
Muhammad Ilyas ( Muhammadi Hospital, Peshawar. )
Juma Gul Haidry ( Muhammadi Hospital, Peshawar. )
November 1980, Volume 30, Issue 11
Special Communication
Abstract
Some aspects of the pathogenetic puzzle of juvenile mitral stenosis have been reviewed. However, some major questions remain unanswered. How does JMS usually evolve? How long after the first attack of rheumatic fever does the opening snap develop ? What is the time lag between the development of an opening snap and the mid-diastolic murmur ? Would it be possible to interrupt the process of Juvenile mitral stenosis?.
Introduction
Pakistan is located in the geographic belt of rheumatic fever-heart disease, alongwith Mongolia, China, India, Afghanistan, Iran, Turkey, Egypt, Morocco and several other African countries. Juvenile mitral stenosis (JMS) is denned as pure or predominant mitral stenosis of rheumatic origin under the age of 20 years. Roy et al (1963) first reported the occurrence of critical mitral stenosis (less than 1 sq. cm valve area) in children and adolescents. In the school survey in Peshawar and Chitral JMS was found in 47 cases, constituting 30% of 154 cases of rheumatic heart disease (Ilyas et al., 1979). This paper reviews the prevalence data and possible etiological factors for juvenile mitral stenosis.
Prevalence
Juvenile mitral stenosis constitutes 11-30 of rheumatic heart disease in different countries located in the geographic belt of this disease (Table 1).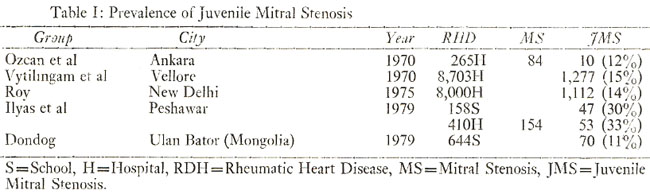
The experience of various cardiac centres in these countries regarding mitral valvotomy in the juvenile group is summarised in Table II.
Pathogenesis
The factors responsible for the development of early and significant mitral stenosis remain undetermined. It is believed that a constellation of factors, acting concurrently, contribute to this amazing and at times disastrous presentation of rheumatic heart disease. These factors include racial and ethnic influences, malnutrition, rheumatic infection at younger age, low grade persistent rheumatic activity or severe fulminating rheumatic infection, and concurrent rheumatic infection. Pronounced keloid phenomenon, notable in Afro-Asians, may in some way contribute to earlier stenosis.
National survey of rural population in India, for example, has shown that 70% of the families were taking very low protein intake, and a high percentage of these families were receiving less than 50% of the recommended allowance of riboflavin, vitamin A and ascorbic acid (Vytilingam et al., 1970).
Evidently higher incidence of carditis in rheumatic fever reported from Pakistan and India invariably implies greater number of cardiac sequelae, and this also possibly accounts for larger cases of juvenile mitral stenosis (Table III).
Higher incidence of JMS in some cases is attributed to the occurrence of rheumatic activity at younger age; 24/122 (20%) of patients hospitalised for acute rheumatic fever in Israel reported to have their first attack before the age of 5 years (Riss, 1970). On the contrary, 4 out of 245 children (1.6%) had the first attack of rheumatic fever before the age of 5 years in Thailand (Jumbala et al., 1970).
Low grade of rheumatic activity has been reported in some cases of JMS and it has been postulated that a mild course of an original rheumatic attack favours the development of pure mitral stenosis, without loss of mitral valve substance (Riss, 1970). Mori (1980) from Japan has reported that patients with mitral insufficiency often give a history of rheumatism with carditis while those with mitral stenosis rarely do so.
Ahmed (1975) from Rawalpindi has reported lower incidence of Aschoff\'s bodies in auricular biopsies in cases undergoing mitral commissurotomy, as compared to reports from Western series. Undue emphasis on this isolated report from this country can be misleading as in some reports from India higher incidence (56%) of Aschoff\'s bodies have been demonstrated (Vytilingam et al., 1970). However, no Aschoft\'s bodies were seen in auricular biopsies of 7/8 (87%) surgical cases of JMS in Ankara (Ozcan et al., 1970). Nevertheless, the prognostic significance of Aschoff\'s bodies or its role in the genesis of JMS requires elucidation.
Its absence perhaps indicates subclinical phase of the disease. However, valvotomy should not be discouraged in JMS for fear of persistent rheumatic activity, its reactivation or higher incidence of restenosis. Persistent or recurrent activity seems to have an important stenotic influence. In our series too, it was present in about 40% of cases of JMS (Ilyas et al., 1979).
In our series of 30 cases of symptomatic juvenile mitral stenosis, studied non-invasively, to determine the degree of obstruction by estimating second sound-opening snap interval phonocardiographically, severe stenosis was present in 14/30 (47%) cases, moderate in 10/30 (33%) cases and mild in 6 (20%) cases. Male to female ratio was 2:1, age range 10-20 (mean 15 years); 18 (6%) cases were 10-15 years old and 12 (40%) cases were 16-20 years old. The majority of the case s(90%) were in sinus rhythm. Evidence of recurrent or persistent rheumatic activity, as indicated by pharyngitis, raised ESR, elevated ASO titre and/or positive throat culture, was manifest in 12/30 (40%) cases. Congestive cardiac failure was present in 13/40 (42%) cases. History of rheumatic fever was available in 12/30 (40%) cases, with recurrence in 2 (7%). Time lag between episode of rheumatic fever and onset of clinical/critical mitral stenosis is not known in our series. Three interesting casuistaries are illustrated in Figures 1-4,

Acknowledgement
T am profoundly obliged to Dr. T. Strasser, World Health Organisation, Geneva, who has stimulated my interest and guided me in this field.
References
1. Ahmad, F.S. (1975) Pathology of rheumatic heart disease Auricular biopsies in mitral stenosis Rawal Med. J., 5:7.
2. Akram, M. Surgery for rheumatic fever heart disease P.M.A. Conference, Peshawar, October 1975.
3. Dondog, N. Rheumatic Fever-Heart Disease in Mongolia. WHO, CVD RF/WP/79, 32, 1979.
4. Ilyas, M., Peracha, M.A., Ahmed, R. et al (1979) Prevalence and pattern of rheumatic fever heart disease in the Frontier Province. JPMA., 29:168.
5. Ilyas, M., Shahid, M.A. and Haidry, J.G. Rheumatic fever-heart disease symposium Peshawar, October, 1979.
6. Jumbala, B., Sukuma, V., Vichipatan, P. et al. Juvenile Mitral Stenosis in Thailand. Cardiology: Current Topics and Progress New York, Associated Press, 1970, p. 184.
7. Manabe, H. (1975) Proceedings: Valvotomy in young patients with rheumatic mitral stenosis Jpn. Circ. J., 39:199.
8. Mori, C. Clinical observation on mitral stenosis in children and adolescents. Cardiology: Current Topics and Progress, New York, Associated Press, 1980, p. 181.
9. Ozcan, R. Danopulose, D. Dorken, N. et al. Severe mitral stenosis under the age of 15 years. Cardiology: Current Topics and Progress New York, Associated Press, 1970, P. 177.
10. Rahimtoola, R.J. and Rahman, H. (1975) Acute rheumatic fever in children. JPMA., 22:185.
11. Riss, O. Juvenile mitral stenosis in Israel. Cardiology: Current Topics and Progress, New York, Associated Press, 1970, p. 191.
12. Robinson, R.D., Sultana, S., Abbasi, A.S., Hashmi, J.A., Khan, A.H., Siddiqui, M. and Syed, S.A. (1966) Acute rheumatic fever in Karachi, Pakistan. Am. T. Cardiol., 18:548.
13. Roy, S.B., Bhatia, M.L., Lazaro, E.J. and Ramalingaswami, V. (1963) Juvenile mitrol stenosis in India. Lencet, 2:1193.
14. Roy, S.B. (1975) Proceedings: Challenge of Juvenile mitral stenosis in India Jpn. Circ. J., 39:198.
15. Roy, S.B. (1973) Challenge in Diagnosis of rheumatic activity, Indian Pediatrics, 10:571.
16. Shaukat Malik, M. Khan, Mushtaq Rheumatic fever in Islamabad. Proceedings IV Pakistan Pediatric Conference, 1979, p. 102.
17. Toh, C.C. (1975) Proceedings: Juvenile mitral stenosis. Jpn. Circ. J., 39:198.
18. Vytilingam K.I., Chairan, G., Sukamer, I.P. A study of juvenile mitral stenosis during 10 years period (1958-1967) Cardiology: Current Topics and Progress, New York, Associated Press, 1970, p. 188.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: