
Farakh A. Khan ( Faculty of Surygery, postgraduate Institute, Lahore. )
Salman H. Siddiqi ( Tuberculosis Research Centre Pakistan Medical Research Council, Mayo Hospital, Lahore. )
September 1981, Volume 31, Issue 9
Original Article
Abstract
Thorough investigations were carried out in 107 proven genito-urinary tuberculosis patients in the Urology Department of Mayo Hospital and Tuberculosis Research Center of Pakistan Medical Research Council. The low frequency of the disease inspite of rampant pulmonary tuberculosis was significant. Its frequency was higher in younger age subjects belonging to higher socioeconomic group. The pattern of clinical presentation varied and the only reliable diagnostic test was urine smear and culture for acid fast bacteria. The disease pattern in Pakistan has similarities with reports from India (JPMA 31:206, 1981).
Introduction
Pakistan has a high incidence of pulmonary tuberculosis and inspite of various control programmes, the problem seems to be on the increase (Roelsgard et al., 1957). Genito-urinary tuberculosis is a well known complication of the pulmonary disease and the incidence of the two, with a time gap, correlates rather well. Genitourinary tuberculosis, as an entity, has not been studied previously in Pakistan. This paper tries to highlight the disease pattern in Lahore and compares the findings with other geographical locations.
In writing this paper the authors have faced difficulties which are peculiar to the health sector in the developing countries. The major problem was to persuade the patients, often from remote areas, for a regular follow up. Regular drug therapy was also neglected in some patients. Complete investigations of some of the patients was not possible becuase of the high cost and reluctance of patients to undergo all the investigations.
Patients and Methods
During a period of 6 years all the patients who were supecteds of having genito-urinary tuberculosis were investigated in the Department of Urology of Mayo Hospital, Lahore.
Most patients were referred to by the general practitioners for their urinary complaints which could not be resolved with routine treatment. Some patients were directly picked up from the Urology Outpatient Department.
The suspected cases were clinically examined and blood Aim, blood sedimentation rate (E.S.R.), urine examination were done. The patients were sent for chest X-ray and intravenous urography. The patients were then referred to one of us for tuberculin skin testing. Standard PPD-S, 5TU (CDC) was used and 10 mm more induration was taken as positive. A sterile glass container was given to the patient along with instruction for collection of first full morning urine.
Urine smear and culture studies were then carried out on this specimen by concentration method (Siddiqi and Khan, 1980). A regular combined assessment of clinical findings and laboratory test results was done. In few selected cases cystoscopy was done.
Results
A total of 107 patients of genitourinary tuberculosis were documented between 1970 and 1976.
The criteria of diagnosis was a positive acid fast bacilli (A.F.B.) smear and or culture of urine (94 cases), a positive histopathology (11 cases) and definite clinical findings (2 cases), (Table-I).
A total of 14 culture positive cases grew atypical mycobacteria.
Age and Sex Distribution

The age of the patients as shown in Table-II ranged from 6 years to 70 years. The peak incidence was between 21 and 30 years. The maximum number of patients were between 11 and 40 years (85.04%).
There were 49 females patients (45.80%) in this series.
Economic Status
Fifty seven patients (64.04%) belonged to above average economic status. This series includes three doctors, one medical student, two nurses and two para-medical staff (Table-III).
Family History of Tuberculosis
This information was recorded in 62 patients. Only in 15 patients (24.19%) threre was a strong history of contact with tuberculosis patient in the family.
Tuberculosis at Other Sites
Out of 69 patients in whom this imormation could be established, a total of 13 patients (18.8%) gave history or were suffering from tuberculosis of other sites. In 12 of these the site was pulmonary and in one cervical lymph nodes were involved in the past.
Symptoms
The symptoms varied. No single symptom or combination of these were diagnostic of genitourinary turberculosis. At one extreme were healthy young patients with azospermia and at the other, the terminal uremics. Unusual presntation was also common. Recurrent calculous disease was one important presentation. Acute pyelonephritis was the only presenting symptom in one doctor. Nephrotic syndrome was diagnosed in 3 children. Vague urinary symptoms were noted in four patients.
Two patients suffered from diabetes as well. Two other had tuberculous pyonephrosis. In this series there were 8 patients with renal failure (Blood urea over 50 mg percent).
The list of symptoms are given in Table IV.
The analysis of duration of symptoms (Table-V) shows that majority of patients presented within 2 years of onset of symptoms (57.97%).
Investigations on Admission
Urine Examination:
In 75 patients who were investigated, pyuria with or without haematuria was the most frequent finding. The results are show in Table-VI.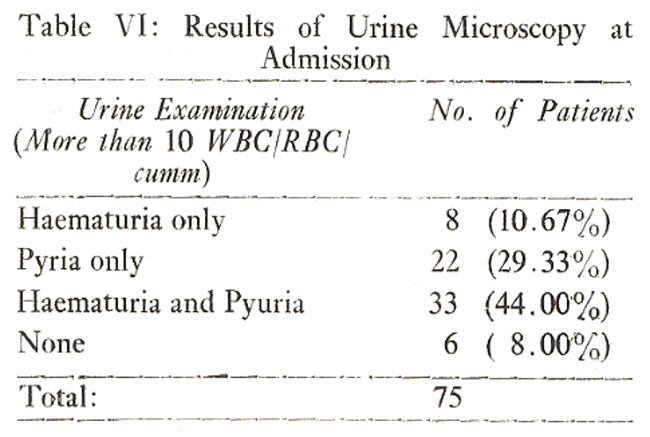
Normal E.S.R. was recorded in 19 patients. The lowest was 2 and the highest 135 mm in the first hour (Table VII).
Tuberculin Test
A total of 43 patients were tested forPPD-S. Eight patients had negative response, while 35 gave a positive reaction (measuring 10 mm or more induration). The highest response was 50 mm.
Intravenous Urography
This was done in 77 patients. It was found to be within normal limits in 20 patients. In 57 patients a single or combination of findings were recorded (Table VIII).
In a total of 22 patients there was evidence of stone disease in the past or at admission. In seven patients stones had been removed in the past and 15 patients had X-ray evidence.
Cystoscopy
This was done in 12 patients. No specific diagnostic feature could be observed. Generalised cystitis with patchy distribution was a common feature. Stenosis of ureteric orifice was seen in 4 patients. In 11 patients no abnormality was detected. In 4 patients retrograde catheterisation was done to locate the site of stricture. In two patients the bladder capacity was too small for a satisfactory view of the bladder. In one of these cases the thin bladder was ruptured and suprapubic repair had to be done.
Operations
Operative treatment was undertaken in 10 patients. The operations performed are given in table IX.
Discussion
In the Department of Urology at Mayo Hospital, on an average, 17.8 new cases of genitourinary tuberculosis were documented every year. This is much lower in contrast to centres in the developed countries where the yearly patient intake is higher. Gow (1970) reporting from England had an admission rate of 43.7 patients per year, Petkovic (1967) from Yugoslavia 79.1 per year, and Shabad (1975) from U.S.S.R. 58.1 per year. Our study has thus shown that genitourinary tuberculosis is uncommon in Pakistan. The low frequency is particularly significant because pulmonary and other forms of extra pulmonary tuberculosis is rampant in the country (Roelsgard et al., 1957, Siddiqi 1973).
The reason for this unusually low incidence of urologic disease in Pakistan is not clear. One obvious factor seems to be the poor diagnostic facilities in the country. However, the late complications of the disease, especially pyonephrosis, which would draw the attention of the surgeon are also uncommon. The Department of Pathology in our institutin received only one specimen of tubercular pyonephrosis over last three years. Khan (1972) reported only 4 cases of genitourinary tuberculosis in 2 years, in his series of 210 cases of extra pulmonary tuberculosis seen at the Department of Pathology in Khyber Medical College, Peshawar. It is also possible that because of poor medical facilities number of pulmonary tuberculosis patients die before renal tuberculosis reaches an advanced stage presuming, of course, that the former is the primary source of the haematogenous spread to the urinary tract. The association of pulmonary and extra pulmonary tuberculosis seems to be rather strong. Singh (1975) repored an incidence of genitourinary tuberculosis in 15 percent of patients with bone and joint and 25 percent of pulmonary tuberculosis. In the present series 17.4 percent of patients also had associated pulmonary tuberculosis. However, we do have a large population of treated pulmonary tuberculosis patients similar to the developed countries and we thus conclude that longivity of pulmonary tuberculosis patients is not the full explaination for the low incidence of genitourinary tuberculosis in Pakistan.
The above arguments make us feel that perhaps other factors are responsible for the poor predilaction of these organisms to the genitourinary tract in our patients. The host susceptibility, virulence and difference of organism are perhaps the most important ones. In our series it is significant that geuitourinary tuberculosis is more common in the higher income groups and especially in the healthy persons. These patients, unless in advanced stages, look apparently healthy in sharp contract to the pulmonary tuberculosis patients. The nutritional status may be linked with the excretion of tuberculostatic factors in the urine (Tsuji 1965). Racial peculiarities may also be important in this respect. Bruce (1970) reporting from the western region of Scotland found only 12 cases of Indo-Pakistan origin out of a total of 534 patients. Carruthers (1970) reported high incidence of pulmonary and extra pulmonary tuberculosis among the Asian immigrants (comprising 61 percent and 78 percent of the total patients respectively). However, only 13 percent Asians in his series had genitourinary tuberculosis. It is thus possible that georacial factors may be of importance.
Organism virulence may also be an important factor. There is some evidence of geographical variation in organism virculence in pulmonary tuberculosis patients (Mitchison 1964). Though this work has not been done in our patients, we nevertheless feel that this factor is perhaps the most important in explaining the low infectivity rate in Pakistan.
The pattern of bacteriological status of patients has been discussed in detail in another paper. (Siddiqi and Khan 1980).
The patterns of age group is similar to that of India (Singh 1975) and pre-antibiotic period in the developed countries (Shahd 1975). Other authors from Great Britain show a higher incidence in older age groups (O\'Flynn 1970, Broth-wick 1970).
The clinical presentation of the patients was remarkably variable. We feel strongly that a good laboratory support is essential for the diagnosis. The presentation of nephrotic syndrome in 3 children with renal tuberculosis was unusual. The incidenae of epididymitis (10 patients) in this series is much higher than quoted by western sources (Gow 1971), although the Indian figures are more in line with ours (Singh 1975). Tubercular urethritis as a presenting symptom was uncommon in our series (2 patients). One of these patients developed stricture of the membranous urethra with multiple perineal fistulae. Urethral involvement, though rare, has been described (Symes and Blandy, 1973 and O\'Flynn 1970).
The symptom variability was at extremes. This may partly be due to the wide range of duration of symptoms prior to diagnosis. Health conscious patients were diagnosed at a very early stage whereas people from the rural areas particularly, reported years after the disease was established. Here again host parasite relationship perhaps finally determines the severity of the damage to the genito-urinary system. We feel that the disease if diagnosed, with laboratory support, within 6 months of onset of symptoms would save the patient from late complications. However, there is a group of patients with minimal symptoms who would enevtually be diagnosed for the first time only when the disease is advanced with clearcut sysmptoms. This pattern is now being emphasised as a problem even in countries with advanced health care system (Petrovic 1975, Ioanid and Galesanu 1976).
History of contact with open pulmonary tuberculosis patients is of limited value in our environment. The incidence of sputum positive tuberculosis is high, and the chances of exposure at early age is also common.
The routine clinical and laboratory diagnostic aids have substantial limitations. E.S.R. readings were generally on the low side with normal values in 19 patients. The high readings were obtained in advanced stages where secondary pyogenic infection was an important feature. On urine microscopy 6 patients did not show any haematuria or pyuria. Haematuria and/or pyuria was noted in 92 per cent of patients. Thus haematuria and/or pyuria is an important symptom. Tuberculin tests also gave us low readings as compared to pulmonary tuberculosis patients. In 19 patients negative responses were illicted. This investigation is of limited value in our patients since a high percentage of normal population is tuberculin positive (Siddiqi 1973).
Intravenous Urography findings were variable but in large number of cases ureteric strictures were noted (21 patients) which were mainly confined to the lower end of the ureter. Frequency of strictures at this site is well known (Gow 1970, Rees 1970, Claridge 1970, Gow 1971, Feldstein iet al 1975 O\'Boyle et al 1976). Calcification and/or stone in the urinary tract was also an important feature in 15 cases and in another 7 cases there was a history of stone removal operation. Thus a total of 20 patients suffered from calcification/stone disease. The incidence of calcification/stone formation given by other authors vary from 2.6 to 34 per cent (Ross 1970). Figures as high as 50 per cent have been quoted by Ioanid and Galesann (1976). In Pakistan stone disease is common (Khan 1973) and we feel tuberculosis may well be an important factor in recurrent stone disease. In one case calcification of the left seminal vesicle was noted. Ross (1970) found calcification of seminal vesicles (8 cases) as the second most common site after the kidney in his series. Segmental dialatation of the lower ureter was a feature in three cases.
Cystoscopy, in 21 patients, did not substantially help in the diagnosis of the disease since no specific finding could be correlated to the tubercular involvement of the bladder. In the small contracted bladder there is a risk of bladder rupture which occured in one patient.
Urine culture for A.F.B. was the most important single investigation in establishing the diagnosis but it has its limitations. In one case 14 specimens were cultured before a positive growth was obtained although urine was repeatedly positive for A.F.B. smear. Here we believe tuberculostatic factors may have been responsible for this phenomenon. Another aspect to be reckoned with is the tuberculostatic properties of certain antibiotics administered for pyogenic infections. These would also reduce the chances of a positive culture and perhaps change the clinical presentation of the disease. Atypical mycobacteria were grown in 14 patients. The high incidence of atypical mycobacteria isolated in our series is comparable to the report from India (Singh et al 1975). It was our impression that the infection by these organisms is usually limited to the kidney and tends to be less damaging.
The patients were treated with Streptomycin, INH and PAS in the early stages of this study. We then encountered a high INH and Streptomycin resistance in pulmonary tuberculosis patients. Furthermore the large number of PAS tablets were found to be a deferent for the patients and a substantial number were not taking the therapy regularly and thus other antitubercular drugs were prescribed. Two of our patients relapsed while on the above regemin. Relapse after completion of drug therapy (Butler and O\'Flynn 1975) has so far been noted in two patients. We feel Ethambutol, inspite of its cost, is an excellent substitute for P.A.S.
In recent years drug combination of Rifam-picin, Isoniazid and Pyrazinamide have been advocated with better results (Gow 1980).
Our operative approach is rather conservative. Ten patients under-went oprations with one death (ureterosignoidostomy patient died 6 months after the operation). We are not in favour of surgery unless the complications hinder in the patient\'s recovery after anti-tubercular treatment.
References
1. Borthwick, W.M. (1970) Present position of urinary tuberculosis. Br. J. Urol., 42:542.
2. Butler, M.T. and O\'Flynn, J.D. (1975) Reactivation of genito-urinary tuberculosis. Eur. Urol., 1:14.
3. Carruthers, R.K. and Long, S.V. (1970) Genitourinary tuberculosis in an area with a large Asian immigrant population. Br. J. Urol., 42:535.
4. Claridge M. (1970) Ureteric obstruction in tuberculosis. Br. J. Urol., 42:688.
5. Feldstein, M.S., Sullivan, M.J. and Banowsky, L.H. (1975) Ureteral involvement in genitourinary tuberculosis. Urology, 6:175.
6. Gow, J.G. (1970) Results of treatment in a large series of cases of genitourinary tuberculosis and the changing pattern of the disease. Br. J. Urol., 42:647.
7. Gow, J.C. (1971) Genitourinary tuberculosis. A study of the disease in one Unit over a period of a 24 years. Ann. R. Coll. Surg., 49:50.
8. Gow J.G. (1979) Genitourinary Tuberculosis: A 7-year review. Br. J. Urol., 51:239.
9. Ioanid, P.C. and Galesann, M. (1976; New aspects of urinary tuberculosis, Eur. Urol. 2:185.
10. Khan F.A. (1973) History of calculous disease of urinary tract. J. P.M. A., 23:19.
11. Khan S.B. (1972) Non-pulmonary tuberculosis, progress Med., 1:47.
12. Mitchison, D.A. (1964) The virulence of tubercle bacilli from patients with pulmonary tuberculosis in India and other countries. Bull. Int. Un. Tuberc, 35:287.
13. O\'Boyle,P.J., Galli, E.M. and Gow, J.G. (1976) The surgical management of tuberculosis lower ureteric stricture. Br. J. Urol., 48:101.
14. O\'Flyn, D. (1970) Surgical treatment of genitourinary tuberculosis,\'A report on 762 cases. Br. J. Urol., 42:667.
15. Petkovic S. Ilic V. Sumarac Z. and Markovic, V. (1969) Renal tuberculosis in the antibiotic era. Urol. Nephrology, 1:9.
16. Petkovic S. Sumarac Z. Petronic V. and Markovic V. (1975) Destructive forms of renal tuberculosis. Eur. Urol., 1:81.
17. Rees, R.W. and Hollands F.G. (1970) The ureter in renal tuberculosis. Br. J. Urol., 42:693.
18. Roelsgard, E. Cristensen N. and Iversen E. (1957) B.C.G. vaccination programme in Pakistan. Bulletin World Health Organization, pp. 187-202.
19. Ross, J.C. (1970) Calcification in genitourinary tuberculosis. Br. J. Urol., 42:656.
20. Ruce, L.G. (1970) The incidence of genitourinary tuberculosis in the western region of Scottland. Br. J. of Urol., 42:637-641.
21. Shabad, A.L. (1975) New features in the pathogenesis of renal tuberculosis and their significance for its detection. Urol. Int., 30:297.
22. Siddiqi, S.H. and Stauffer J.C. (1973) Tuberculin sensitivity to PPD-S and three Aytpical Antigens in Pakistan. Pakistan J. Med. Res., 12:11
23. Siddiqi, S.H. and Niaz, N. (1976) Bovine Tuberculosis in Pakistan. Proceeding of Jinnah Postgraduate Medical Symposium Karachi.
24. Siddiqi S.H. and Khan F.A. (1980) Bacteriological study of renal tuberculosis in Pakistan JPMA., 30:257.
25. Singh S.M., Raju, B.V., Wadhwa, S.N., Shriniwas and Bajaj, J.S. (1975) Genitourinary tuberculosis in Northern India. J. A.I.I.M.S., 1:20.
26. Symes, J.M. and Blandy, J.P. (1973) Tuberculosis of the male urethra. Br. J. Urol., 45:432.
27. Tsujj, S., Oshima, S., Fujita, Y., Okada, N. and Nakashima, M. (1965) Isolation from human urine of a polypeptide having marked tuberculostatic activity. Am. Rev. Respir. Dis., 91:832.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: