
Altaf Hussain Rathore ( Department of Surgery, Punjab Medical College, Faislabad. )
Yousaf Farooq ( Tehsil Headquarters Hospital, Shakkar Gardh. )
May 1981, Volume 31, Issue 5
Case Reports
Abstract
We present two unusual cases of conjoined xiphopagus where separation was successfully performed. The first pair had a common heart and the second pair shared a common liver. The classification, embryology of conjoined twins and results of the surgery are discussed.
Introduction
The aetiology of the conjoined twin has intrigued surgeons for many years (Seammon, 1925) especially since the birth of the famous conjoined twins in Siam in 1811 named Chang and Eng. Since then more than 400 cases, live and still born have been reported (Mulcare et al, 1970).
Many different classifications have been suggested by Guttmacher (1967) and Hirst and Piersol (1891) but the one derived from the area of union is commonly accepted. These are thoracopagus, Xipho or Omphalopagus pyopagus, Ischiopagus and Craneopagus (Table).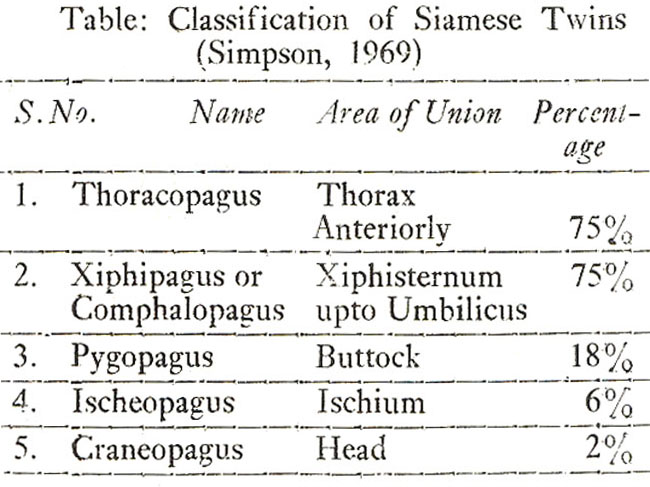
Conjoined twins are the product of a single ovum. They present an incomplete cleavage of the blastodermic vesicle which occurs in the third week of pregnancy (Zimmermann, 1967).
The group which are joined anteriorly share a common umbilicus. This can be disastrous for one of the twins. If one foetus is larger and has a stronger heart than the other it will monopolise the greater part of the placental circulation and it may actually cause regurgitation through the umbilical arteries of the weaker foetus. In such cases the latter may not develop completely. The two cases presented in this paper are of this type-one normal foetus attached in front to an incomplete one.
Case Reports
Case I:
On 26-3-1974 a twenty five year old woman delivered normally a full term live, male xiphopagus twin (Fig. 1) at home.
The mother already-had two daughters who had been born normally. There was no history of twins in the family. A normal baby was attached to a headless sibling. Their combined weight was 10 lbs. One foetus was completely normal and active apart from a systolic murmur in the. mitral area and a small omphalocele. The headless foetus was acardiac with each of the four limbs only possessing three digits. The penis and scrotum were well developed although the testes and other organs were rudimentary. A plain X-ray was taken (Fig. 2).
Other investigations such as alimentary canal series, I.V.P., cholecystogram, isotope tagged albumin cross over studies, radioactive oxygen, to assay the anatomical connections were not done as described by Singleton (1967), Spencer et al (1967), Pedrosa de Lima and Teixeira (1967), Spratt et al (1961), Hill et al (1961) and Aird (1954). The.E.C.G. of the first baby was normal. The separation was performed on under local anaesthesia. The abnormal sibling was sacrificed. The patient had a stormy postoperative period but survived and was discharged from the hospital on 7-6-1978. He is still alive and well at the time of reporting.
Case 2:
On 9-9-1975 a thirty year old woman delivered normally a full term, live male xiphopagus twin at home. She was the mother of 4 children who had all been born normally. There was no history of twins in the family. A normal foetus was joined anteriorly to a monster (Fig. 3).
One foetus was active, feeding well, passing stool and urine and showed no abnormality whatsoever. The second foetus was abnormal with a head, deformed nose, bilateral cleft lips, normal neck, only one left normal upper limb, one nipple and a very small chest in which was a normal heart. All the abdominal visceras were enclosed in a thin transparent membranous bag attached to the abdominal wall of the normal foetus like a baloon in the area between the xiphoid sternum and the umbilicus. The abnormal foetus was breathing and moving his only limb and there was excessive saliva trickling out of the mouth. Both shared a common liver. No investigations were done.
Separation took place in two stages under local anaesthesia. The first operation was performed six hours after birth in which the monster was sacrificed and separated except for the liver (Fig. 4).
This was separated one week later in the second operation. The normal baby was discharged from hospital 14 days after the second operation. Unfortunately the baby died at home after 2 months due to a chest infection.
Discussion
Conjoined twinning is one of the rarest of congenital anomalies with an overall incidence ranging from 1 in 50,000 to 1 in 80,000 births. The treatment is surgery because no one can afford to be Chang and Eng in these days. Thirty-one attempted operations have been reported in medical literature so far (Mulcare et al., 1970). There may have been more which have not been reported. Most of them shared a common liver but few of them had a common heart. Unlike our first case none of the twins with a single heart, including Bland\'s twin, actually survived (Bland and Hammer, 1962; Jenkins et al., 1958; Johnson and Doherty, 1957; Retiman et al., 1953). Thus the first case holds a place of special importance in medical literature as being the only record of survival of the subject after surgery who had shared a single heart with the other foetus.
The most difficult part of the operation in the separation of a conjoined twin is the closure of the skin defect and division of the common liver if the twin happens to share one as occurred in our second case. In dealing with our second case in which the twin shared a common liver, owing to the poor chance of survival, the possibility of a two staged operation was explored and finally successfully performed. This brings us to the conclusion that more separations could be successfully performed in two stages.
Acknowledgement
The authors wish to acknowledge the help of Miss Elizabeth Ann Yates in the preparation of this manuscript.
References
1. Aird, I. (1954) The conjoined twins of Kano. Br. Med. J., 1:831.
2. Bland, K.G. and Hammer, B. (1962) Xiphopagus twins. Report of obstetric and surgical management of a case. Cent. Afr. J. Med., 8:371.
3. Guttmacher, A.F. (1967) Biographical notes on some famous conjoined twins. National Foundation, Birth Defects, Original Articles Series, 3:10.
4. Hill, A.J. Jr., Peterson, C.G., Grondahl, R.D. and Krip-pachne, W.W. (1961) Conjoined thoracopagus twins; pre-and postoperative considerations. J. Pediatr., 58:59.
5. Hirst, B.C. and Piersol, G.A.; Human Monstrosities, vol. I. Philadelphia, Lea Brothers 1891, p. 17.
6. Jenkins, E.W., Watson, T.R. and Mosenthal, W.T. (1958) Surgery in conjoined twins. Arch. Surg., 76:35.
7. Johnson, N.J. and Doherty, J.E. (1957) Simultaneous electrocardiograms in thoracopagus twins. Am. Heart 53:150
8. Mulcare, R.J., Bhokakul, P., Potitung, P. and Wheeler, B. (1970) The surgical separation of the thoracopagus conjoined twins of korat, Thailand. Ann. Surg., 172:91.
9. Pedrosa de Lima, J.J. and Teixeira, S.N. (1967) Liver scan in a case of conjoined twins. Nuclearmedizin, 6:363.
10. Reitman, H., Smith, E.E. and Geller, J.S. (1953) Separation and survival of Xiphopagus twins. JAMA., 153:1360.
11. Scammon, R.E. Fetal Malformations, in pediatrics. Edited by I.A. Abt. Philadelphia, Saunders, 1925, p. 654.
12. Simpson, J.S. (1969) Separation of conjoined thoracopagus twins with the report of an additional case. Can. J. Surg., 12:89.
13. Singleton, E.B. (1967) Radiologic studies of thoracopagus twins. The National Foundation-Birth Defects Orig. Art. Series, 3:89.
14. Spencer, R.P., Rockoff, M.L., Nichols, B.L. and Johnson, P.C. (1967) Radioisotope flow studies in conjoined twins. The National Foundation Birth Defects Orig. Art. Series, 3:120.
15. Spratt, J.S. Jr., Ter-Pogossian,M., Rudman, S. and Spencer, A. (1961) The measurement of the pulmonary venous cross-circulation through the conjugated heart of thoracopagus twins with radioactive O15. Surgery, 50:941.
16. Zimmermann, A.A. Embryologic and anatomic consideration of conjoined twins, National Foundation, Birth Defects., Original Article Series, 3:18 April 1967.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: