
Ikram Ullah Khan ( ENT Specialist, Central Government Polyclinic, Islamabad. )
May 1982, Volume 32, Issue 5
Case Reports
Abstract
A case of Tubercular granuloma of the epiglottis is presented. The presenting symptoms were hoarseness and dysphagia, and the laryngoscopic appearance resembled carcinoma. Histological examination of biopsy material was diagnostic, emphasising the difficulty of diagnosis in the general population (JPMA 32:128, 1982).
Case History
A 56 years old male, resident of Rawalpindi, businessman by profession, attended the E.N.T. Department Central Government Poly Clinic, Islamabad on 15-12-1980. His main symptoms were dysphagia, pain radiating to the right ear and a change in the character of his voice, having become rough and muffled. He looked pale and depressed and was concerned about having cancer of the throat. These symptoms were of 8-10 weeks duration and were getting increasingly worse. Five years back he was treated for pleural effusion and pulmonary tuberculosis for about a year, following which he was well. About ten weeks prior to consultation he had noticed a changing voice and gradually increasing dysphagia alongwith a dry cough. He had been smoking 40-60 cigarettes a day.
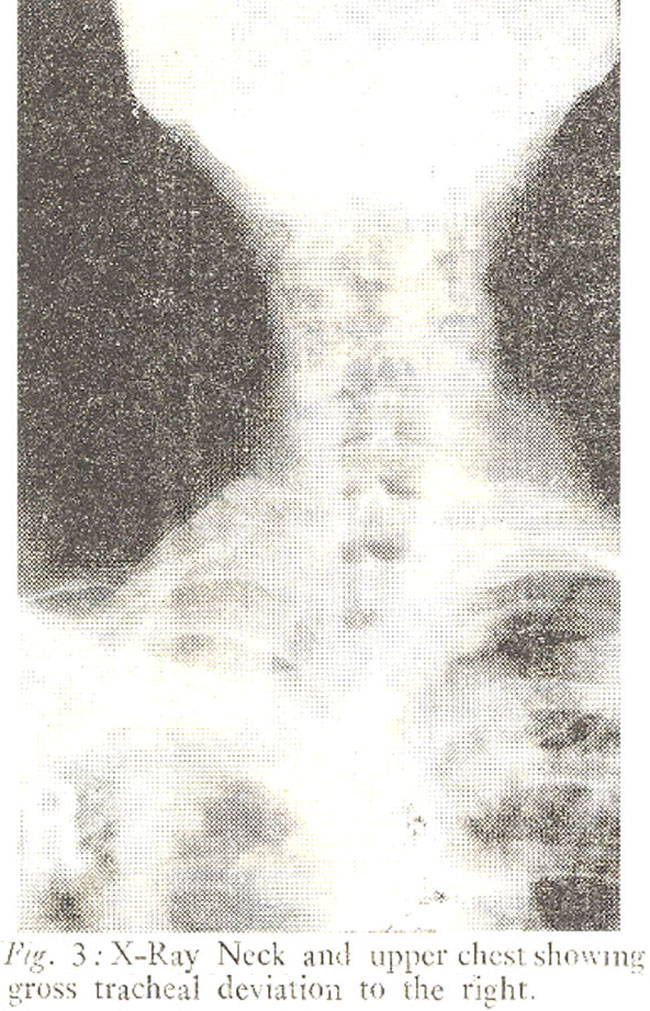
Clinical examination of the larynx showed a tumour arising from the epiglottis, occupying mainly the right half of the cartilage. The rest of the epiglottis was oedematous, the aryepig-lottic folds ventricular bands and vocal cords were hyperaemic, the right cord showing restricted movements on phonation. Two Right Upper deep cervical nodes were palpable and mobile. He was admitted for further examination and investigations. X-Ray neck lateral view-showed swelling of the epiglottis. X-Ray chest showed gross fibrotic changes on the right side, with obvious deviation of the trachea;. Blood examination revealed Hb 11.9G%, TLC 5,300 with a normal differential count and ESR 30mm 1 st hour. Sputum could not be tested and a direc laryngoscopy complied with the clinical diagnosis. The histological examination of the biopsy confirmed the diagnosis of Tuberculous Granuloma.
Treatment was given with Streptomycin, INH and Ethambutol in combination according to established principles. Response to therapy was prompt and positive. Considerable general and clinical improvement was seen within four weeks. The tumour disappeared completely and on examination two months later the epiglottis appeared normal except for a punched out appearance of the area where the tumour was originally observed. Both vocal cords were mobile about 8 weeks following treatment and the cervical nodes were not palpable. He remains symptom-free to the present date.
Discussion
The presentation of the case has resembled carcinoma with a short history of progressive hoarseness and dysphagia. Other authors have emphasised laryngeal tuberculosis mimicking carcinoma (Bull, 1966; Hunter, 1981). In their cases the lesions were noted mostly on the vocal cords and ventricular bands and were associated with moderate to advanced pulmonary tuberculosis. In the present case histological examination of biopsy material was necessary to confirm the diagnosis. X-Ray chest showed extensive fibrotic changes but no active pulmonary lesion. Sputum could not be obtained for examination. This exemplifies the difficulty in early diagnosis of laryngeal tuberculosis in the general population.
Although this is an isolated case presentation, several interesting features have been noted. In contrast to classic descriptions of laryngeal tuberculosis, when cases were seen suffering from marked constitutional symptoms accompanied by advanced pulmonary disease with productive cough, this patient presented himself with dysphagia due to the lesion, on the epiglottis fearing he had cancer of the throat.
Also the appearances of the laryngeal tuberculosis of the past emphasised multiple ulcerating lesions of the posterior half of the larynx and vocal cords. In contrast tumour formation was seen in the present case. Bull and Hunter report a similar change in the clinical presentation of their cases. Tumour formation could possibly be due to improved host resistance and perhaps previous chemotherapy. Altered virulance of the organisms may also play a similar role in the pathogenesis of this lesion.
In general, inspite of the prevalence of pulmonary and extra pulmonary tuberculosis in Pakistan, laryngeal lesions have not been frequently reported. Several factors could account for this. As the larynx is not a very accessible organ for examination by the G.P. and medical specialists, the lesion could be easily missed. Also perhaps there exists a general lack of awareness of the existence of laryngeal tuberculosis.
To overcome these difficulties, it is felt that a high index or suspicion has to be cultivated in order to isolate and promptly treat cases.
References
1. Bull, T.R. Tuberculosis of the Larynx. The Institute of Laryngology and Otology reports, 16:1965-66 page 245.
2. Hunter, A.M. et al (1981) The changing pattern of Laryngeal Tuberculosis. J. Laryngol. Otol., 95:393.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: