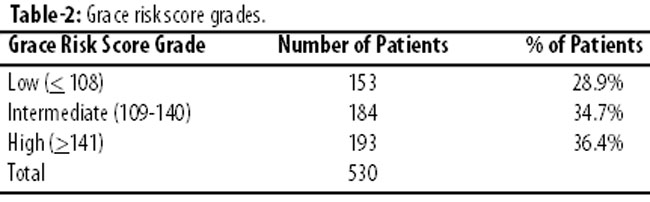
During the in hospital stay, 19 (3.6%) patients expired.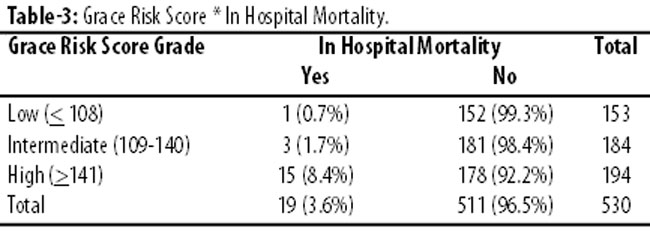
Table 3 shows the distribution of mortality during the stay in hospital, divided into low, intermediate and high-risk categories. It was observed that the mortality rate increased significantly as the risk category increased. The differences proved to be significant upon comparing total population with the risks. The trend of increasing In-hospital mortality rates in low 1 (0.7%), intermediate 3 (1.7%) and high-risk 15 (8.2%) patients was significant (p<0.001). The mortality predicted by the model approaches real values for the 3 risk categories; the approximation is much closer for the high-risk categories (Table-3). The GRACE validated model shows an adequate capacity for discrimination, with an AUC-ROC of 0.803 (95% CI, 0.705-0.902; P<.001) (Figure-2).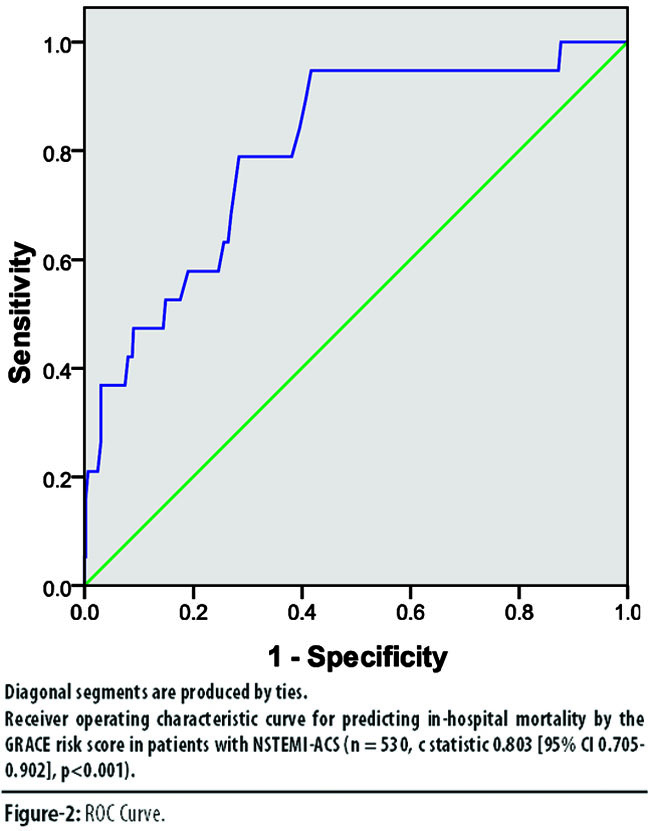
The study population showed a highly significant correlation (Kendall\'s tau-b bivariate correlation coefficient -0.152, p-value 0.003) between the level of Grace Risk Score and In-hospital mortality as shown in Table-4.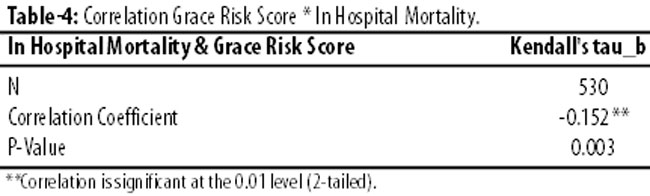
Discussion
The Grace Risk Score was derived from the large GRACE registry of patients with Syndrome (n=43810) to predict death and death or MI, both In-hospital and at six months.15-20 Clinically important observation in our study showed that the Grace Risk Score has strong accuracy in predicting In-hospital mortality in patients with NSTEMI and UA in our population also. The clinical consequences of NSTEMI and UA range from none or minimal sequelae to early death. Patients with NSTEMI and UA have a relatively high incidence of cardiac events in the short term, particularly myocardial ischaemic recurrences, recurrent angina or myocardial infarction (MI) but also heart failure, arrhythmias and other events, which may also lead to future complications.
Worldwide a number of long-term studies have also evaluated and validated the predictive value of the Grace risk score in NSTEMI AND UA. The GRACE Risk Score for predicting in-hospital death was assessed in several Acute Coronary Syndrome patient registries, the MINAP database. Bradshaw et al found that the discriminatory capacity of GRACE model was good overall (C-statistic 0.80).18 Fox Ka et al determined prediction of risk of death and myocardial infarction in the six months after presentation with Acute Coronary Syndrome via prospective multinational observational study (GRACE) and found C-statistic of 0.81 for predicting death and 0.73 for death or myocardial infarction from admission to six months after discharge which is comparable to our study (C-statistics 0.803). This study also found that GRACE score showed good predictive accuracy for the combined endpoint of cardiovascular diseases or myocardial infarction in hospital (c2 likelihood ratio 219.2, P < 0.0001, C-statistic 0.86) and the same combined endpoint at 5 years (c2 likelihood ratio 477.1, p<0.0001, C-statistic 0.68). This is the largest study analyzing the long-term survival.19
Tang et al. found that GRACE measured post discharge provided relevant prognostic factors and accurately discriminated survivors from non survivors over the longer term (up to 4 years) in all subsets of ACS patients.20 Abu-Assi et al. found that the GRACE RS for predicting in-hospital and 6-month mortality still maintain their excellent performance in patients with NSTEMI and UA.21 The Grace Risk Score demonstrates similar predictive accuracy for the In-hospital phase and long-term follow-up. Elbarouni et al. found that Grace Risk Score is a valid and powerful predictor of adverse outcomes across the wide range of Canadian patients with ACS.22 Its excellent discrimination is maintained despite advances in management over time and is evident in all patient subgroups.20-22
Eggers et al. found that the Grace Risk Score was significantly higher in patients who died (p<0.001) and provided a C-statistic regarding mortality of 0.78. Grace Risk Score allowed for the prediction of mortality in chest pain patients even after 5.8 years of follow-up.23 It is worth noting that Grace Risk Score can also be used to predict risk in low risk populations for ACS and to identify those at almost no risk of complications.24 Granger et al. shared the large GRACE registry of patients with Acute Coronary Syndrome (N=43810) derived from the GRACE risk score to predict death and death or MI, both in-hospital and at six months. Chan My et al evaluated the performance of the GRACE In-hospital mortality risk score, directly and after recalibration, in a large Singaporean cohort representing 3 major Asian ethnicities and found that In-hospital mortality after acute MI, recalibration can improve risk estimation substantially and may help adapt externally developed risk scores for local practice.25
The ability of the GRACE Risk Score to predict death at 6 months, 1, 2, 3, and 4 years was assessed also in a New Zealand ACS registry (N= 1143; all ACS, N=697; Non-ST Elevation ACS). The GRACE Risk Score worked for all 3 subsets of ACS at all time points, with C index >0.75 in all analyses.26 Our results validate GRACE Risk Score as a useful tool in the risk stratification of patients with NSTEMI and UA in our population as well as it has already been emphasized by NSTEMI and UA ACC/AHA management guidelines for early risk stratification and assisting physicians in making treatment decisions.
Limitation of Study
Despite the prospective planning of the methodology used in our study there are important aspects that should be considered as limitations. The main weakness of the study is that it is designed as a single-center analysis on a small population. There is a potential bias related to the local population characteristics, procedures and guidelines adherence. Second, we observed in-hospital outcomes of patients with NSTEMI and UA with no long-term follow-ups as yet and STEMI arm of acute coronary syndrome patients was not studied. Third, the low rate of in-hospital deaths in low-risk patients means that even small differences between the expected and the observed rates could lead to a statistically significant result, even though this probably may not be clinically relevant.
Conclusion
This study strongly proves the validity of GRACE Risk Scale of the NSTEMI and UA and Tabba Heart Institute. Therefore, we conclude that the GRACE score represents a useful and reliable clinical tool in our population for predicting the risk of death during in hospital stay in patients with NSTEMI and UA. However, more multi-center registries on a larger population with long term follow up are required to study the further detailed trends in our population.
References
1. Van Domburg RT, Miltenburg-van Zijl AJ, Veerhoek RJ, Simoons ML. Unstable angina: good long-term outcome after a complicated early course. J Am Coll Cardiol 1998; 31: 1534-9.
2. Cohen M, Antman EM, Murphy SA, Redley D. Mode and timing of treatment failure (recurrent ischemic events) after hospital admission for non-ST segment elevation acute coronary syndromes. Am Heart J 2002; 143: 63-9.
3. Calvin JE, Klein LW, VandenBerg BJ, Meyer P, Condon JV, Snell RJ, et al. Risk stratification in unstable angina. Prospective validation of the Braunwald classification. JAMA 1995; 273: 136-41.
4. Jacobs DR Jr, Kroenke C, Crow R, Deshpande M, Gu DF, Gatewood L, et al. PREDICT: a simple risk score for clinical severity and longterm prognosis after hospitalization for acute myocardial infarction or unstable angina: the Minnesota heart survey. Circulation 1999; 100: 599-607.
5. Boersma E, Pieper KS, Steyerberg EW, Wilcox RG, Chang WC, Lee KL, et al. Predictors of outcome in patients with acute coronary syndromes without persistent ST-segment elevation: results from an international trial of 9461 patients. The PURSUIT Investigators. Circulation 2000; 101: 2557-67.
6. Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, Papuchis G, et al. The TIMI risk score for unstable angina/non-ST elevation MI: a method for prognostication and therapeutic decision making. JAMA 2000; 284: 835-42.
7. Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, Cannon CP, et al. Predictors of hospital mortality in the Global Registry of Acute Coronary Events. Arch Intern Med 2003; 163: 2345-53.
8. Yan AT, Jong P, Yan RT, Tan M, Fitchett D, Chow CM, et al. Clinical trial-derived risk model may not generalize to real-world patients with acute coronary syndrome. Am Heart J 2004; 148: 1020-7.
9. de Araujo Goncalves P, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur Heart J 2005; 26: 865-72.
10. Lyon R, Morris AC, Caesar D, Gray S, Gray A. Chest pain presenting to the emergency department-to stratify risk with GRACE or TIMI? Resuscitation 2007; 74: 90-3.
11. Ramsay G, Podogrodzka M, McClure C, Fox KA. Risk prediction in patients presenting with suspected cardiac pain: the GRACE and TIMI risk scores versus clinical evaluation. QJM 2007; 100: 11-8.
12. Yan AT, Yan RT, Tan M, Casanova A, Labinaz M, Sridhar K, et al. Risk scores for risk stratification in acute coronary syndromes: useful but simpler is not necessarily better. Eur Heart J 2007; 28: 1072-8.
13. Gale CP, Manda SO, Weston CF, Birkhead JS, Batin PD, Hall AS. Evaluation of risk scores for risk stratification of acute coronary syndromes in the Myocardial Infarction National Audit Project (MINAP) database. Heart 2009; 95: 221-7.
14. CALCULATOR. (Online) (Cited 2013 Dec 13). Available from URL: http://www.outcomesumassmed.org/grace/acs_risk/acs_risk_content.html.
15. Steg PG, FitzGerald G, Fox KA. Risk stratification in non-ST-segment elevation acute coronary syndromes: troponin alone is not enough. Am J Med 2009; 122: 107-8.
16. Samaha FF, Kimmel SE, Kizer JR, Goyal A, Wade M, Boden WE. Usefulness of the TIMI risk score in predicting both short- and long-term outcomes in the Veterans Affairs Non-Q-Wave Myocardial Infarction Strategies In-Hospital (VANQWISH) Trial. Am J Cardiol 2002; 90: 922-6.
17. Bradshaw PJ, Ko DT, Newman AM, Donovan LR, Tu JV. Validation of the Thrombolysis In Myocardial Infarction (TIMI) risk index for predicting early mortality in a population-based cohort of STEMI and non-STEMI patients. Can J Cardiol 2007; 23: 51-6.
18. Bradshaw PJ, Ko DT, Newman AM, Donovan LR, Tu JV. Validity of the GRACE (Global Registry of Acute Coronary Events) acute coronary syndrome prediction model for six month post-discharge death in an independent data set. Heart 2006; 92: 905-9.
19. Fox KA, Dabbous OH, Goldberg RJ, Pieper KS, Eagle KA, Van de Werf F. Prediction of risk of death and myocardial infarction in the six months after presentation with acute coronary syndrome: prospective multinational observational study (GRACE). BMJ 2006; 333: 1091.
20. Tang EW, Wong CK, Herbison P. Global Registry of Acute Coronary Events (GRACE) hospital discharge risk score accurately predicts long-term mortality post acute coronary syndrome. Am Heart J 2007; 153: 29-35.
21. Abu-Assi E, Ferreira-González I, Ribera A, Marsal JR, Cascant P, Heras M, et al. "Do GRACE (Global Registry of Acute Coronary events) risk scores still maintain their performance for predicting mortality in the era of contemporary management of acute coronary syndromes?" Am Heart J 2010; 160: 826-4.
22. Elbarouni B, Goodman SG, Yan RT, Welsh RC, Kornder JM, Deyoung JP, et al., Validation of the Global Registry of Acute Coronary Event (GRACE) risk score for in-hospital mortality in patients with acute coronary syndrome in Canada. Am Heart J 2009; 158: 392-9.
23. Eggers KM, Kempf T, Venge P, Wallentin L, Wollert KC, Lindahl B. Improving long-term risk prediction in patients with acute chest pain: the Global Registry of Acute Coronary Events (GRACE) risk score is enhanced by selected nonnecrosis biomarkers. Am Heart J 2010; 160: 88-94.
24. Kozieradzka A1, Kami?ski KA, Maciorkowska D, Olszewska M, Dobrzycki S, Nowak K, et al. GRACE, TIMI, Zwolle and CADILLAC risk scores--do they predict 5-year outcomes after ST-elevation myocardial infarction treated invasively? Int J Cardiol 2011; 148: 70-5.
25. Chan MY, Shah BR, Gao F, Sim LL, Chua T, Tan HC, et al. Recalibration of the Global Registry of Acute Coronary Events risk score in a multiethnic Asian population. Am Heart J 2011; 162: 291-9.
26. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, et al, American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction); American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association of Cardiovascular and Pulmonary Rehabilitation; Society for Academic Emergency Medicine. ACC/AHA 2007 Guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol 2007; 50: e1-e157
27. Chan MY1, Shah BR, Gao F, Sim LL, Chua T, Tan HC, et al. Recalibration of the Global Registry of Acute Coronary Events risk score in a multiethnic Asian population. Am Heart J 2011; 162: 291-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: