
Sher Muhammad Khan Paindakhel ( Nuclear Medicine Division, Institute of Radiotherapy and Nuclear Medicine Peshawar. )
Muhammad Ilyas ( Muhammadi Hospital, Peshawar. )
August 1981, Volume 31, Issue 8
Original Article
Abstract
In a series of 102 digitalised patients serum digoxin levels (SDL) were determined by radioimmunoassay (RIA). Age categorisation included juveniles (15%), adults (67%) and geriatrics (18%). Clinical categorisation included loading, adequate, inadequate, toxic, and borderline digitalisation groups. The mean SDL in the toxic-group was 3 .93 ng/ml (S.D. 1.40), and in the non-toxic group 1.27 ng/ml (S.D. 0.84). In the toxic group with high SDL, palpitations (39.3%), vomiting (35.7%), nausea (21.5%), anorexia (17.8%) and hiccough (10.7%) were the commonest manifestations of digoxin intolerance (JPMA 31:161, 1981).
Digoxin is the most widely used cardiac glycoside for patients with cardiac decompensation. Varying incidence of digoxin intolerance has been reported but with careful dose adjustment the frequency of its toxic effects can be reduced (Doherty, 1973; Storestein et al., 1977; Takahashi et al., 1979). Despite extensive clinical use the critical evaluation of its side effects remains a diagnostic problem mainly because of the narrow margin between therapeutic and toxic doses, and also because of nonspecificity of gastrointestinal side effects. Different methods for estimation of serum digoxin concentration have been used including erythrocyte rubibium 86 method (Lowenstein and Corrill, 1966), double isotope dilution assay and gas liquid chromatography (Watson and Haber, 1971). Radioimmunoassay (RIA) for digoxin has been the most recommended procedure (Smith et al., 1969). Serum digoxin levels estimated by RIA are reported in this study.
Material and Methods
The series consists of 102 consecutive patients taking digoxin (70 males and 32 females). Their ages ranged from 8 to 95 years (mean 50-3 years). Age subcategorisation included:
Adults: 69 (67%): 21-69 years old (mean 48.5 years)
Juvenile:15 (15%): 8-20 years old (mean 14 years)
Geriatrics. 18 (18%): 70-93 years old (mean 77.2 years).
Out-patients and in-patients receiving digoxin for cardiac failure associated with coronary, hypertensive or rheumatic heart disease were included in the study. History of heart disease and digoxin intake was obtained and a twelve lead electrocardiogram was taken. Clinical criteria of digoxin toxicity included nausea, vomiting, anorexia, weakness, yellow vision, slow pulse, palpitations and electrocardiographic evidence of ectopic beats, tachycardia or conduction disturbances.
Serum digoxin estimation was carried out by the radioimmunosassay (Smith et al., 1969), using digoxin RIA Kit (Radiochemical Centre, Amersham, England), and serum digoxin level (SDL) was expressed as millimicrogram per-milliter (ng/ml).
Results
The results, in various clinical group with SDL correlation, are shown in Table I.
Group A-Loading Group
A group of 9 patients (7 males and 2 females), 23-80 years old (mean age 52.2 years), received loading dose of digoxin 1.5 mg on the first day, administered orally in 7 caes and intravenously in 2 cases, one tablet digoxin (0.25 mg) was given on the following morning and serum samples were obtained by the mid day.
Group B-e Digit alhation
The clinically adequately controlled group of 25 patients with cardiac failure (16 males and 9 females), age range 21-69 years (mean 45.4 years )was taking 0.5 mg digoxin daily.
Group C-Inadequate Digitalisalion
Digitalisation was considered inadequate in a group of 10 cases of cardiac failure not satisfactorily controlled with the standad dosage of digoxin 0.5 mg/day (9 males and 1 female) 22-69 years old (mean 52.5 yeas).
Group D-Toxic Group
This group included 19 cases with signs and symptoms suggestive of digoxin toxicity (10 males and 9 females), 22-68 years old (mean 50 years). Except one case who had adequate SDL (2.07ng/ml.), all the other cases had high SDL ranging 2.75-8.0 ng/ml (Table I).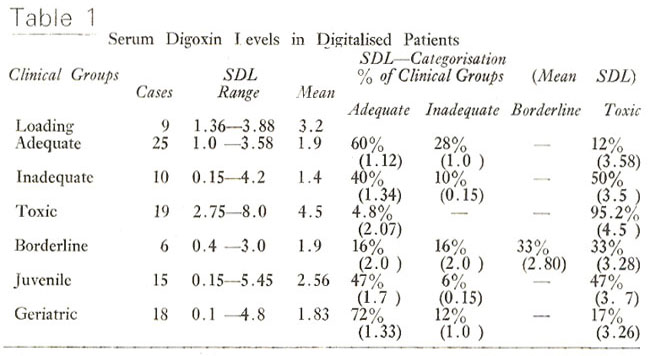
Group E-Borderline Group
In a group of 15 juvenile cases (10 males and 5 females), 8-18 years old (mean 14 years), receiving 0.25-0.5 mg digoxin/day (mean 0.392 mg/day), SDL ranged from 0.15-5.45 ng/ml.
Group G-Geriatric Group
In 18 geriatric cases (15 males and 3 females), 70-93 years old (mean 77 years), receiving 0.5 mg digoxin per day, (excepting one case receiving 0.25 mg/day), SDL ranged 0.1-4.8 ng/ml.
Comparative Data of this and other series for toxic and non-toxic groups of patients is shown in Table-II.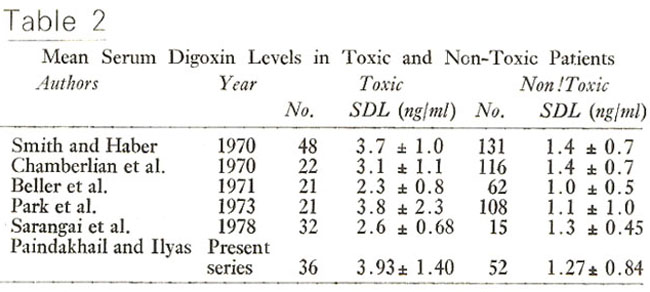
In 6 cases (3 males and 3 females), age range 35-68 years (mean 54.5 years), with borderline clinical presentation of toxicity only two cases (33%) had borderline toxic SDL.
Group F-fuvenile Group
In a group of 15 juvenile cases (10 males and 5 females), 8-18 years old (mean 14 years), receiving 0.25-0.5 mg digoxin/day (mean 0.392 mg/day), SDL ranged from 0.15-5.45 ng/ml.
Group G-Geriatric Group
In 18 geriatric cases (15 males and 3 females), 70-93 years old (mean 77 years), receiving 0.5 mg digoxin per day, (excepting one case receiving 0.25 mg/day), SDL ranged 0.1-4.8 ng/ml.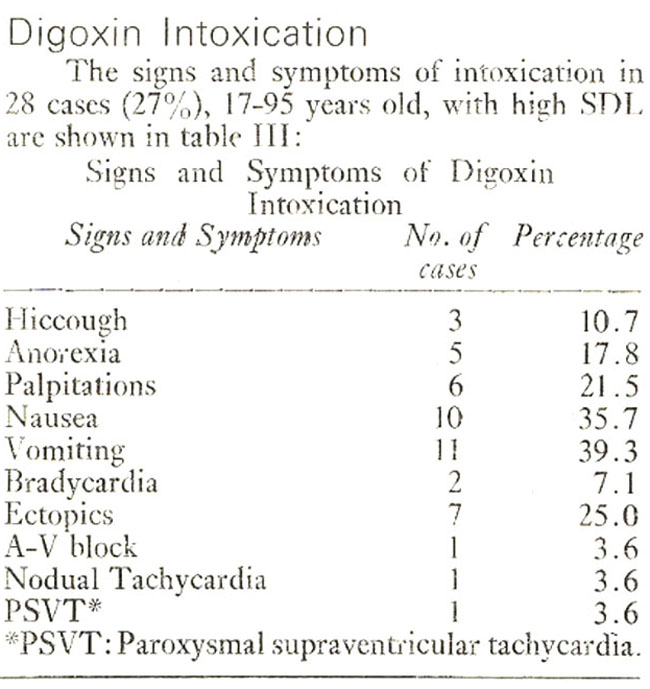
Comparative Data of this and other series for toxic and non-toxic groups of patients is shown in Table-II.
Discussion
This study has demonstrated the usefulness of serum digoxin estimations and significant differences in SDL (P<0.005) between toxic and non toxic patients were observed. Similar differences have been reported by other workers (Chamberlian et al., 1970; Smith and Haber, 1970; Park et al., 1973; Sarangai et al., 1980). However, in a number of borderline cases a degree of overlap exists between toxic and nontoxic serum digoxin levels.
In the present series and in several other reports (Park et al., 1973; Schaolin et al., 1980), it has been observed that serum digoxin levels of 2ng/ml best discriminated toxicity with minimum overlap. In addition to identification of digoxin toxicity, radioimmunoassay also detects patients who may be underdigitatlised. However, a serum digoxin level is of limited value in differentiation of toxic from non-toxic patients and correlation with clinical data is mandatory (Shapiro, 1978).
Serum digoxin estimation requires special care in the pediatrics and the geriatirc groups. Due to a possible decrease in end organ sensitivity in infancy serum digoxin levels of more than 3ng/ml. are frequently found in the non-toxic group, while children over 1 years of age resemble the adult of group with non-toxic levels less than 3 ng/ml. (Greenwood et al., 1977). In the elderly group, mean serum digoxin concentration in patients with definite digoxin intoxication has been reported as 3.16 ng/ml (Suzuki and Ogawa, 1980).
Renal function has an important influence on serum digoxin concentration and a close relationship has been demonstrated between urea, creatinine and digoxin clearance (Dobbs et al., 1977; Singh et al., 1975). A degree of correlation has also been demonstratred between digoxin levels and different cardiac arrhythmias (Singh et al., 1975).
References
1. Chamberlain, D.A., White, R.J., Howard M.R. and Smith, T.W. (1970) Plasma digoxin concentration in patients with atrial fibrillation. Br. Med. J., 3:429.
2. Dobbs, S.M. Rodger, E.M. Kenyon, W.I. et al. (1977) Digoxin prescribing in perspective. Br. J. Clin. Pharmacol., 4:327.
3. Doherty, J.E. (1973) Digitalis glycosides; pharmacokinetics and their clinical implications. Ann. Intern. Med., 79:229.
4. Greenwood, H., Howard, M. Landon, J. et al. (1977) Development of a highly sensitive radioimmunosassay for digoxin and its application in pediatric practice Euro. J. Cardiol., 5413.
5. Lowenstein, J.M. and Corrill, E.M. (1966) An improved method for measuring plasma and tissue concentrations of digitalis glycosides. J. Lab., Clin. Med., 67:1048.
6. Park, H.M. Chen, I.W., Manitassas G.J. et al. (1973) Clinical evaluation of radiommunosassay of digoxin J. Nucl. Med., 14:531.
7. Sarangi, A., Tripathy, R, Lal, D. Patnaik, B.C. and Swain, A.K. (1980) Study of serum digoxin status in digitoxicity by radioimmunosassay Am. Heart J., 99:289.
8. Schaolin, C, Jiming, T. and Zhonglun, S. et al. (1980) Clinical significance of plasma estimation by radioimmunosassay Chinese J. Cardiol., 9:19.
9. Shapiro, W. (1978) Correlative studies of serum digitalis levels and the arrhythmias of digitalis intoxication. Am. J. Cardiol., 41:852.
10. Singh, R.B., Dube, G.P. and Dube K.P. et al. (1975) Cardiac manifestations of digoxin intoxication. Clinical Correlation with serum levels Acta Cardiol., 30:85.
11. Smith, T.W., Butler, V.P. Jr., and Haber, E. (1969) Deter mination of serum digoxin concentration by radioimmunosassay. N. Engl. J. Med., 281:212.
12. Smith, T.W. and Haber, E. (1970) Digoxin intoxication; the relationship of clinical presentation to serum digoxin concentration. J. Clin. Invest., 49:2377.
13. Storestein, O., Hansteen, V., Hatle, D. et al. (1977) Studies of digitalis XIII. A prospective study of 649 patients on maintenance treatment with digitoxin Am. Heart J. 93:434.
14. Suzuki, M. Ogawa, D. (1980) Clinical studies on digoxin intoxication. Serum Concentration of digoxin in the elderly of and the effect of disease Jpn. Heart J. 21:341.
15. Takahashi. M., Sadda, T. Taneichi, Y. et al. (1979) Some observations on serum concentration of digixon and digoxin Jpn. Heart J. 20:623.
16. Watson, T.W. and Haber, W. (1971) Assay of digoxin in plasma by gas chromatography J. Chromatogr., 56:209.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: