
Huma Qureshi ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Anjum Shahid ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Sarwar J. Zuberi ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Rashida Hassan ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
S. Ejaz Alam ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
June 1987, Volume 37, Issue 6
Original Article
Abstract
Thirty non azotemic cirrhotics with ascites were treated with oral diuretics on outpatient basis. Estimation of 24 hrs urinary sodium levels proved useful in the diagnosis of secondary hyperaldosteronism (63.3% cases) and the determination of type and dose of diuretics required. Prompt and effective clearance of ascites occurred within 4 weeks of the therapy. No adverse effects were noted and no hospitalisation was required. The regimen was found to be cost effective for developing countries (JPMA : 37 : 142, 1987).
INTRODUCTION
Ascites is one of the commonest complications of cirrhosis of the liver and diuretics are still the drugs of choice for its treatment. Furosemide and spironolactone are the two commonly used drugs either alone or in combination.
Furosemide, a potent loop diuretic, often fails to produce adequate natriuresis in cfrrhotics because of the aldosterone mediated effect on the increased reabsorption of sodium and excretion of potassium in the distal nephrone resulting in kaliuresis without natriuresis1.
Indirect assessment of sodium handling by the nephron can be judged by the determination of 24 has urinary sodium excretion. An excretion of less than 60 meq/L is often associated with secondary hyperaldosteronism2, which responds well to increasing doses of spironolactone until the urinary sodium levels exceed 60 meq/L. Addition of furosemide at this stage further enhances the diuretic effect.
A study was undertaken to determine the frequency of secondary hyperaldosteronism and the requirement of aldosterone antagonists in cirrhotics.
MATERIAL AND METHODS
PATIENT SELECTION
Thirty non-azotemic cirrhotics with moderate to severe ascites were selected for the trial. Except for the few cases already admitted in the hospital, all were treated on outpatient basis. All diuretics were stopped for 5 days and salt intake was restricted. None of the patients were bleeding from the upper G.I. tract or had hepatic encephalopathy or any acute infection during the trial.
BIOCHEMICAL INVESTIGATIONS
Twenty four hours urine was collected for sodium and potassium estimation. Blood samples were taken for the determination of glomerular filteration rate (GFR), electrolytes, urea and creatinine. GFR was determined by creatinine clearance, electrolytes by flame photometry, urea by diacetyl method using thiosemicazbazide3, and creatinine by the method of Broad and Sirota4.
REGIMEN
The diuretic regimen followed is shown in Figure.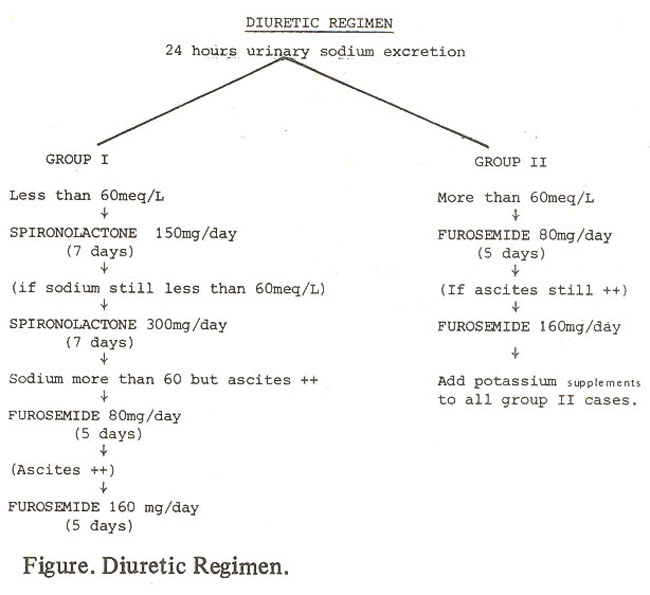
Depending upon the 24 his urinary sodium levels, the patients were divided into group I (sodium < 60 meq/L) and group II (sodium> 60 meq/L). The initial doses of spironolactone and furosemide were 150 and 80 mg/day, respectively, given at 8.00 A.M. The doses were increased to 300 and 160 mg/thy, respectively (half the dose given at 8.00 A.M. and half at 4.00 P.M), if there was no response i.e. mean wt. loss was less than 200 g/day, or the urinary sodium levels were still less than 60 meq/L. Furosemide 80 mg/thy at 8.00 A.M. was added to group I when, though the urinary sodium excretion increased to more than 60 meq/L, but ascites was still moderately present. The dose of fumsemide was doubled (half the dose given at 8.00 A.M. and half at 4.00 P.M.) if ascites persisted. Complete drying of ascitic fluid was avoided. Spironolactone was not added to the group II patients but oral potassium supplements given in doses varying between 120-180 mg/thy.
Body weight, urinary volume, serum and urinary electrolytes were determined in each case before and during the trial at an interval of 5-7 day depending upon the diuretic used.
Statistical analysis was done using paires student 't' test.
RESULTS
Of 30 cirrhotics with ascites, 633% had secondary hyperaldosteronism (< 60 meq sodium excretion/L) and therefore belonged to group I. Liver and renal function tests and the frequency of oedema before the diuretic therapy in the two groups is shown in Table I.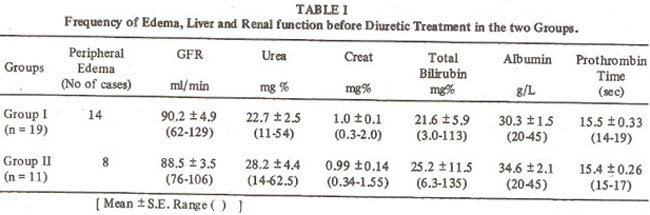
Creatinine clearance,a measure of GFR, urea and creatinine were within normal limits in the two groups. Serum bilirubin was slightly elevated and albumin low in both the groups.
The mean changes in the body weight and serum and urinary electrolytes in the two groups before and after the diuretic therapy are shown in Table II.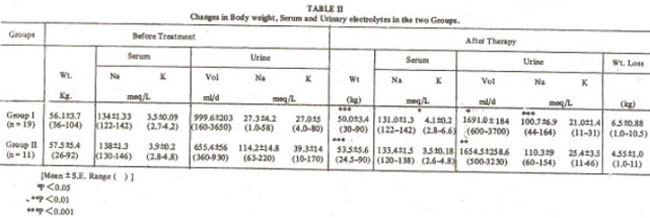
Except for urinary sodium levels in group II significant differences were noted in the body weight and urinary volume in the two groups after 4 weeks of diuretic therapy. ln group I serum potassium levels increased significantly with spironolactone therapy while urinary potassium levels showed an insignificant fall.
During the treatment period which lasted for 4 weeks a gradual increase in urinary volume and sodium excretion was noted in both groups at the end of each week, peaking around 4th week. Weight loss per week was noted for 3 weeks after which a slight weight gain (4.7 kg) was seen, which probably reflects the actual weight gain after the clearance of excess of ascites. Serum potassium levels were maintained within the normal limits in all the cases (Table III).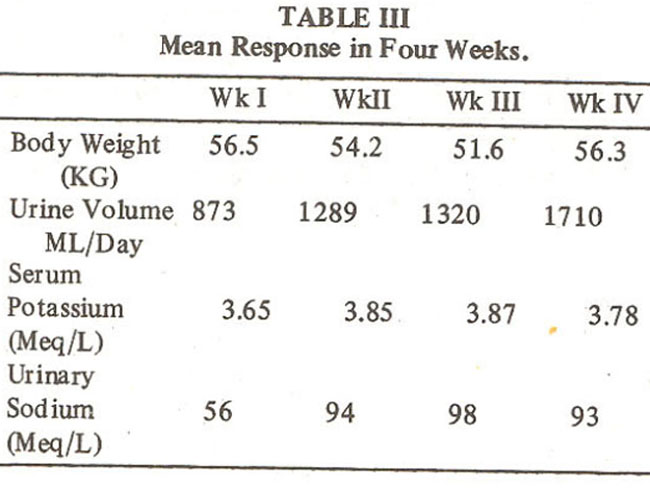
DISCUSSION
About 63% cases in the present study had urinary sodium levels under 60 meq/L and it was therefore assumed that they were all conserving sodium under the influence of aldosterone, or that they probably had secondary hyperaldosteronism. Diuretic response in these patients was good when aldosterone antagonists were given followed by furo semide.
Due to lack of awareness of the importance of urinary sodium excretion per day and the role of renin and aldosterone in producing ascites, most cirrhotics with ascites are initially treated with oral furosemide. The non-responders are given high doses of parenteral furosemide, resulting in electrolyte imbalance especially of potassium. Paracentesis causes further deterioration of their condition resulting in hepatic coma or hepatorenal syndrome and claiming almost 100% mortality.
The dose of spironolactone varies from patient to patient5, but is usually related directly to the degree of hyperaldosteronism and doses as high as 500-1000mg/day may be required5,6.Although the urinary sodium levels were less than 10 meq/L in 26% of the patients in the present study, none of them required more than 300mg of spironolactone to overcome aldosterotie mediated sodium reabsorption. About 1/3rd of cirrhotics without renal failure have normal plasma aldosterone levels,7-9 but spironolactone is still helpful in these cases to revert sodium reabsorption probably due to increased tubular sensitivity to aldosterone10. In spironolactone treated patients in this study, mean serum potassium levels increased without causing a concomitant reduction in urinafy potassium excretion. Similar results were reported in other studies1,6 The present results are quite contrary to the classical view that increased serum potassium levels are due to its decreased excretion in the urine11. The actual causes of increased potassium levels are not yet clear.
In developing countries like ours where cost of treatment is of prime importance and most diuretics given on hit and trial basis, a cost effective diuretic regimen for cirrhotics with ascites is suggested. In areas where facilities for electrolyte estimation are available, a base line electrolyte estimation would help in the determination of the type and dose of diuretic required. Isolated estimation of urinary electrolytes especially sodium per week would thereafter help in the determination of response. In areas lacking in laboratory facilities spironolactone may be used as the drug of first choice; because more than 50% cases are likely to have low urinary sodium levels. The regimen of treatment for these cases would be the one followed in group I in the present series. This blind regimen of treatment is cost effective because the total cost of treatment per patient for 4 weeks comes to approximately Rs.350/- which is far less than that required for hospitalisation, random allocation of diuretics and later paracentesis and its complications.
REFERENCES
1. Perez-Ayuso, R.M., Arroyo, V., Planas, R., Gaya, .J., Bory, F., Rimola, A., Rivera, F. and Rodes, J. andomized comparative study of efficacy of furosemide versus spironolactone in noriazotemic cirrhosis with ascites. Relationship between the diuretic resoonse on the activity of the remnaldosterone system. Gastroenterology, 1983; 84:961.
2. Krupp, M., Chaitton, M.J. Current medical diagnosis and treatment. Los Altos California, Lange, 1984, p.411.
3. King, E.J. Micro-analysis in medical biochemistry, by l.D.P. Wooton. 5th ed. London, Churchill, 1974, p. 74.
4. Brod, J. and Sirota, J.H. The renal clearance of endogenous “creatinine” in man. J. Clin. Invest., 1948; 27: 645.
5. Eggert, R.C. Spironolactone diuresis in patients with cirrhosis and ascites. Br. Med. J., 1970; 4:401.
6. Campra, J.L. and Reynold, T.B. Effectiveness of high dose of spironolactone therapy in patients with chronic liver disease and relatively refrac tory ascites. Dig. Dis., 1978; 23:1025.
7. Arroyo, V., Bosch, J., Mauri, M., Viver, J., Mas, A., Rivera, F. and Rodes, J. Renin, Aldosterone and renal hemodynamics in cirrhosis with ascites. Europ.J.Clin.Invest., 1979;9:69.
8. Wilkinson, S.P., Smith, I.K. and Williams, R. Changes in plasma renin activity in cirrhosis;a reappraisal based on studies in 67 patients and “low renin” cirrhosis. Hypertension, 1979; 1:125.
9. Reynolds, T.B. Portal hypertension/in the liver. Edited by Arias, I.M., Frankel, M., Wilson, J.H.P. Oxford, Princeton, 1982, p. 233.
10. Wilkinson, S.P. and Williams, R. Reninangio tensin-aldosterone system in cirrhosis. Gut, 1980; 21:545.
11. Gussin, R.Z. Potassium sparing diuretics. J. Clin. Pharmacol., 1977;17:651.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: