
Mohammad Zaman ( Department of Pulmonary Medicine, Pakistan Institute of Medical Sciences, Islamabad. )
November 1987, Volume 37, Issue 11
Case Reports
Asthmatic pulmonary eosinophilia is due to hypersensitivity to Aspergilus fumigatus or Candida albicans. It is a combination of types 1 and 3 hypersensitivity reactions, occurs predominantly in atopic people1 and is characterized by episodic wheeze, migratory pulmonary infiltrations and eosinophilia of blood and sputum. Bronchial casts containing A. fumigatus or C. albicans may be expectorated2, precipitins to the fungi commonly present in the blood and skin tests with respective antigen cause both immediate and late reactions. Bronchial challenge with these antigens may produce positive immediate and late bronchial (asthmatic) reactions and may precipitate severe asthma, and is not done routinely. Pollens, dust, animal products, various thugs have been blamed in some cases3. Nickel vapours have given rise to this syndrome4 and it has also been recorded in established cases of Filariasis and Schistosomiasis. Sometimes no potential allergen can be identified.
CASE REPORT
R.B., an unmarried 20 year old girl, with history of recurrent paroxysmal attacks of dysponoea for 15 years, reported to Pulmonary Medicine Department (Islamabad Hospital Complex), Pakistan Institute of Medical Sciences Islamabad, complaining of cough and expectoration of dark yellow inspissated sputum with fever and chest pain of 2 months and haemoptysis of 1 month duration, but with severe incapacitating breathlessness and louder wheeze of 12 hours duration. Temperature was 101°F, pulse 105 and respiration rate was 42 per minute. Pallor was present with both peripheral and central cyanosis. Percussion note was equally resonant on each side. On auscultation, She had bronchial breathing in upper 1/2 (anteriorly and posteriorly) with vesicular breath sounds in lower 1/2 of the chest and high pitched (inspiratory as well as expiratory) rhonchi and scattered course crepitations all over the chest without pleural rub. Nothing abnormal was detected in any of the remaining systems.
Chest radiograph PA view of November 17, 1986 (Figure 1)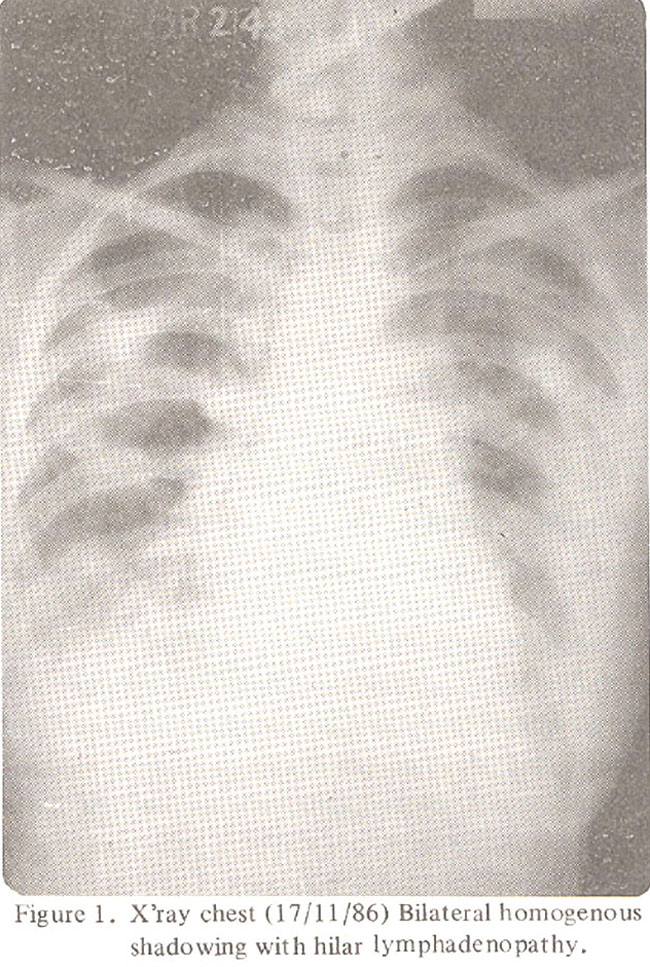
reveals bilateral homogenous shadowing all over the lung fields with bilateral hilar lymphacienopathy. These shadows migrated and occupied the central areas of mid and upper zones as compared to their locations in the periphery in the X-ray chest PA view of November 12, 1986 (Figure 2).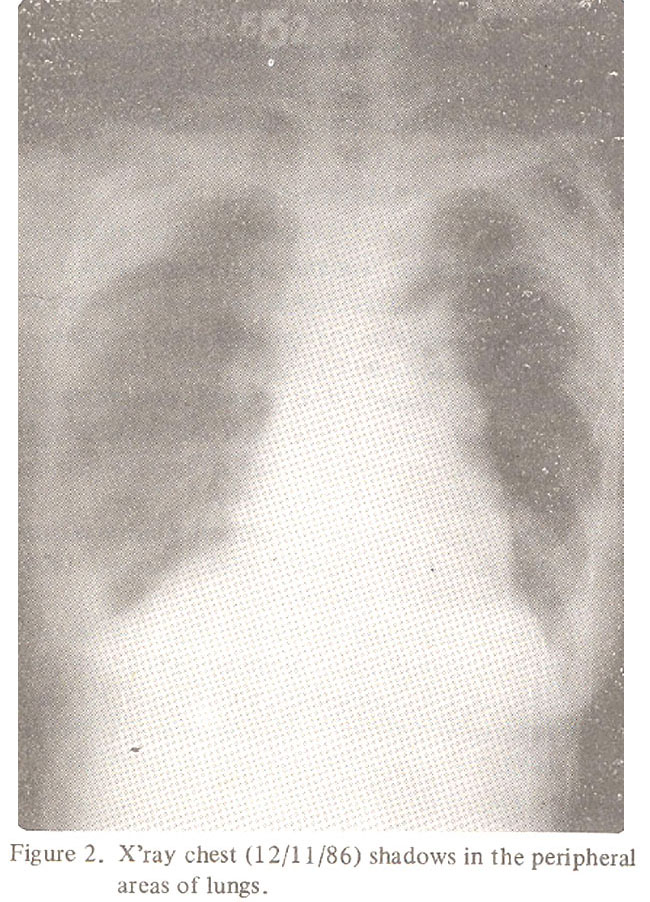
Blood picture prior to treatment’ was Hb 12.5 gm/dl, TLC 4 330/mm3, Neutrophils 13%, Lymphonytes 23%, Monocytes 0, Eosinophils 64%, Total Eosinophils 277 1/mm3, ESR 77 mm/lst hour.
Three specimens of sputum for culture and sensitivity for bacteria, fungi and direct microscopy for AFB were negative. ECG showed right axis deviation, generalized flattening of T wave and occasional supraventricular ectopics (patient was already on salbutamol 4 mg t.d.s.). Mantoux with 5 TU was negative. Blood collected at midnight for microfilariae showed negative results. Bone marrow revealed marked hyperplasia of eosinophilic series of cells, consistent with blood eosinophilia with no other significant finding.
Treatment started with Ketoconazote 200 mg daily (a broadspectrum systemic-antimycotic agent active against pathogenic fungi), prednisolone 40 mg daily in divided doses for 3 days and tapered gradually and stopped completely in 10 days. Salbutamol was substituted with Turbutaline SO2. Patient became asymptomatic after 72 hours. Occasional rhonchi could be heard. Temperature was settled. No side effects of Ketoconazole.except itching developed.
X-ray chest PA view (29 Nov. 86) showed clear lung fields and normal hilar shadows (Figure 3).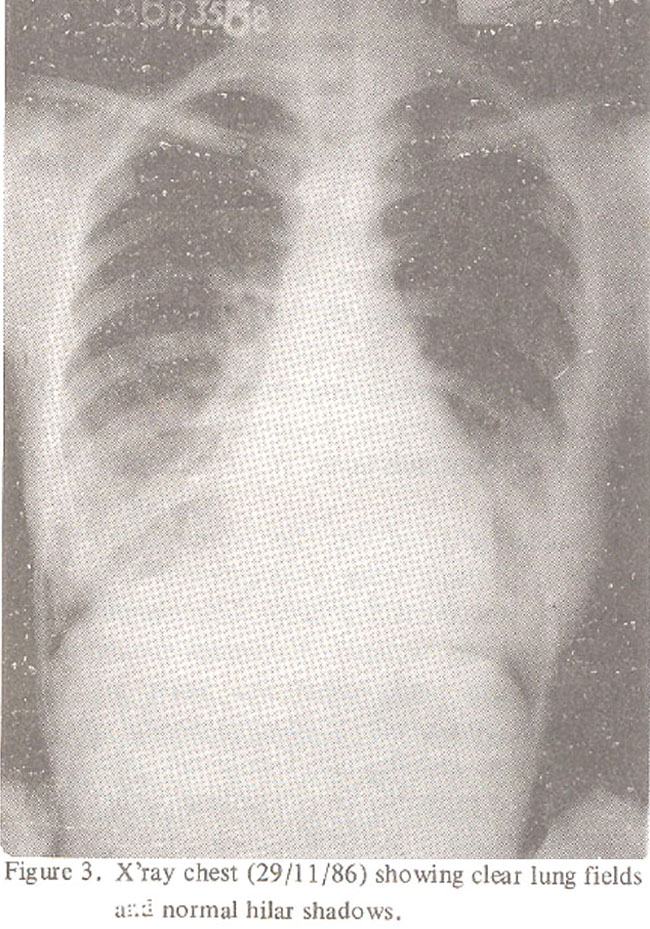
After treatment, complete blood picture showed Hb 12.5 gm/dl, TLC 8600/mm3, Neutrophils 60%, Lymphocytes 31%, Eosinophils 01, ESR 4 mm. ECG became normal. Ketoconazole was continued until one week after symptoms cleared. (Total duration of treatment withKeto conazole was 12 days and after that she is not on medication).
DISCUSSION
Asthmatic pulmonary eosinophilia is usually seen in the 4th or 5th decade of life but occasionally in younger adults. The incidence in women is more than twice that in men.
Pathological examination shows areas of alveolar and interstitial exudate containing numerous eosinophils, sometimes also neutrophils, lymphocytes and plasma cells, and in some cases there are granulomata containing giant cells. In most of the cases there is infiltration of bronchial lumen and walls with eosinophils -There are areas of arteritis sometimes with actual necrosis4.
Radiologically there are characteristically recurrent abnormal shadows, one shadow clearing to be replaced by others, usually bilaterally and are common in upper zones. The shadows are relatively homogenous, though sometimes there is mottling and occasionally there are bizarre shadows resembling plaits of hair, or “Clouds of Smoke” rising after an explosion, in the region of hilum and drifting up against the chest wall peripherally5.
Occasionally the total white tell count is over 2O,00 per mm3 and eosinophil counts as high as 82%. Precipitins for these fungi are usually present in the blood serum in patients with positive skin or provocation tests. Fungi may not be readily cultured from the sputum and repeated attempts may be necessary. Scraps of mycelium may be identified in the sputum, plugs or casts, with appropriate staining, eosinophils are often present in large numbers in the sputum5.
The differential diagnosis is with those of pulmonary tuberculosis, pulmonary infarcts and large local consolidations from carcinoma of bronchus.
Treatment of the syndrome is routine therapy for asthma often corticosteroid drugs and of specific treatment for fungi. The prognosis of this entity is very variable. Recurrent attacks over weeks, months and sometimes years are not uncommon. Some recover completely and remain symptom-free indefinitely. Death may occur but this is related primarily to the asthma rather than to the pulmonary eosinophilia.
ACKNOWLEDGEMENT
I gratefully acknowledge the help, interest and advice of Dr. Khurshid Ahmed, Pathologist of Islámabad Hospital Complex, Islamabad.
REFERENCES
1. Perys, J., Faux Jennifer, A., Longbottom Joan, L., McCarthy, D.S. and Hargreave, RE. Candida albicans precipitins in respiratory disease in man. J. Allerg.,1968;41 :305.
2. Pepys, J., Riddell, R.W., atron, K.M., Clayton, Y.M. and Short, E.I Clinical and immunologic significance of aspergillus fumigatus in the sputum. Am.Rev. Tuberc., 1959;80:l67.
3. Bell, R.J.M. Pulmonary infiltration with eosinophils caused by chlorpropamicie. Lancet, 1964; 1:1249.
4. Liebow, A.A. and Carrington, C.B. The eosinophilic pneumonias. Medicine, 1969; 48:251.
5. Crofton, J.W., Livingstone, J.L., Oswald, N.C. and Roberts, A.T.M. Pulmonary eosinophilia. Thorax, 1952; 7 :1.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: