
Akhtar Ahmed ( Dept. of Neurology, Dow Medical College, Civil Hospital, Karaehi. )
November 1980, Volume 30, Issue 11
Case Reports
Abstract
Sub-acute sclerosing Pan Encephalitis (S.S.P.E.) a childhood degenerative neurologic disease has lately been proved to be caused by measles or mealses-like virus. This paper presents the first reported cases of this disease in Pakistan and it\'s features. The literature regarding aetiology is briefly reviewed.
Sub-acute Sclerosing Pan Encephalitis (S.S.P.E.), a \'degenerative\' disease of (childhood and adolescence has been the subject of great interest and investigation since the discovery that it is caused by a slow virus infection of the nervous system. This disease is considered to be synonymous with sub-acute inclusion body encephalitis (Golden and Tellez-Nagel, 1968). Between 1968 and 1969 isolation of a paramyxovirus closely related antigenically to mealses virus was reported by many workers (Golden and Tellez-Nagel, 1968; Chen et al., 1969; Horta-Barbosa et al., 1969; Katz et al., 1969; Payne et al., 1969). There are a number of interesting aspects of S.S.P.E. The nature of virus still remains unknown. It is possible that the causative virus is conventional measles-virus with unusual response of patient resulting in its protracted clinical course and long latency period of 5-13 years (Iwasaki and Koprowski, 1974). Immunologically, S.S.P.E. may be comparable to the virus-carrier culture involving defective measles virus established in Hela cells in the presence of antibody (Lege, 1967, Legg, 1969; Rustigian, 1966)-a phenomenon not yet observed in human or other animal hosts. However, the mechanism of cell damage mediated by antibody and complement may also be operating. There is as yet no evidence of immunological deficit in patients suffering from S.S.P.E. (Ristigian, 1966). Yet the virus like organism in other slow virus infections of the nervous system persists for years.
The disease has become very rare in countries where measles vaccination has been introduced effectively (Zeman, 1975). Over the past 10 years more than 25 cases probably of S.S.P.E. have been seeri in Karachi all of which were probably the cases of this condition. Seven of these cases have been adequately documented and their features are presented in this paper.
Brief Description of Disease
It is difficult to give a comprehensive description of S.S.P.E. Briefly S.S.P.E. is exclusively a disease of child-hood and adolescence with an \'incubation period\' (during which the virus does not produce manifest clinical symptoms) which may last many years. This is" followed typically by a falling scholastic performance, alteration of behaviour, and sometimes headache and impairment of speech (stage I of Kalm). The next stage (stage 2) shows gross neurological abnormalities including ataxia, dyskinesias, myoclonic jerks and typical R-complexes in EEG. Visual disturbances may be prominent at this stage. In stage 3, patient loses all mental function and may become decerebrate or opisthotonic. Even later (stage 4) all rigidity, myoclonus subside and the patient may retain only startle response, medullary reflexes and forced laughter and crying. From stage 1 to stage 4 the average duration is 2-3 years. Clinical courses lasting over 10 years have been described. High levels of measles antibody titres are found in serum and C.S.F. The description of the disease has been given by Zeman (1975).
Material and Methods
Case records of patients seen in Civil Hospital, Karachi, between 1972 and 1978 showing clinical feature of progressive encephalopathy were scrutinised. Seven adequately documented cases who had myoclonus were found to conform to the stereotyped clinical pattern and characteristic EEG findings of subacute sclerosing pan encephalitis (S.S.P.E.), with compatible CSF findings. The only other conditions which may show some-what similar EEG findinggs are Creutzfeldt-Jacob Disease and chronic progressive rubella panencephalitis (Zeman, 1975) but the clinical features are quite different because of which these diseases can be excluded.
Results

Duration of Illness:-Table II shows the duration of symptoms at the time of reporting. None had manifest symptoms lasting longer than six months.
Symptoms:-Table III lists the symptoms in these cases. They include intellectual regression, speech difficulty, abnormality of gait myoclonic jerks. Headache and vomiting occurred in 2 cases accompanied by low grade fever.
No preceding history of measles was obtained during the preceding 2 years as "epidemiological data suggests that the risk for S.S.P.E. is greatest in children exposed to wild type measles virus during an early age" (Zeman, 1975).
Neurological Abnormalities:
The neurological signs found in these cases are listed in table IV.
They include recognised features of stage 2 of the disease. Myoclonus was present in all the cases. Other features found included intellectual impairment (leading ultimately to unresponsiveness), speech difficulty, optic atrophy, weakness of voluntary power and spasticity. Decerebrate and decorticate posture developed later in 2 fatel cases.
All cases with spasticity were accompanied by extensor plantar responses. Optic atrophy was noted only in 2 cases. In others optic atrophy was not detected and pupillary reactions to light were normal. Changes of chorioretinitis were not noted in any of the cases during neurological examination although it is reported in 10-20% of cases by Zeman (1975d).
C.S.F. Findings:
The C.S.F. findings were recorded in 5 cases. There was no pleocytosis in CSF in any case. Proteins were raised in 2 cases (72 and 67 mg% respectively) and normal in other 3 cases. This is in comformity with generally accepted findings in S.S.P.E.
E.E.G. Findings:
The characteristic EEG change in S.S.P.E. is the occurrence of R-complexes described by Radermecker in 1949 (Gibbs and Gibbs, 1964). These are synchronous high amplitude slow waves that recur at intervals. These are also synchronous with periodic myoclonic jersk. Other changes in EEG are diffuse slowing and dysrhythmia which may precede appearance of R-complexes (Gibbs and Gibbs, 1964; Zeman, 1975).
R-complexes were present in all seven cases (Fig. 1,2,3 arrows).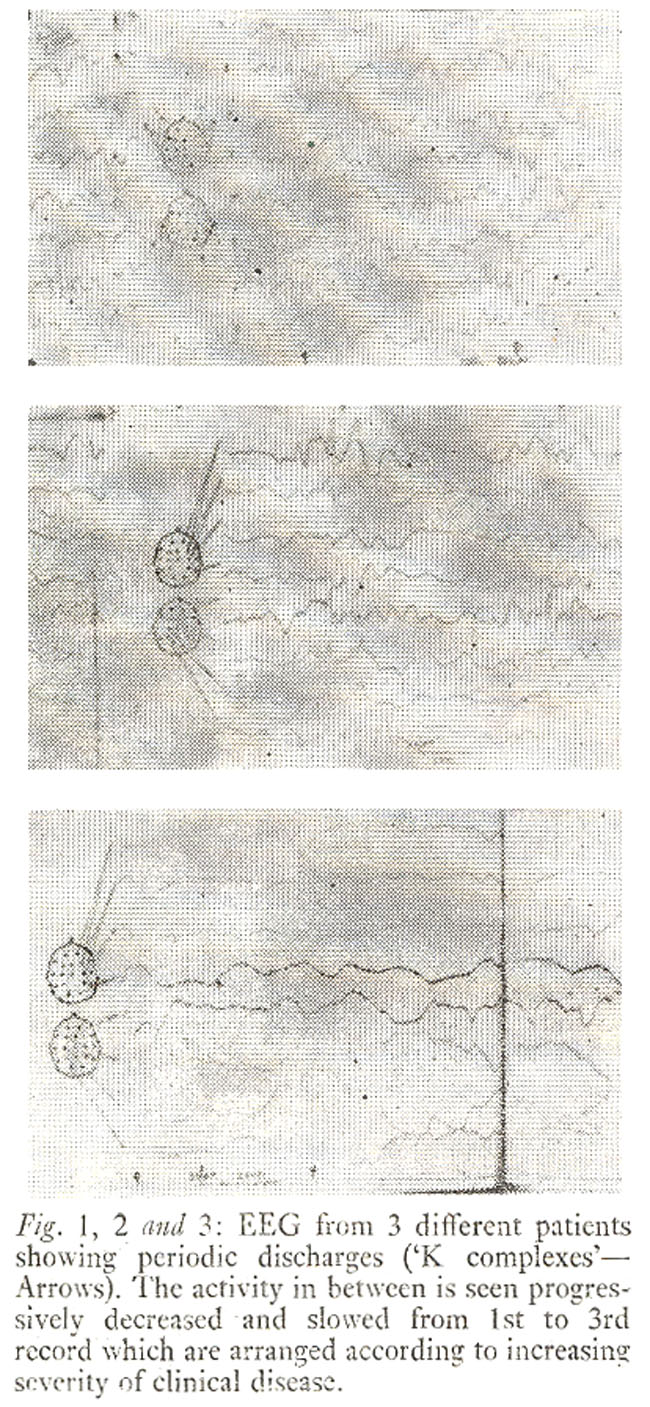
Diffuse wslowing was present in all cases. Degree of slowing was related to degree of progression of illness. Fig. 1 shows a portion of EEG recording from an 11 years old boy with 3 months history of myoclonic jerks. The child was still well oriented and able to speak reasonably well. The back ground slowing in the EEG\'s in Fig.2 and 3 that show increasing-degree of back ground slowing accompanied with grossly dis . ablingclinical. features of pain and encephalities.
Course of Disease.
One patient died after 15 months and the other after 6 months of onset of symptoms. Three cases were followed for 1, 2 and 3 months respectively before being lost to follow up. Three cases continued to deteriorate during in follow up for 1, 2 and 3 months repectively after the diagnosis.
Comments
The cases reported here show clinical features of S.S.P.E. consistent with those generally described inS.P.P.E. On an average 2 to 3 cases per year have been seen in the Civil Hospital,during the last 8-10 years which probably refects an appreicable incidence in our population which is not largely voccinsted against measles virus.
The course of illness appears much more severe in our cases. The interval between onset of overt symptoms and death has been 15 months or less in the two cases while another three appeared to be headed the same way.
References
1. Chen, T.T., Watanable, T., Zeman, W. and Measley, J. Jr. (1969) Subacute Sclerosing Panencephalitis; propagation of measles virus from brain biopsy in tissue culture. Science; 1963:1193.
2. Gibbs, F.A. and Gibbs, E.L. In Atlas of Electroencehalo-graphy, Marrachussetts, Addision wesley publishing Co., 1964, V. 3, p. 264.
3. Golden G.S. and Tellez-Nagel. I. (1968) Subacute sclerosing leukoencephalitis: Clinical and Ultrastructural studies. Bull, N.Y. Acad. Med., 44:400.
4. Horta-Barbosa, L., Fucillo, D.A., Sever, J.I. and Zeman, W. v1969) Subacute sclerosing pan Encephalitis; Isolation of measles Virus from a brain biopsy. Nature, 221:974.
5. Iwasaki, Y. and Koprowski, H. (1974) Cell to cell transmission of virus in the central nervous system. Lab. Investign., 31:187.
6. Katz, M., Oyanagi, S. and Koprowski, H. (1969) Subacute sclerosing pan encephalitis; Structures resembling myxovirus nucleocapsids in cells cultured from brains. Nature, 222:888.
7. Legg, N.J. Measles virus as an aetiological agent in encephalitis, in virus diseases of nervous system edited by C.W.M. Whitty Hughes and F.O. McCallum. Oxford, Blackwell 1969, p. 163.
8. Legg, N.J. (1967) Virus antibodies in subacute sclerosing pan encephalitis: a study of 22 cases. Brit. Med. J., 3:350.
9. Legg, N. How virus attacks nervous system, in modern trends in neurology. Edited by D. Williams. Washington, Butterworths, 1975 pp. 116-7.
10. Payne, F.E., Baublis, J.V. and Itabashi, H.H. (1969) Isolation of measles virus from cell cultures of brain from a patient with subacute sclerosing pan encephalitis. N. Engl. J. Med., 281:585.
11. Rustigian, R. (1966) Persistent infection of cells in culture by measles virus II. Effects of measles antibody on persistently infected HeLa sublines and recovery of HeLa clonal lines persistently infected with incomplete virus. J. Bacteriol., 92:1805.
12. Zeman, W. Subacute sclerosing pan encephalitis and paramyxovirus infections, in hand book of neruology. Edited by Viken, P.J. and Bruyn G.W. New York. North Holland Publishing Co, 1975, V. 133, pp. 351. 355, 357.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: