
Zulfiqar Haider ( PMRC Research Center, Fatima Jinnah Medical College, Lahore. )
Surraiya Obaidullah ( PMRC Research Center, Fatima Jinnah Medical College, Lahore. )
Fayyaz ud Din ( PMRC Research Center, Fatima Jinnah Medical College, Lahore. )
Manzar Saleem ( Services Hospital, Lahore. )
January 1981, Volume 31, Issue 1
Original Article
Abstract
Fifty seven newly diagnosed obese maturity onset diabetics were studied for 3 years to monitor the effect of diabetic control on weight and blood lipids. Of the 41 patients who had a satisfactory control of diabetes, weight loss of a modest degrec was recorded in only 6. The blood lipids did not show any significant changes in both the controlled and uncontrolled groups. It is suggested that blood sugar control can be achieved in a majority of obese diabetics without weight loss. However, the correction of abnormal lipid pattern probably neeth weight reduction to the near ideal weight (JPMA 31:8, 1981).
Introduction
The relationship between diabetes and obesity is well known and a significant number of patients presenting with clinical diabetes are over weight. Both diabetes and obesity are associated with lipid abnormality. In general weight reduction has been thought to be an important step to achieve good control in obese diabetics. However, it has been observed that a large number of obese diabetics achieve a reasonable control of blood glucose on carbohydrate restriction without appreciable change in weight. There are not many studies in which the long term effect of metabolic control with and without weight loss have been assessed. The influence of weight changes and metabolic control on lipid behaviour in obese diabetics also needs more evaluation.
tn this study 57 newly diagnosed obese diabetics were followed up to assess the relationship of blood glucose control with changes in weight and blood lipids.
Material and Methods
Initially 103 newly diagnosed obese maturity onset diabetics were included. Obesity was defined as ‘weight excess’ of more than 10% above the standard weight. The present study deals with 57 patients, who completed a follow up of 3 years or more.
After an initial assessment the patients were given a reducing diet containing 100 to 150 gms of carbohydrate. The short term assessment of control was done at 6 weeks after starting thc dietary therapy. Those who were not controlled by the dietary therapy alone were given oral anti-diabetics according to the clinical situation.
All patients were followed up for a period of at least 3 years when final assessment of their state of control, weight and blood lipids was made. The lipid study which included serum cholesterol and triglyceride was done in the fasting state at the time of diagnosis and at final assessment.
The control of each patient was assessed from the mean of the last 3 readings of random blood sugar. Those with a value of less than 200 mg were considered in the catcgory of satisfactory control. Serum cholesterol was measured by the method of Abell (Abell et al., 1952) and triglycerides by Van Handel and Zilversmit method (1957).
Results
Of the 57 patients studied 41 had a satisfactory blood sugar control.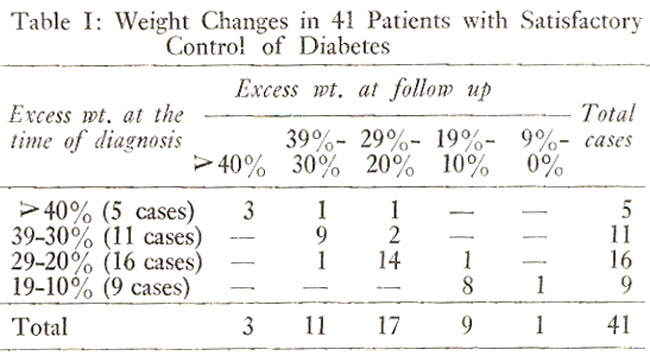
Table I shows weight changes in 41 patients with a satisfactory control of blood sugar levels. There were 5 patients with a weight excess of 40% or more of which only 2 patients reduced to the lower range of weight excess. There were 11 patients with a weight excess between 30-39% and only 2 showed a reduction in weight excess. Of the 16 patients who had a sveight excess between 20-29%, one patient gained weight and one lost weight. Thus in only 6 out of 41 patients a loss of excess weight occurred. None of the patients achieved a weight reduction to ‘ideal weight’ after 3 years.
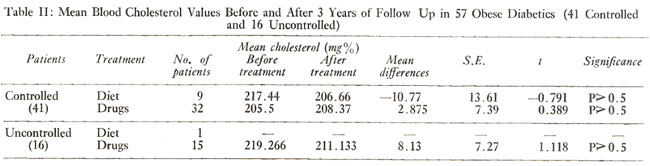
Table II shows the mean cholesterol values in 57 patients bethre and after 3 years. There was no significant change in the mean terol values in those with a satisfactory or poor control either on diet or drugs.
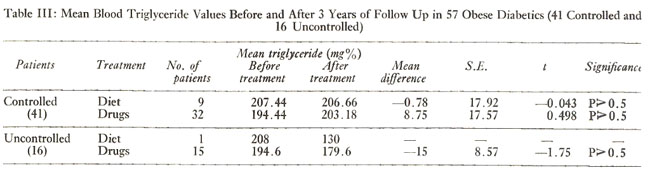
Table III shows the mean triglyceride values in 41 controlled and 16 uncontrolled diabetics before the onset of" therapy and at the time of follow up. There were no significant changes in triglyceride values in various groups irrespective of the mode of therapy.
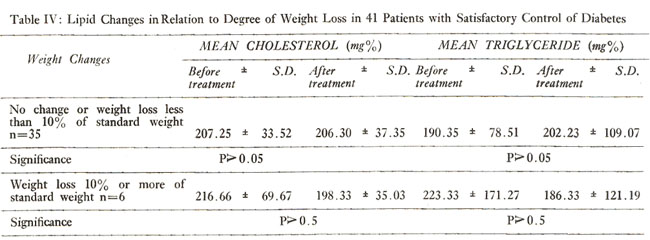
Table IV shows the relationship of lipid changes to the degree of weight loss in 41 patients who were apparently controlled.
In 35 patients who did not lose weight the cholesterol and triglyceride values were 207.25 mg% and 190.357 mg% respectively at the time of diagnosis. After 3 years the cholesterol and triglyceride values were 190.35 mg% and 202.23 mg% respectively. The changes were insignificant.
In the 6 patients who lost 10% or more of \'weight excess\' the cholesterol and triglyceride values at the time of diagnosis were 216.66 mg% and 223.07 mg% respectively.
At the time of reassessment the values were 223.33 mg%±171.27 and 186.33 mg%± 121.19 respectively. Serum triglyceride values showed an insignificant decline in the group of patients who lost weight.
Discussion
Obesity is widespread amongst diabetics particularly in the females. It is associated with reduced number of insulin receptors (Olefsky, 1976). In obese diabetics there is a high insulin secretory rate due to peripheral insulin resistance, which ultimately leads to attenuation of the insulin response and hyperglycaemia. Weight reduction is an ideal treatment for obese diabetics, but it is difficult to achieve in practice.
In 53 obese diabetic patients, who were followed for a period of 3 years, 41 achieved a reasonable degree of blood sugar control but only a modest reduction in weight by carbohydrate restriction. Wall and his colleagues(1973) observed that in 80% of their obese diabetics blood glucose control was achieved on simple carbohydrate restriction without an appreciable weight loss.
The concept of \'control\' in the management of diabetes is undergoing a change. Diabetes mellitus is an important risk factor for ischaemic heart disease and a more comprehensive approach towards its control is desirable. Both diabetes and obesity lead to alterations in lipid metabolism. The association between hypertriglyceridaemia and obesity is generally known (Albrink and Meigs, 1965).
Olefsky et al (1974) found that insulin over production in obese diabetics may lead to increased synthesis of very low density lipoprotein (VLDL). An increase turn over of fatty acids has also been associated with obesity (Nestel and Whyte, 1968) and may be partly responsible for increased VLDL secretion in patients with diabetes. There is a considerable evidence that hypertriglyceridaemia leads to the development of atherosclerosis in diabetics (Santen et al., 1972). The incidence of hypercholesterolemia in diabetic patients is controversial but some workers have shown a high cholesterol level in diabetics with metabolic decompensation (Bennion and Grundy, 1977).
The blood triglyceride and cholesterol levels in obese patients in this study did not show any significant changes even in those who achieved a reasonable control of blood glucose. This may be due to the fact that the weight reduction in our patients was not sufficient and no patient achieved the target of "ideal weight". Wilson et al (1980) in a study of dietary management of maturity onset diabetes showed that the blood triglyceride values follow the pattern of body weight more closely than the blood glucose as has also been found in this study.
Diabetic control should include reduction to as near to the "ideal weight" as possible and correction of lipid abnormalities along with that of hyperglycaemia.
References
1. Abell, L.L., Levy, B.B., Brodie, B.B. and Kandall, F.E. (1952) Simplified method for the estimation of total cholesterol in serum and demonstration of its specificity. J. Biol. Chem., 195:357.
2. Albrink, M.J. and Meigs, J.W. (1965) The relationship between serum triglycerides and skinfold thickness in obese subjects. Ann. N.Y. Acad. Sci., 131:673.
3. Bennion, L.J. and Grundy, S.M. (1977) Effects of diabetes mellitus on cholesterol metabolism in man. N. Engl. J. Med., 296:1365.
4. Nestel, P.J. and Whyte, H.M. (1968) Plasma free fatty acid and triglyceride turnover in obesity. Metabolism, 17:1122.
5. Olefsky, J., Reaven, G.M. and Farquhar, J.W. (1974) Effects of weight reduction on obesity. Studies of lipid and carbohydrate metabolism in normal and hyperlipoproteinemia subjects. J. Clin. Invest., 53:64.
6. Olefsky, J.M. (1976) Decreased insulin binding to adipocytes and circulating monocytes from obese subjects. J. Clin. Invest., 57:1165.
7. Santen, R.J., Willis, P.W. and Fajans, S.S. (1972) Atherosclerosis in diabetes mellitus. Correlations with serum lipid levels, adiposity, and serum insulin level. Arch. Intern. Med., 130:833.
8. Van Handel, E. and Zilversmit, D.E. (1957) Micromethod for direct determination of serum triglycerides. J. Lab. Clin. Med., 50:152.
9. Wall, J.R., Pyke, D.A. and Oakley, W.G. (1973) Effect of carbohydrate restriction in obesediabetics; relationship of control to weight loss. Br. Med. J., 1:577.
10. Wilson, E., Hadden, D.R., Merrett, J.D., Montgomery, D.A.D. and Weaver, J.A. (1980) Dietary management of maturity onset diabetes. Br. Med. J., 280:1367.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: