
Muhammad Tariq Farman ( National Institute of Cardiovascular Diseases Karachi, Pakistan. )
Tahir Saghir ( National Institute of Cardiovascular Diseases Karachi, Pakistan. )
Nadeem Hasan Rizvi ( National Institute of Cardiovascular Diseases Karachi, Pakistan. )
Jawaid Akbar Sial ( Chandka Medical College Hospital, Larkana, Pakistan. )
Naveedullah Khan ( National Institute of Cardiovascular Diseases Karachi, Pakistan. )
Abdul Malik ( Lady Reading Hospital, Peshawar, Pakistan. )
Khan Shah Zaman ( National Institute of Cardiovascular Diseases Karachi, Pakistan. )
June 2014, Volume 64, Issue 6
Original Article
Abstract
Objective: To determine the safety and efficacy of selective thrombus aspiration during Primary Percutaneous Coronary Intervention (PCI).
Methods: This observational prospective study was conducted in the catheterization laboratory of a tertiary care cardiovascular centre. A total of 150 consecutive patients who underwent primary PCI were enrolled. Aspiration was done only when thrombus burden was considered significant. After completion of procedure angiographic and electrocardiographic signs were recorded and clinical follow up was documented up to 1 year.
Results: No significant difference among the groups was found in age, height, weight and other risk factors like Hypertension, Diabetes Mellitus and Smoking. In general, left anterior descending artery was culprit in ~ 65 % of patients and more than 90 % of culprit vessels had visible thrombus. Multivessel disease was present in 38 % of patients and 22.7% had past history of myocardial infarction. Out of 150 patients 117 (78%) underwent thrombus aspiration. No significant difference was found in ST resolution within 60 minutes (72.6 vs 81.8 %; P<0.285) and myocardial blush grade II & III (41.9 vs 27.3 %; P<0.128). No difference in event free survival was observed among the two groups (80.3 vs 84.8 %; P<0.708) at one year.
Conclusion: Selective thrombus aspiration in definite thrombus laden arteries and no aspiration in low or negligible thrombus burden vessels may be a safe and effective strategy in patients undergoing primary PCI. Overall poor risk profile of our patients as compared to western population necessitates further evaluation of this matter in randomized studies.
Keywords: Acute ST elevation myocardial infarction, Priamry percutaneous coronary intervention, Aspiration thrombectomy. (JPMA 64: 653; 2014).
Introduction
Primary percutaneous coronary intervention (PCI) is the established and preferred mode of treatment for ST segment elevation myocardial infarction (STEMI) and has proved more effective in opening the infarct related occluded artery.1,2 Along with other adjuvant treatment manual thrombus aspiration is considered feasible and reasonable for patients undergoing primary PCI.3,4 Although death, reinfarction and target vessel revascularization (TVR) rates were not significantly different at 30 days but at 1 year, rates of cardiac death and nonfatal reinfarction were significantly lower with thrombus aspiration.5,6 However, among low risk patients in whom thrombus burden is either absent or negligible, the role of aspiration thrombectomy is not known. We designed this study to answer this question that whether aspiration thrombectomy should be the mainstay of the Primary PCI irrespective of thrombus burden or should it be reserved for the high risk group of patients in whom clot burden is definite? Considering the fact that most of the expenses of Primary PCI in our setup has to be borne by the patients (who are usually poor), it becomes very important to answer this question. In patients with low thrombus burden, avoiding aspiration thrombectomy will make primary PCI cost effective for most of our averaged income patients. Whether this practice is judicious and safe? This study aims to give us a rationale to advocate this practice.
Our secondary objective was to compare our data with the western model to find out any demographic and procedural difference that may affect the outcome of primary PCI.
Patients and Methods
This observational, prospective, single centre study was conducted at a tertiary care cardiovascular teaching hospital from January 1st 2009 to October 31st 2010. All adult patients (>18 years old) with chest pain lasting > 30 minutes and ST elevation of >1mm in >2 contiguous leads were included in this study. Informed consent was taken and detailed questionnaire was filled of those patients who agreed for primary PCI.
Patients who received Thrombolytic therapy within 24 hours of hospital admission, those who were diagnosed as Non ST elevation Myocardial Infarction (NSTEMI) and those presenting beyond 24 hours with resolved symptoms were excluded from the study.
Procedure: Primary PCI was performed in standard method using a variety of guiding catheters, coronary wires, balloons and stents. The majority of interventions were performed through the femoral route. However, the choice of access was on discretion of operators and considerable number (18%) of interventions was performed through radial route. All patients received 5000-10,000 units of intravenous unfractionated heparin, Aspirin 300mg, clopidogrel 600mg (loading dose), and Platelet glycoprotein IIb IIIa inhibitor. Thrombus extraction catheter (Export catheter 6-F; Medtronic corporation, USA) was used when obvious clot was visible in the infarct related artery (thrombus class 2-5). Proximal to distal continuous aspiration was done while advancing the device into the culprit artery. Suction was provided by hand with a lockable 20 ml syringe that allows for a suction rate of 1 ml/second. No aspiration was done when clot was not obvious (thrombus class 0 & 1). Intracoronary nitroprusside and adenosine use were at the discretion of operators. All patients were prescribed Aspirin 300mg, Clopidogrel 75mg and Atorvastatin 20-40mg / Rosuvastatin 10-20mg daily at the time of discharge from the hospital.
Data collection: The prospective information on variables including age, gender, history of diabetes, hypertension, hyperlipidaemia, Smoking, angiographic and procedural details (number of vessels, segment of vessel, use of aspiration catheter, clot retrieval, use of stents, GP IIb IIIa inhibitors, Thrombolysis in Myocardial Infarction (TIMI) flow, and Tissue Myocardial perfusion (TMP) grade and Electrocardiogram (ECG) findings were recorded.
TIMI flow, TMP grades and ST resolution (on 12-lead ECG strips) were visually determined and documented by two independent observers before and after PCI and in case of controversy third expert opinion was taken as final. These observers were blinded about the use of aspiration thrombectomy.
Angiographic analysis and Definitions: Intracoronary thrombus was classified as: zero - No thrombus, 1 - reduced contrast density / possible thrombus, 2 - small size thrombus / greatest dimension <½ of vessel diameter, 3 - moderate size thrombus / greatest dimension > ½ and <2 vessel diameter, 4 - large size thrombus / >2 vessel diameter, 5 - total occlusion.7
PCI success was defined as achievement of vessel patency to a residual <30%. Major bleeding was defined as a hematoma >10cm in diameter or bleeding requiring transfusion, vascular surgery or resulting in major morbidity.
TIMI flow grades were defined as: Zero - total occlusion resulting in no antegrade flow, 1 - minimal penetration of contrast across the obstruction but fails to opacify the vessel, 2 - contrast opacifies the vessel beyond the occlusion but with delay, 3 - normal complete perfusion of entire vessel without any delay.8
TMP grades were defined as: Zero - minimal or no myocardial blush, 1 - dye stains the myocardium and this stain persists on the next injection, 2 - dye enters the myocardium but washes out slowly and strongly persists at the end of injection, 3 - normal entrance and exit of dye in the myocardium.9
Complete ST resolution was defined as >70% ST resolution compared to baseline ECG. No ST segment resolution was defined as persistent ST segment elevation or <30% resolution of ST segment.10
Patients were followed in out patient department (OPD) after one month, and at 1 year. Those patients who could not come in OPD, they were contacted through telephone and follow up documented.
Statistical Analysis
All the data was entered and analyzed through SPSS version 17. Categorical variables like gender, diabetes, hypertension, smoking, history of previous MI, cardiogenic shock, inotropic support, IABP, infarction territory, route of access etc. were presented in frequencies and percentages. Whereas continuous variables like age, height, weight, BMI, symptom onset to ER and door to balloon time were presented as mean ± SD. Chi square test was used for significant association. Independent t-test for normally distributed data and Mann Whitney U test were used for not normally distributed data to compare mean (±SD) values of with and without aspiration of thrombus. Pvalue <0.05 was considered as statistically significant.
Results
Out of 150 patients enrolled, 117 (78%) were aspirated for thrombus retrieval. Baseline demographic, clinical and angiographic features of both groups were nearly the same (Table-1).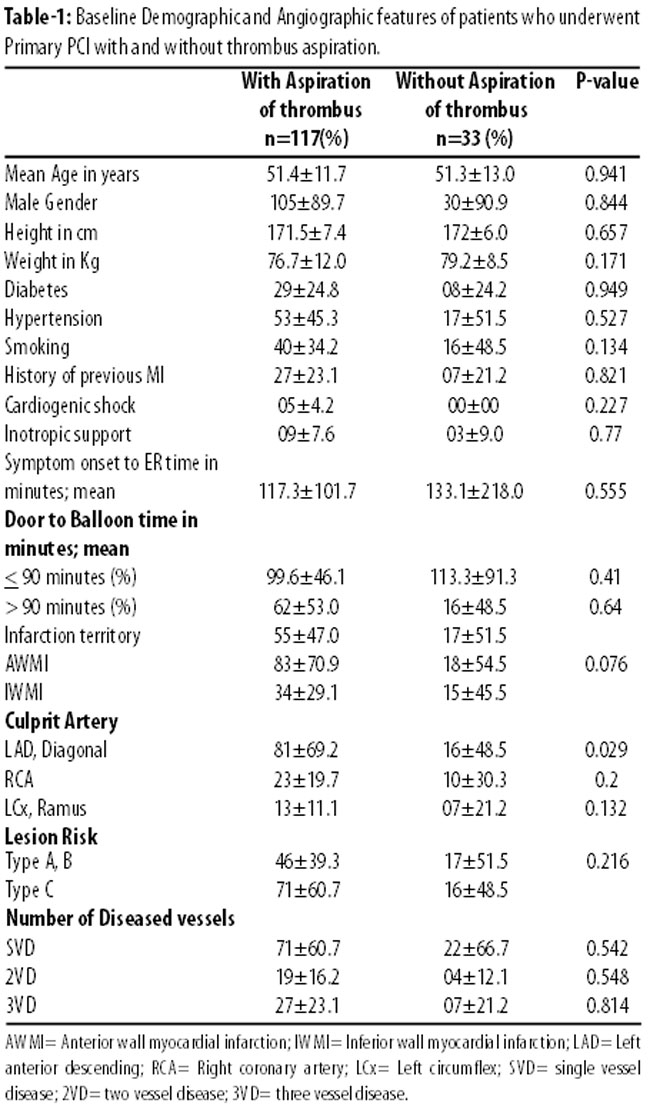
However, aspiration catheter was more frequently used in patients with AWMI as compare to IWMI but this difference was not significant (70.9% vs 29.1%; p<0.07). Moreover, LAD artery was found culprit in majority of patients (~ 64%).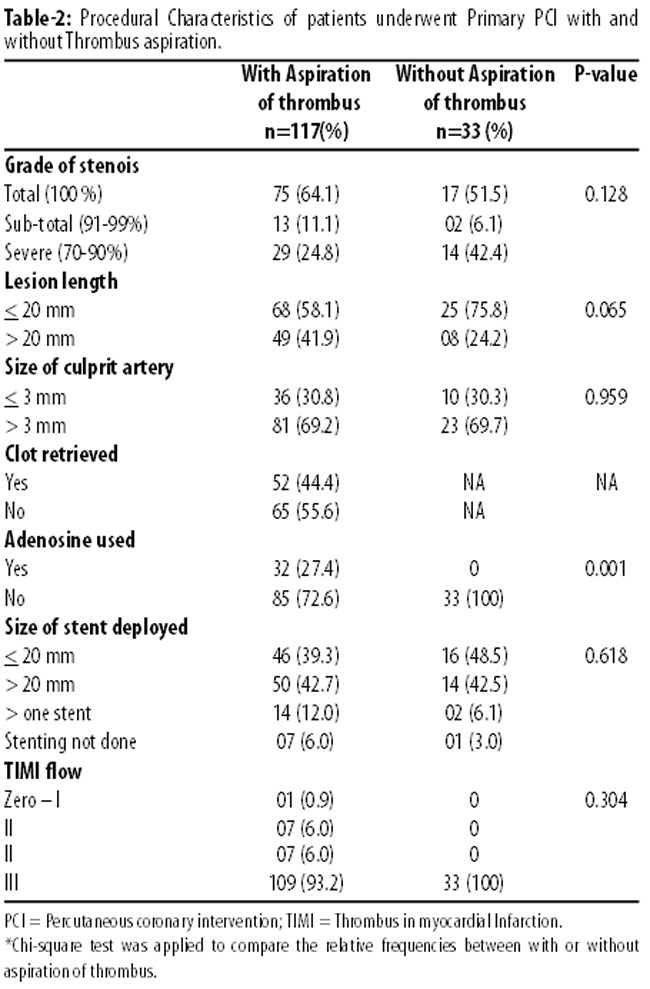
Table-2 showing procedural characteristics of patients who underwent primary PCI with and without thrombus aspiration. Patients with diffuse lesions (length of >20mm) were aspirated more as compare to patients with non diffuse lesions (85.9% vs 73.1%; p<0.06). Patients underwent thrombectomy with aspiration catheter frequently had adenosine and none of the patients had adenosine in whom aspiration catheter was not used.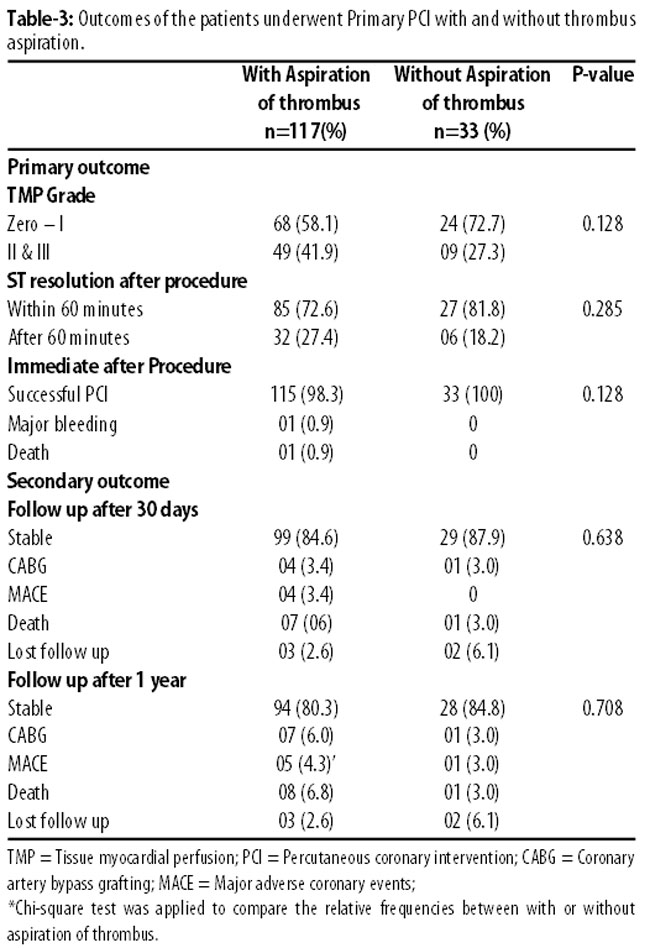
Table-3 showing outcomes of patients who underwent primary PCI with and without thrombus aspiration catheter. No significant difference was found among the two groups at immediate, 30 days and 1 year follow up.
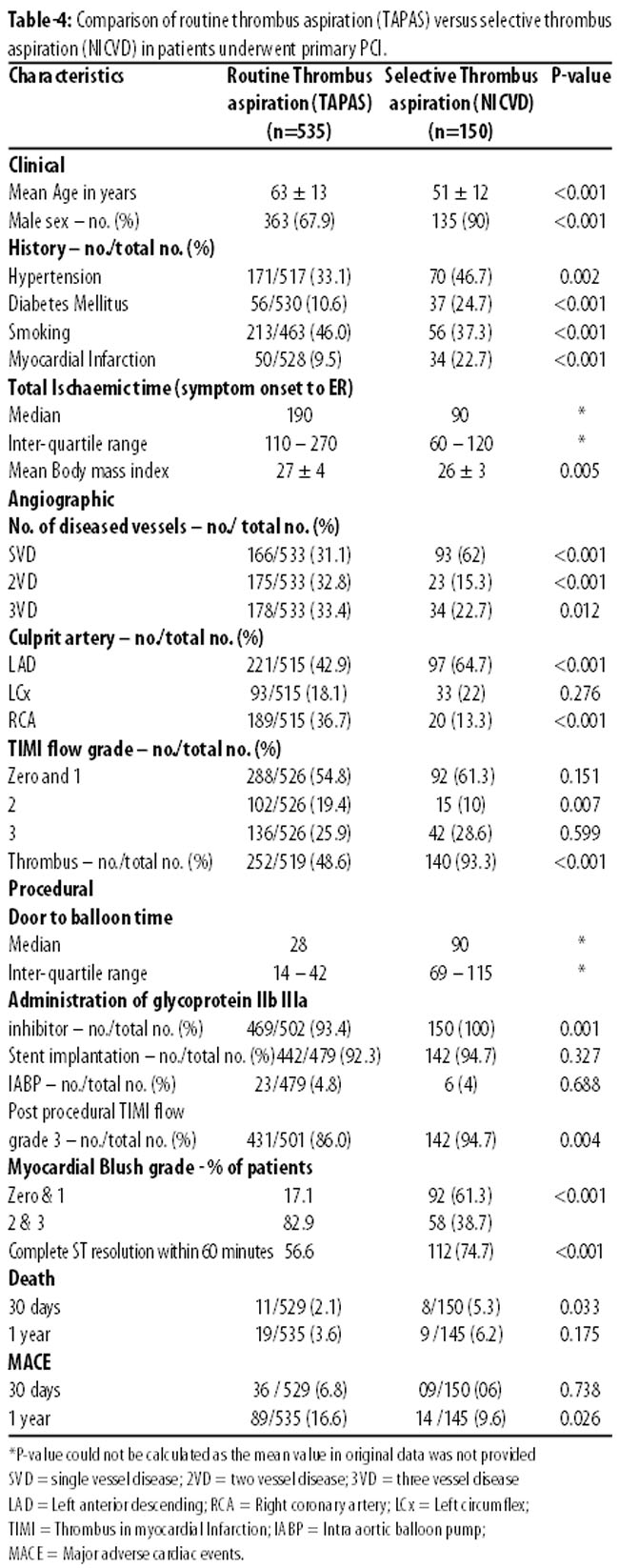
Table-4 shows the comparison of our data with TAPAS land mark study. Significant difference in age and risk factors profile was observed among both the study population. SVD is common in our study population contrary to Multivessel disease that was commonly seen in European study. LAD was the most common culprit artery in our setup, while disease pattern was distributed among different vessels in TAPAS. Angiographically visible thrombus was also common in our data. Median DBT was higher and MBG was poor but ST-resolution within 60 minutes was better in our study population.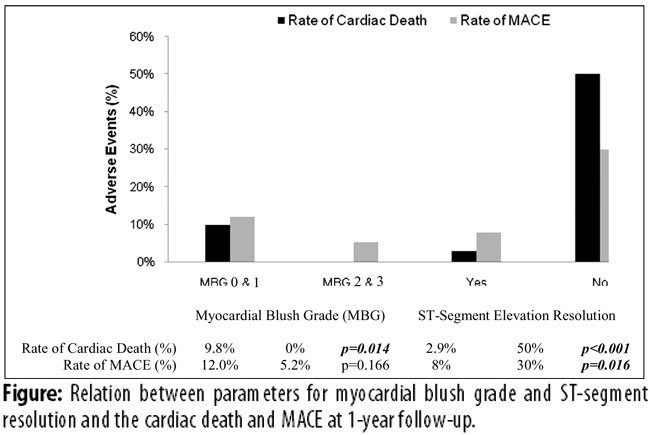
Figure-1 shows the relation of MBG and ST segment resolution and the cardiac death and MACE rate at one year follow up. Poor MBG (zero & 1) and no ST segment resolution significantly reflected poor outcome.
Discussion
The rationale behind manual thrombectomy during primary PCI is to prevent distal embolization that impairs microcirculation and may lead to no reflow.11,12 This is not uncommon in case of primary PCI where thrombus burden in infarct related artery is frequently seen. Poor myocardial reperfusion that is best evident angiographically by myocardial blush grade (MBG) is considered to be associated with adverse outcomes including reduced left ventricular function and survival.13-15 Numerous adjunctive coronary devices have been developed in an attempt to decrease or prevent embolization during revascularization and therefore to improve clinical outcomes. However, manual thrombus-aspirating catheters are user friendly, not usually associated with any specific or device related complications, and suitable for most coronary anatomies. In addition, they are considered beneficial in terms of improved late clinical outcomes as compare to non-manual thrombectomy.16
In this observational study we compared the patients who underwent Primary PCI with thrombus aspiration and without thrombus aspiration in a selective group. Like most of observational studies an inherent bias was present in the study design. However, to the best of our knowledge the issue of selective thrombus aspiration has not been addressed yet in any large studies especially from our part of the world. Interesting findings have emerged from this study. We found no significant difference among the selective groups in primary and secondary endpoints (Table-3). Our findings suggest safety of using aspiration thrombectomy only in patients with definite thrombus burden i.e. selective thrombus aspiration, which is different from the previous trials.6
Thrombus Aspiration during Percutaneous coronary intervention in acute myocardial infarction Study (TAPAS) is a landmark trial that changed the technique of Primary PCI. At 1-year TAPAS showed lower cardiac death (3.6% versus 6.7%; p<0.02) and cardiac death or non fatal reinfarction (5.6% versus 9.9%; p<0.009) with thrombus aspiration. However, it should be remembered that TAPAS was a study of routine thrombus aspiration versus no thrombus aspiration rather than a study of routine thrombus aspiration versus selective thrombus aspiration. The issue of selective thrombus aspiration strategy is still unresolved. Our findings support the strategy of selective thrombus aspiration and showed almost equivalent efficacy and safety as well as long term outcome in our population.
Although the study designs are different but in the absence of any other randomized study in our part of the world the results of current study can be compared with TAPAS just to initiate a discussion in this respect. Comparison of routine thrombus aspiration (TAPAS study) with selective thrombus aspiration (NICVD data) is shown in Table-4. Overall risk profile in selective thrombus aspiration group was worse as having significantly more diabetic and hypertensive patients, more frequent history of previous infarction, more frequently involved LAD as a culprit artery, and 93.3% visible thrombus as compared to 48.6% in TAPAS study group (p<0.001).
Poor myocardial blush grade (zero & 1) in our study group (61.3%) as compared to TAPAS study group (17.1%) is alarming. One can argue that this increased frequency of poor myocardial blush grade in our study is due to underuse of aspiration thrombectomy. But this argument does not get enough strength by our observation that despite of active thrombus aspiration in 117 patients (Table-3) we were able to achieve MBG II & III in 49 (41.9%) patients. This low rate of favourable MBG is understandable in view of poor risk profile especially high prevalence of diabetes (24.7% vs 10.6%; p<0.001) and high thrombus burden (93.3 vs 48.6%; p<0.001) in our study group. Secondly, deterioration of myocardial perfusion is a complex condition not affected by aspiration thrombectomy alone. Other factors like endothelial dysfunction, microvasculature obstruction, and reperfusion injury are also related to perfusion abnormality.18,19 These factors are more expected to present in our study population because of above mentioned poor risk profile.
However, one year mortality and MACE rate were not significantly different between the two groups although 30 day mortality was higher in our study population. The probable explanation of this short term high mortality was the greater number of patients with larger infarcts and poor background clinical history. But at the same time despite of poor risk profile our patient population was more than a decade younger (Table-4) as compared to TAPAS patient population and this may have an equalization effect of other poor risk factors and resulting in non-significant long-term clinical outcome. Same applies to better TIMI flow results despite of longer door to balloon time.
Interestingly poor MBG in higher number of patients in our patient population did not translate into poor long term outcome. In previous investigations it was reported that although removal of thrombus from the infarct related artery reduced no-reflow and was associated with improved TIMI flow and MBG but with an inconsistent effect on clinical outcome.16,20,21 Recently there are few other studies that raise the concerns of mortality benefit of aspiration thrombectomy.22,23 In contrast, we found complete ST resolution within 60 minutes of procedure in ~75% of our patients. This is consistent with TAPAS and various other studies and it is found to be a better and consistent predictor of outcome after primary PCI.24-26
There are few other findings in our study that need to be discussed. Ninety per cent patients of our study group were male. This could be due to gender bias that is present in our male dominant society where female gender, in general, is a less privileged part of the society. This is consistent with other studies on acute MI, in general, and reflects the gender discrimination commonly seen in the Indo-Pakistan subcontinent.27,28 Secondly, we enrolled only those patients who preferred and opted primary PCI as a mode of reperfusion. As we are lacking state funding for such procedures therefore patient has to bear most of the cost of the procedure (if not all). Consequently, most of the patients (~90%) opted pharmacological reperfusion (streptokinase) therapy. This may introduce a bias but it was inevitable in our resource limited setup.
In ~50% of our patients we could not retrieve the visible thrombus despite of the use of aspiration catheter (Table-2). This may be due to the fact that we used Platelet glycoprotein IIb IIIa inhibitor in all patients irrespective of clot burden. Secondly, we documented the retrieval of thrombus only by naked eye examination and we did not include the histopathological findings in our data. This was irrelevant to our aim and beyond the scope of the current object. Similarly, we did not use Adenosine in any patients of "No thrombus aspiration" arm. This was just because they did not show any post PCI complications like slow flow or no-reflow. This evident that they were low risk and low thrombus burden patients and did not warrant intracoronary injections of adenosine.
What would be the implications of our findings? Cost of primary PCI in our set up is $1265 and export catheter costs $275. If we deduct the cost of export catheter we can reduce the cost up to $990. This includes the balloon for predilation that costs just $88. In our study group predilation was done in 44% patients and predilation along with export catheter was used in 30.6% patients. Therefore according to our observation use of aspiration catheter does not necessarily preclude the need of predilation and hence does not affect the cost. Income per capita in Pakistan is $1368 in 2012-13 according to recent economic survey29 and saving $275 is a significant amount of money in such a poor country without adding any risk to the procedure. Moreover, it is evident by our findings that risk profile of our patient population is entirely different from the western population therefore contemplation of the safety and efficacy of a device is not necessarily the same. So, until the efficacy of routine manual thrombectomy is fully established our data supports the strategy of selective manual thrombus aspiration. This is a feasible strategy in our resource limited setup and reduces the unnecessary burden of cost.
Study Limitations
This was a single centered and non-randomized study that reflects the local experience of selective thrombus aspiration and thus the results may not necessarily be generalized. Secondly, this study was underpowered to identify exactly the difference in MACE after MI, especially in patients without aspiration thrombectomy. Moreover, we only evaluated our data on the basis of clinical follow up. We assessed the long term effect of thrombus aspiration and MBG on Left Ventricular (LV) function with clinical follow up and did not go for echocardiogram. Therefore we do not know the correlation of MBG on ejection fraction.
Conclusion
Our study supports the strategy of selective thrombus aspiration in definite thrombus laden infarct related artery and no thrombus aspiration in low risk group of patients with acute STEMI. Moreover, our data shows the diversity of risk profile between our population and the western population and adds to the data regarding the controversy about the clinical outcome of routine thrombus aspiration. This needs larger randomized trial data in our native population to conclusively resolve this issue.
Acknowledgement
Authors wish to thank Mr. Jaffer bin Baqar for his great help in managing and analyzing data.
References
1. Keeley EC, Boura JA, Grines CL. Priamry angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomized trials. Lancet 2003; 361: 13-20.
2. Silber S, Albertsson P, Aviles FF, Camici PG, Colombo A, Hamm C, et al. Guidelines for percutaneous coronary interventions: the Task Force for Percutaneous Coronary Interventions of the European Society of Cardiology. Eur Heart J 2005; 26: 804-47.
3. Ashraf T, Rasool SI, Saghir T, Rizvi SNH, Qamar N, Zaman KS, et al. Aspiration of Thrombus in ST elevation myocardial infarction. J Pak Med Assoc 2007; 57: 359-62.
4. Kushner F G, Hand M, Smith S C, King SB, Anderson JL, Antman EM, et al. 2009 Focused updates: ACC/AHA Guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 Guideline and 2007 focused update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (updating the 2005 Gudideline and 2007 focused update). Cath Cardiovasc Interv 2009; E1-44.
5. Svilaas T, Vlaar PJ, van der Horst I, Diercks GF, de smet BJ, Van de Heuvel AF, et al. Thrombus aspiration during primary percutaneous coronary intervention. N Engl J Med 2008; 358: 557-67.
6. Vlaar PJ, Svilaas T, van der Horst I, Diercks GF, Fokemma ML, de Smet BJ, et al. Cardiac death and reinfarction after 1 year in the Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS): a 1-year follow-up study. Lancet 2008; 371: 1915-20.
7. Sianos G, Papafaklis MI, Serruys PW. Angiographic thrombus burden classification in patients with ST segment elevation myocardial infarction treated with Percutaneous coronary intervention. J Invasive Cardiol 2010; 22: 6B-14B.
8. The TIMI study group. The Thrombolysis in Myocardial Infarction (TIMI) Trial Phase I findings. N Eng J Med 1985; 312: 932-6.
9. Van\'t Hof AW, Liem A, Suryapranata H, Hoorntje JC, de Boer MJ. Zajistra F. Angiographic assessment of myocardial reperfusion in patients treated primary angioplasty for acute myocardial infarctiopn. Myocardial blush grade. Zwolle myocardial infarction study group. Circulation 1998; 97: 2302-6.
10. Van\'t Hof AW, Liem A, de Boer MJ, Zijlstra F. Clinical value of 12-lead electrocardiogram after successful reperfusion therapy for acute myocardial infarcton. Lancet 1997; 350: 615-9.
11. Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary interventionpredicts outcome in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation 2005; 112: 906-15.
12. Henriques JP, Zijlstra F, Ottervanger JP, de Boer MJ, Van Hof AW, Hooranjee JC, et al. Incidence and clinical significance of distal embolization during primary angioplasty for acute myocardial infarction. Eur Heart J 2002; 23: 1112-7.
13. Poli A, Fetiveau R, Vandoni P, del Rosso G, D\'Urbano M, Seveso G, et al. Integrated analysis of myocardial blush and ST-segment elevation recovery after successful primary angioplasty: real time grading of microvascular reperfusion and prediction of early and late recovery of left ventricular function. Circulation 2002; 106: 313-8.
14. Ito H, Maruyama A, Iwakura K, Takiuchi S, Masuyama T, Hori M, et al. Clinical implications of the \'no-reflow\' phenomenon. A predictor of complications and left ventricular remodeling in reperfused anterior wall myocardial infarction. Circulation 1996; 93: 223-8.
15. Stone GW, Peterson MA, Lansky AJ, Dangas G, Mehran R, Leon MB. Impact of normalized myocardial perfusion after successful angioplasty in acute myocardial infarction. J Am Coll Cardiol 2002; 39: 591-7.
16. Burzotta F, De Vita M, Gu YL, Isshiki T, Lefevre T, Kaltoft A, et al. Clinical impact of thrombectomy in acute ST-elevation myocardial infarction: an individual patient-data pooled analysis of 11 trials. Eur Heart J 2009; 30: 2193-203.
17. Svilaas T, van der Horst IC, Zijlstra F. Thrombus aspiration during percutaneous coronary intervention in acute myocardial infarction study (TAPAS) study design. Am Heart J 2006; 151: 597.e1- 597.e7.
18. Fokkema ML, Vlaar PJ, Svilaas T, Vogelzang M, Amo D, Diercks GF, et al. Incidence and clinical consequences of distal embolization on the coronary angiogram after percutaneous coronary intervention for ST-elevation myocardial infarction. Eur Heart J 2009; 30: 908-15.
19. Bekkers SC, Yazdani SK, Virmani R, Waltenberger J. Microvascular obstruction: underlying pathophysiology and clinical diagnosis. J Am Coll Cardiol 2010; 55: 1649-60.
20. De Luca G, Dudek D, Sardella G, Marino P, Chevalier B, Zijlstra F. Adjunctive manual thrombectomy improves myocardial perfusion and mortality in patients undergoing primary percutaneous coronary intervention for ST-elevation myocardial infarction: a meta-analysis of randomized trials. Eur Heart J 2008; 29: 3002-10.
21. Mongeon FP, Belisle P, Joseph L, Eisenberg MJ, Rinfret S. Adjunctive thrombectomy for acute myocardial infarction: a Bayesian metaanalysis. Circ Cardiovasc Interv 2010; 3: 6-16.
22. Vink MA, Kramer MC, Li X, Damman P, Rittersma SZ, Koch KT, et al. Clinical and angiographic predictors and prognostic value of failed thrombus aspiration in primary percutaneous coronary intervention. J Am Coll Cardiol Intv 2011; 4: 634-42.
23. Bertrand OF, Larose E, Costerousse O, Mongrain R, Rodes-Cabau J, Dery JP et al. Effects of aspiration thrombectomy on necrosis size and ejection fraction after transradial percutaneous coronary intervention in acute ST elevation myocardial infarction. Cath Cardiol Interv 2011; 77: 475-82.
24. De Luca G, vant Hof AW, de Boer MJ, Ottervanger JP, Hoorntje JC, Gosselink AT, et al. Time to treatment significantly affects the extent of ST segment resolution and myocardial blush in patients with acute myocardial infarction treated by primary angioplasty. Eur Heart J 2004; 25: 1009-13.
25. Bhatia L, Clesham GJ, Turner DR. Clinical Implications of ST segment non resolution after thrombolysis for myocardial infarction. J R Soc Med 2004; 97: 560-70.
26. Farman MT, Sial JA, Khan NU, Rizvi SNH, Saghir T, Zaman KS. Outcome of primary percutaneous coronary intervention at public sector tertiary care hospital in Pakistan, 2011; 61: 575-81.
27. Jafary MH, Samad A, Ishaq M. Profile of acute myocardial infarction in Pakistan. Pak J Med Sci 2007; 23: 485-9.
28. Khan MS, Jafary FH, Faruqui AM, Rasool SI, Hatcher J, Chatervedi N et al. High prevalence of lack of knowledge of symptoms of acute myocardial infarction in Pakistan and its contribution to delayed presentation to the hospital. BMC Public Health 2007; 7: 284.
29. Pakistan Economic Survey 2012-13 Page V. Government of Pakistan, Finance Division, Economic Adiser’s Wing, Islamabad.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: