
M.S. Khan ( Chemistry Department, Islamia University, Bahawalpur, Pakistan. )
Parveen Akhtar ( Chemistry Department, Islamia University, Bahawalpur, Pakistan. )
Abdul Majeed ( Chemistry Department, Islamia University, Bahawalpur, Pakistan. )
October 1987, Volume 37, Issue 10
Original Article
Abstract
Uric acid concentration in serum and urine of 296 persons of Bahawalpur city is reported. Although the general pattern corresponds to the studies in other regions of the world but the range of uric acid concentration in male and female serum and uric acid is slightly higher. Correspondingly the incidence of uricemia is also high in the region with some cases of gout. Statistically, the serum urate level were more compact and had smaller coefficient of variance. Only persons with serum urate level above 125mg/lOOmI showed signs and symptoms of gout (JPMA 37: 266 , 1q87).
INTRODUCTION
Uric acid is a nitrogenous waste product of amino acid metabolism1 and plays a significant role in the evolution and ecology of vertebrate life2. Uric acid nitrogen constitutes 60-90% or more of the total urinary nitrogen3. Urate appears in blood mainly in free form and the serum urate concentration represents a dynamic balance between uric acid production and its disposition2. In normal human beings renal excretion accounts for 57-77% of the body’s daily production of uric acid4. Most of the remainder is excreted into gastrointestinal tract where it is degraded by enteric bacteria5. Its production may be regulated by the amount of various substrates which include ribose-5-phosphate. glutamine, glycine and aspartic acid and their induction of increased activities and amounts of enzyme involved in uric acid synthesis6 Serum uric acid may be considerably increased in starvation due to accelerated tissue turnover and decreased renal excretion of uric acid resulting probably from acidosis that accompanies starvation7. Bahawalpur region, a hot area with low annual rainfall, is considered as water deficient area. Low intake of water and consequently smaller volume of urine, results in higher uric acid concentration in the urine an’d poor uric acid secretion within the nephron, causing in-creased serum urate levels. The present studies were carried out to observe the normal and abnormal excretory pattern of uric acid in Bahawalpur Region and to correlate the results with increased incidence of uricemia and gout in the region.
MATERIAL AND METhOD
A total of 296 (159 male and 137 female) persons were randomly selected for this study.
Samples of blood and urine were collected from the Pathology Department of .Quaid-i-Azam Medical College, Bahawalpur, different localities and private clinical laboratories in Bahawalpur city.
Uric acid in blood, serum and urine was estimated by phosphotungstic reduction .method and the concentration of uric acid/lOOmI of the sample was determined photometrically8 (Tables I—IV).
RESULTS AND DISCUSSION
Normal uric acid levels have been quoted as 375 moles! litre in women and 425 moles/ litre in men8. These values are equivalent to 63rng/lOOml and 7.l4mg/lOOml of uric acid(Mol. Wt: 168) for females and males respectively.
The subject were divided into two groups:
Group—I: Subject with normal uric acid level in blood serum. These were 157 in number i.e., 87 males and 70 females.
Group-II: Subject with abnormal uric acid level in blood serum. These were 139 in total i.e., 72 males and 67 females.
In the present study 453% of the male and 48.9% of the female subjects under the survey were found hyperuricemic. The prevalence of hyperuricemia varies among the people of the world. In England only 23% of females were found hyperuricemic9: In France 17.6% of the total men surveyed were found hyperuricemic10. However, more than 40% of serum urate values of the three Polynesian groups exceeded the limits for the normal uric acid serum levels11. By corn parison, the serum urate values obtained in the present survey were comparable to those for the Polynesian people and much higher than the corresponding values for the people from the West. Subjects were further classified into different age groups (Table I-IV).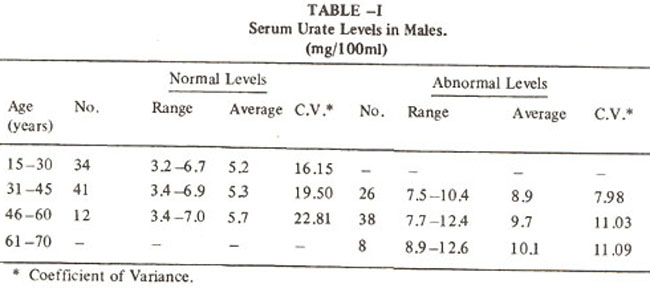
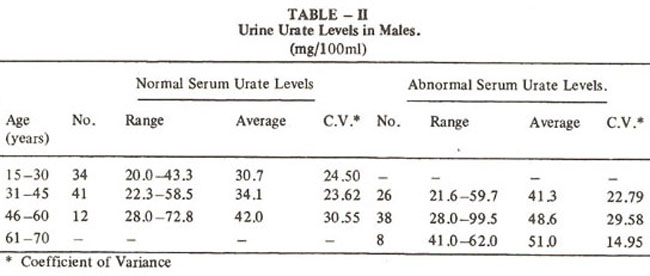
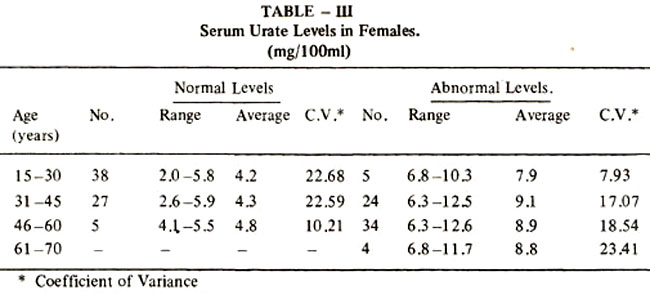
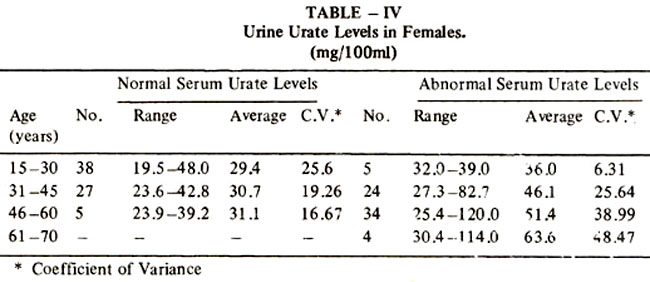
A trend for increased uric acid values in serum and urine was observed with the advancing age and with a difference in values between the sexes. These results conform with those reported by other workers7,9,12 . We found serum uric acid and urinary uric acid levels higher in males than in females, in all the age groups. Age and sex relationship strongly suggested endocrine influence on serum uric acid11. Androgens may be impor tant regulatory factors. Estrogen and possibly progesterone are also of importance as indicated by the fact that female subjects have lower uric acid level.
As both the serum urate and urine urate levels increased progressively with age, it can be concluded that hyperuricemia aggravates with age. It was also observed that with the increase in the serum urate level there was a corresponding increase in the urine urate level, indicating that the amount of uric acid transported from plasma to tubular fluid was mainly dependent on the initial serum urate level.
Statistical analysis showed that the abnormal urate levels were more compact than the corresponding values for the normal serum urate levels for males as well as for females. Serum urate levels of the subjects showed higher percentage of scatter of individual values around the mean of samples group observations. However, such a comparison was not possible for urine urate levels. Urine urate levels were found not only higher than the corresponding serum urate levels for all the age groups, these also showed higher coefficient of variance. It was, therefore, concluded significant in determining the cases of hyperuricemia and untreated gout. A higher fraction of the subjects under the present study was also hyperuricemic.
High serum urate levels of the subjects may be due to low water intake, hot weather, purine rich diet and genetics. Bahawalpur region is a hot area with low annual rainfall and is considered as water deficient area. Low intake of water or heavy perspiration may result in smaller volume of urine with higher ccncentration of uric acid, also in poor uric acid sccretion within the nephron thuc causing increased serum urate leveL. That hot climate is a factor responsible for higher uric acid concentration can be deduced from comparison of 3ur results with those of a similar study carried out in Karachi12. As Bahawalpur has a much severe dry hot climate as compared to Karachi, the urate levels in serum and urine in all age groups under study, both male and female, respectively, were higher for Bahawalpur than for Karachi. Hqwever, the raised levels of serum urate occur in wide variety of the circumstances and do not necessarily establish the diagnosis of gout. In the present study patients only with serum urate levels above I 2mg/lOOml showed signs and symptoms of gout (1.69%).
REFERENCES
1. Gutman, A.B. and Yu, T.F. Renal function in Gout; with a commentary on the renal regulations of urate excretion and the role of kidney in the pathogenosis of gout. Am. J. Med., 1957;23: 600.
2. Seegmiller, J.E., Laster, L. and Howell, R.R. Biochemistry of uric acid and its relation to gout. N. Engi. J.Med.. 1963; 268:712.
3. Benedict, J.D., Farsham, P-H and Statten, D. Jr. The metabolism of uric acid in the normal and gouty human studied with the aid of isotosic uric acid. J. Biol. Chem., 1949; 181 :183.
4. Seegmiller, J.E., Grayzel, A.I., Laster, L. and Liddle, I. Uric acid production in gout. J. Clin. Invest.,1961;40:1304.
5. Sorensen, L.B. The elimination of uric acid in man studied by means of C14 -labelled uric acid, uricolysis. Scand. J. Clin. Lab. Invest., 1960;12 (Suppi. 54): 1.
6. Muramatsu, T. and Okumura, J. Effect of dietary methionine and arginine on uric acid excretion of cocks fed a protein-free diet. J. Nutr., 1979;109 :1057.
7. Todd, J.C. Clinical diagnosis and management by laboratory methods. Edited by Israel Davidson and John Berrard Henry. 14th ed. Philadelphia. Saunders, 1969.
8. Swash, M. and Mason, S. Hutchinson’s clinical methods. 17th ed. London, Billier Tindall, 1980, p.371.
9. Hall, A.P., Barry, P.E., Dawber, T.R. and McNamara, P.M. Epidemiology of gout and hyper uricemia; a long term population study. Am J. Med., 1967;42: 27.
10. Zalokar, J., Lellouch, J., Claude, J.R. and Kuntz, D. Serum uric acid in 23,923 men and gout in a sub sample of 4527 men in France. J. Chronic Dis., 1972;25:305.
11. Prior, l.A., Rose, B.S. and Harvey, H.P. et al. Hyperurecemia, gout and diabetics abnormality in Polynesian people. Lancet, 1966; 1: 333.
12. Rehman, A. and Naqvi, S.A. Serum and urinary uric acid in relation to age and sex. JPMA., 1980; 30:242.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: