
Abdul Latif Qureshi ( Department of Urology, King Edward Medical College, Lahore. )
November 1985, Volume 35, Issue 11
Original Article
Abstract
Posterior surgical approach to the kidney and upper ureter was performed on 20 cases. The Lumbotomy incision gave excellent results in nephrectomy, open renal biopsy, pyelolithotomy, pyeloplasty and upper third ureterolithotomy. Review of operative technique, advantages and limitations of the approach are presented (JPMA 35 :334, 1985).
INTRODUCTION
The posterior approach to the kidney is not a new technique. It was described by Simon1 and subs9uently was popularised by Lurz2 and Gil.Vernet3 . This approach although being used quite frequently in Europe for a variety of upper urinary tract operations has not achieved an equal measure of popularity with our surgical colleagues in this country, where the extra-peritoneal lumbar incision is generally preferred. Nevertheless, the posterior lumbotomy incision does allow certain operations on the kidney, renal pelvis and upper ureter to be accomplished more rapidly with reasonably good exposure and diminished morbidity, particularly in selected patients. The incision is particularly well suited for bilateral nephrectomy in renal transplantation, open renal biopsy, simple nephrectomy, pyelolithotomy, pyeloplasty and upper third ureterolithotomy. The advantages and limitations of this approach to the urinary tract and the clinical results in patients under-going pyelolithotomy, nephrectomy and upper third ureterolithotomy throughsuch an incision are described herein.
MATERIAL AND METHODS
Twenty patients (13 females, 7 males) needing surgery on the upper urinary tract for a variety of renal disorders were operated upon from May, 1983 to April, 1984. The average age of the patients was 28 years, the youngest being 4 and the oldest being 63 years old. They were selected at random. Clinical history, laboratory tests especially renal functions, urocultures and excretory urography which was the mainstay in diagnosis were done in all the case. Only one female patient had undergone previous renal surgery through flank incision. The operations performed were pyelolithotomy, pyeloplasty, nephrectomy, nephrostomy, open renal biopsy and upper third ureterolithotomy.
The surgical technique used was similar to the one used by Gil-Vernet3 and Freed4. The patient was positioned on the operating table on the lateral side so that the affected side looked towards the operator. The bridge was raised and the patient was flexed laterally in order to widen the intercostal space. Then the table was tilted towards the opposite side with a veiw to bring the back towards the operator in a more or less flattened position (Fig I).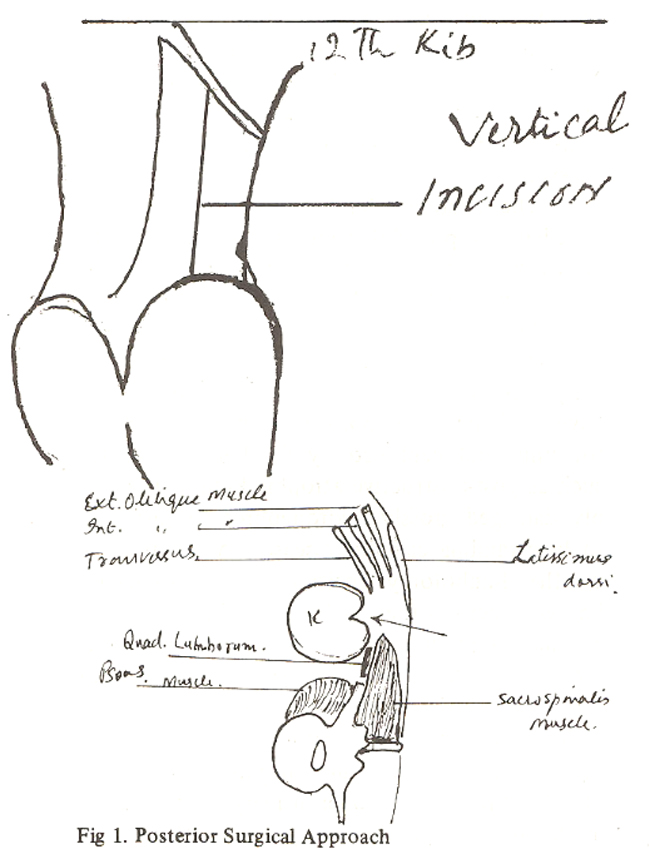
A vertical incision commencing at the 12th rib was made along the lateral edp of the sacrospinatis muscle upto the iliac crest3,4. The incision was deepened through fat, latissmus dorsi muscle in the upper part of the wound and continued down through lumbodorsal fascia just lateral to the sacrospinatis and quardatus lumborum muscles which were then retracted medially to enter the renal fossa. Then GEROTA’S fascia incised and the kidney was mobiised as usual. (12th subcostal and iliohypogastric nerves traverse the field obliquely and need to be carefully retracted). In case the exposure is inadequate and the access is restricted, 12th rib can be resected. To obtain a better posure superiorly the costovertebral ligamentous attachment of the rib can be severed and the incision opened widely with retractors. Resection of the rib was not required in our case. Care is taken to avoid injury to the pleura and the subcostal vessels. Since the renal pelvis and the ureter are situated dorsally, a good exposure is obtained with this incision for pyelolithotomy, pyeloplasty and upper third ureterolithotomy. The exposure provided by the lumbotomy incision is especially helpful when the dissection into the renal sinus is indicated to perform Gil-Vernet’s extended pyelolithotomy for intra-renal pelvis or branched calculi. The approach is also excellent for open renal biopsy. An abbreviated incision of 7-8 cms long is made in such cases directly on the lower pole of the kidney to obtain the biopsy.
RESULTS
From May, 1983 to April, 1984, 20 patients were operated upon through posterior vertical lumbotomy incision (Table 1).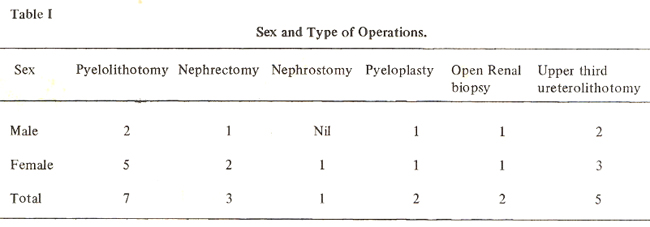
This route, although requiring more operative care, undoubtedly results in a much smoother post-operative course with minimum morbidity. Post operative recovery was excellent in all the cases with most of the patients fully ambulatory and on oral diet on 2nd 3rd day. The average hospital stay was 5 ~. days. There was no operative death. In two patients superficial wound infection occurred, otherwise recovery was uneventful in all the cases. This stands in vivid contrast to our experience with the flank incision. A young man of 24 was maa4~operated upon for bilateral upper ureteric calculisimultaneously on both sides. The approach to the right side was through vertical lumbotomy while the left calculus was removed through flank incision. The right lumbotomy wound healed nicely relatively painlessly on the 4th post. operative day but the left flank incision still looked angery with considerable pain and got infected taking 2 weeks to clear up. Thus the healing was distressingly delayed on the left side for 2 weeks.
There appears to be a significant decrease in the morbidity associated with lumbotomy incisions as compared to other incisions used for renal surgery. The approach is in particular advan. tageous for open renal biopsy with an abbreviated incision to establish an accurate tissue diagnosis. The operations were done under G.A. and both the patients were ready to get discharged from the hospital the next day after undergoing open renal biopsy. No surgical complication was noted in the patients. They had mild postoperative discomfort from the incision which was easily controlled with oral analgesics. None of the 20 patients developed post.operative incisional hernia. The incision was much appreciated by the female patients.
DISCUSSION
Present experience with the posterior vertical lumbotomy incision has convinced us of several distinct advantages that render it ideal for performing certain operations on the upper urinary tract. Unlike the standard flank incision no muscles are cut and the access to the kidney is obtained by simply incising the posterior fascial layers, The approach is more rapid, provides a strong wound closure with less postoperative pain, obviates antelateral bulging of the abdomen that commonly results from the flank incision. In addition to offering rapid exposure, the lumbodorsal approach considerably simplifies the closure
Detachment of the costovertebral ligament allows the 12th rib to be retracted widely laterally rendering the resection of the 12th rib unnecessary. The posterior approach has been found parti. cularly of great advantage in patients with prior abdominal or flank operation on the kidney,since it permits dissection of fresh untouched tissue planes. Since the lumbotomy incision provides the shortest and most direct approach to the dorsal aspect of the kidney, it is ideal for pyelolitho. tomy, and pyeloplasty. The kidney can be mobi. lised and delivered down into the incision for these operations provided the lower third of the kidney is located below the 12th rib on preoperative X.rays. However, for high lying kidneys the posterior approach is cumbersome and either a flank or anterior incision will provide a better exposure.
The posterior lumbotomy incision is also excellent and provides the most rapid approach for removing calculi impacted in the upper third of the ureter and for performing open renal biopsy.
Freed4 has reported excellent results with this approach in a large number of transplant recipients undergoing bilateral nephrectomy. We have used the same approach with good exposure for unilateral nephrectomy for benign disorders such as post-obstructive atrophic kidney, irreversibly damaged grossly hydronephrotic kidney due to longstanding calculus disease. A disadvantage of the lumbotomy incision is the somewhat limited access to the renal vessels. For this reason alternate approaches are preferable for operations such as iIèphrolithotomy, partial nephrectomy that may require temporary control or repair of major vessels of kidney. Neverthe less, the advantages of the posterior surgical approach in terms of exposure to the upper urinary tract and the minimum patient morbidity are sufficient to warrant its increased use when the prerequisite conditions described herein are met.
ACKNOWLEDGEMENT
The author would like to express his gratitude to Dr. Aftab Ahrned Jehangir for his taking pains in typing the article.
REFERENCES
1. Simon, G. Exterpation Einer and Menscher. Disch.Klin., 1871;22: 137.
2. Lurz, H. Ein maskelschonender Jumbalschnitt zur Freilegung der Niere. Chirrg, 1956; 27: 125.
3. Gil-Vernet, New surgical concepts in removing renal calculi. Urol. Int., 1965; 20 : 255.
4. Freed, S.Z. The present status of bilateral nephrectomy in transpient recipients. J. Urol., 115:8.
5. Novick, A. C., Braun, W.E., Magnusson, M. and Stowe, (1979) Current status of renal transplan tation at the Cleveland clinic. J. Urol., 1979; 122: 433.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: