
Nabeel Dastgir ( Department of Trauma and Orthopaedics, Mid Western Regional Orthopaedic Hospital, Croom, Co Limerick, Ireland. )
June 2014, Volume 64, Issue 6
Original Article
Abstract
Objective: To explore the effect of extracorporeal shock wave therapy in patients with chronic plantar faciitis.
Methods: The prospective study was conducted at Department of Orhopaedic, Regional Hospital, Limerick, Ireland from January to December 2004 and comprised 70 heels in 62 patients with chronic plantar fasciitis in whom conventional conservative treatment consisting of non-steroidal anti-inflammatory drugs, heel cup, orthoses and/or shoe modifications, local steroid injections had failed, and they were treated with low energy extracorporeal shock wave therapy. Patients were reviewed at 6, 12 and 24 weeks post treatment.
Results: At follow-up there was significant decrease in pain on the visual analogue scale (p<0.027), with significant improvement in pain score (p<0.009) and in functional score (p<0.001). The comfortable walking distance had increased significantly and there were no reported side effects.
Conclusion: Extracorporeal shock wave therapy is a new modality providing good pain relief and a satisfactory clinical outcome in patients with chronic plantar fasciitis.
Keywords: Plantar Fasciitis, Extracorporeal shock wave therapy. (JPMA 64: 675; 2014)
Introduction
Plantar fasciitis is a common clinical problem which may occur both in athletes and in general population. The specific pathological feature of this clinical entity is not yet well understood. Inflammation of the plantar fascia, thinning of the proximal fascia, loss of normal elasticity and alteration of nociceptor physiology all may play role in the pathogenesis of plantar fasciitis.1 There is strong tendency of spontaneous resolution but in proportion of patients a chronic syndrome may develop and further treatment may be required.2 A variety of conservative treatments have been proposed for this condition. Apart from weight reduction and rest, various orthotic devices, heel pads, non-steroidal anti-inflammatory drugs (NSAID), topical application of steroids, injection of steroid into the painful area also have been used. A small percentage of patients ultimately had open release of plantar fascia, but results were not always predictable or satisfactory.3
Although the application of low-energy extracorporeal shock wave therapy (ESWT) to treat musculoskeletal disorders is controvertial, but there has been some limited evidence of its effectiveness in the treatment of chronic plantar fasciitis. The aim of this study was to explore the effect of ESWT in patients with chronic plantar fasciitis.
Patients and Methods
The prospective study was conducted at Department of Orhopaedic, Regional Hospital, Limerick, Ireland from January to December 2004. During the study period 70 heels were treated in 62 patients with chronic plantar fasciitis. The inclusion criteria for the study was heel pain resistant to all conservative treatment provided for a period of at least six months. These patients were seen in the outpatient clinic of the orthopaedic department. The exclusion criteria was presence of local arthritis, generalised polyarthritis, rheumatoid arthritis, ankylosing spondylitis, Reiter syndrome and history of previous attempt of open release of plantar fascia. All patients were given a single dose of Ibuprofen 400mg two hours prior to the treatment. Additional treatments like NSAIDs or orthotics were not continued. Standard plain radiographs of the affected heels were taken to document the presence/absence of calcaneal spur. Approval for this study was taken from the hospital ethics committee. All ESWT were given according to a standardised protocol. All patients were positioned prone on the bed. Ultrasound gel was put over the heel and the focus of shockwave treatment area was localised with the help of ultrasound (Figure). Each patient received 2500-3000 impulses. Energy level was between 11-15 N/sq.m. Each patient had three sessions of ESWT in three weeks. Pre and post treatment subjective and objective scoring systems were used (Table-1).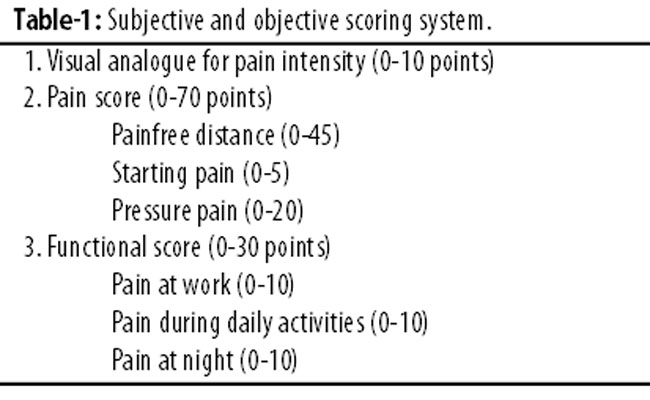
Follow-up evaluation was at 6, 12 and 24 weeks. All the 62 patients were followed up for 24 weeks.
Results
Of the 100 patients initially enrolled, 32 (32%) males and 30 (30%) females (8 (8%) patients had bilateral heels) met the inclusion criteria. The mean age was 39±5 years (range: 25-51).
At 24 week follow-up there was significant decrease in pain on the visual analogue scale [VAS] (p<0.027), with significant improvement in pain score (p<0.009) and in functional score (p<0.001). The comfortable walking distance has increased significantly. There were no adverse effects/complications. Overall, there was statistically significant improvement in all the subjective and objective scoring systems (Table-2).
Discussion
Plantar fasciitis is a common orthopaedic syndrome. The cause of this clinical entity remains enigmatic. The specific pathologic features are not well understood; inflammation of the plantar fascia, thickening of the proximal fascia, decreased vascularity, peritendinous inflammation, loss of normal elasticity, and alteration of nociceptor physiology all may play roles in the onset and persistence of heel pain.1,2 The clinical diagnosis of plantar fasciitis is relatively easy to make. Radiographically, a heel spur on the inferior surface of the calcaneus frequently is evident, but is not considered pathognomonic of the disorder3 Magnetic resonance imaging (MRI) regularly shows oedematous involvement of the calcaneal insertion of the plantar aponeurosis, with a marked thickening of the proximal segment of the central cord of the plantar fascia.4-7 Although proximal plantar fasciitis is the most frequent cause of inferomedial heel pain, but other pathologic conditions, such as seronegative arthropathies or nerve entrapment, may be causal in about 10% of cases. The pain is usually present when the patient first stands on his or her feet after awakening and it persists or becomes worse with activities of daily living. The use of non-operative methods such as rest, application of ice to the sore area, NSAIDs, or topical application of steroids will alleviate the condition in most patients. A stretching protocol is regarded as the mainstay of non-operative treatment. A meta analysis,8 looked for randomised controlled trials on plantar fasciitis and found 11studies on non-operative treatment since 1966.2 However, these trials had low methodological assessment scores; not a single one evaluated the effectiveness of surgical therapy. The meta analysis showed there was limited evidence for the short-term effectiveness of topical corticosteroid and for the effectiveness of use of dorsiflexion night splints. When conservative treatment has failed, surgical release of the plantar fascia has been undertaken with variable result. Treatment of chronic plantar fasciitis with low-dose extracorporeal shockwaves is relatively new. The first paper reporting favourable results after application of shock waves for the treatment of painful heel syndrome was published in 1996.9 Positive outcomes have been confirmed in other studies as well.2,9,10 The term "shockwave" denotes a high-energy sound wave that terminates in a bursting of energy similar to a mini- explosion. It is essentially the same as a supersonic jet breaking the sound barrier and creating an energy force strong enough to shatter windows. ESWT utilises a high peak pressure ranging from 5 to 130Mpa, with a most common energy of 50Mpa and a broad frequency of 14Hz to 20MHz. The most significant aspect of this unique form of energy is the rapid initial rise in pressure amplitude (500 bar) over a short lifecycle of less than 10ns. The action of ESWT is the result of a process called cavitations, which is like the formation and movement of bubbles in a quid. Strong forces exerted in the region of a moving bubble cause mechanical tissue disruption. The repair of the mechanical tissue disruption is the theoretical basis for the neovascularisation process and subsequent pain relief following ESWT.18,19 In order for ESWT to be therapeutic, the energy should be focused at the point of existing pathology.
Although the mechanism of ESWT disintegration of renal calculi is well understood,2 the current mechanism of ESWT in the treatment of musculoskeletal disorders is not fully appreciated. Some have used an analogy of creating micro trauma to the tissues with an effect similar to tenderising meat. The mechanism of pain relief is attributed to a release of enzymes, which effect nociceptor, much like the action of transcutaneous electrical nerve stimulation (TENS). More importantly, studies have shown that neovascularisation occurs following the application of ESWT.4-7 The painful process in plantar fasciitis is a local inflammatory reaction which leads to stimulation of the central nervous system (CNS) via ascending pain pathways. It is believed that hyper stimulation of the painful spot by shockwaves cause activation of descending inhibitory fibers at brain stem level. This could lead to a control of transmission through the dorsal horns as well as at higher levels in the somatic projection system and thus to suppression of pain. The long-lasting pain relief after a short period of hyper stimulation could be due to a change of pathologic moving patterns.9 A satisfying clinical outcome after application of low-energy extracorporeal shock waves was first reported in patients with chronic tendinitis of the elbow.10 The study showed comparable short-time results for patients with plantar fasciitis and a heel spur.10 Similarly positive outcomes have been confirmed in clinical studies from various university hospitals.11 Another study reported good or excellent results, according to the modified Roles and Maudsley score, in 36 of 48 heels at 29 months. The clinical outcome was not influenced by the duration of the follow-up period. No negative side effects were reported.6 Wang et al.12 reported that 33 of 41 patients were either free of symptoms or substantially better at 12 weeks after the therapy Ogden et al.13 performed a randomised, placebo-controlled study with 119 patients in the treatment group and 116 patients in the placebo group. Twelve weeks after a single application of 1500 high-energy shockwaves at 18kV with the patient under regional anaesthesia, the result was successful in 47% of the patients. The success rate after the sham treatment was only 30%. This study led the United States Food and Drug Administration to approve shock-wave therapy for painful heels. Chen at al.14 studied 80 patients treated with 1000 shockwave impulses at 14kV. Of the 54 patients who were evaluated at six months, 59% had no symptoms and 27% had substantial improvement. In other studies radial extracorporeal shockwave therapy was found to be safe and effective in the treatment of plantar fasciitis.15,16 In a recent study Yucel I et al17 compared the results of corticosteroid injection and ESWT. They found both treatments to have similar good results, but corticosteroid injection was cost-effective compared to ESWT. In our study each patient received 2500-3000 impulses on first treatment. Energy level was between 11-15 N/sq.m. Each patient had three sessions of therapy in three weeks. Pre- and post-treatment subjective and objective scoring system showed statistically significant improvement in all scoring systems. None of the outcome variables in our study was free from the possibility of observer bias, although this risk was kept low by making sure that an independent observer evaluated the patients before and after treatment. Pain, however, may be influenced by many factors and is difficult to measure.
Conclusion
ESWT is a new therapeutic modality in the treatment of patients in the chronic plantar faciitis. It is safe and effective and has produced a high rate of success in pain relief and functional restoration.
References
1. Malay DS, Pressman MM, Assili A, Kline JT, York S, Buren B, et al. Extracorporeal shockwave therapy versus Placebo for the treatment of chronic proximal plantar fasciitis: results of a randomized, placebo-controlled, double-blinded, multicenter intervention trial. J Foot Ankle Surg 2006; 45: 196-210.
2. Gerdesmeyer L, Frey C, Vester J, Maier M, Weil L Jr, Weil L Sr, et al. Radial extracorporeal shockwave therapy is Safe and effective in the treatment of chronic recalcitrant plantar fasciitis. Am J Sports Med 2008; 36: 2100-9.
3. Schepsis AA, Leach RE, Gorzyca J. Plantar fasciitis. Etiology, treatment, surgical results and review of the literature. Clin Orth Relat Res 1991; 266: 185-96.
4. Berkowitz JF, Kier R, Rudicel S .Plantar fasciitis: MR imaging. Radiology 1991; 179: 665-7.
5. Grasel RP, Schweitzer ME, Kovalovich AM, Karasick D, Wapner K, Hecht P, et al. MR imaging of plantar fasciitis: Edema, tears, and occult marrow abnormalities correlated with outcome. Am J Roentgenol 1999; 173: 699-701.
6. Maier M, Steinborn M, Schmitz C, Stäbler A, Köhler S, Pfahler M, et al. Extracorporeal shock wave application for chronic plantar fasciitis associated with heel spurs: prediction of outcome by magnetic resonance imaging. J Rheumatol 2000; 27: 2455-62.
7. Narvaez JA, Ortega R. Painful heel: MR imaging findings. Radiographics 2000; 20: 333-52.
8. Crawford F, Atkins D, Edward J. Interventions for treating plantar heel pain (Cochrane Review), in Cochrane Library, Issue 3. Oxford, Update Soft-ware, 2000.
9. Melzack R. Prolonged relief of pain by brief, intense transcutaneous somatic stimulation. Pain 1975; 1: 357-73.
10. Rompe JD, Hopf C, Nafe B, Burger R. Low-energy extracorporeal shock wave therapy for painful heel. A prospective controlled single-blind study. Arch Orthop Trauma Surg 1996; 115: 75-9.
11. Lowell SW Jr, Thomas SR, Lowell SW Sr, Anthony HB, et al. ECSWT for treatment of Chronic Plantar Fasciitis. J Foot and Ankle 2002; 41: 166-72.
12. Wang CJ, Chen HS, Chen WS, Chen LM. Treatment of painful heels using extracorporeal shock wave. J Formos Med Assoc 2000; 99: 580-3.
13. Ogden JA, Alvarez R, Levitt R, Cross GL, Marlow M. Shock wave therapy for chronic proximal plantar fasciitis. Clin Orth Relat Res 2001; 387: 47-59.
14. Chen HS, Chen LM, Huang TW. Treatment of painful heel syndrome with shock waves. Clin Orthop Relat Res 2001; 387: 41-6.
15. Ibrahim MI, DonatelliRA, Schmitz C, Hellman MA, Buxbaum F.Chronic plantar fasciitis treated with two sessions of radial extracorporeal shockwave therapy. Foot Ankle Int 2010; 31: 391-7.
16. Leach RE, DiIorio E, Harney RA. Pathologic hindfoot conditions in the athlete. Clin Orthop 1983; 177: 116-21.
17. Yucel I, Ozturan KE, DemiraranY, Degirmenci E, Kaynak G.Comparison of high dose extracorporeal shockwave therapy and intralesional corticosteroid injection in the treatment of plantar fasciitis. J Am Podiatr Assoc 2010; 100: 105-10.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: