
Bahu S. Shaikh ( Department of Medicine, Medical College of Ohio, Toledo, Ohio, U.S.A. )
January 1987, Volume 37, Issue 1
Special Communication
Abstract
The modern blood bank came into existence less than fifty years ago as one of the byproducts of knowledge gained during the second world war. The blood banks then could supply only two products as compared to the modern blood bank which is capable of supplying over 17 highly specialized blood cormponents.
This paper reviews the history and progress made in the transfusion of blood and its components and makes specific r ecommendations for the proper use of packed red blood cells, platelets, white cells and fresh frozen plasma (JPMA 37: 13, 1987).
HISTORICAL NOTES
Forty years ago the blood banks were only called to supply whole blood and plasma from outdated blood. The blood bank operation has now become very sophisticated and about 17 products are available from the modern blood bank (Table I).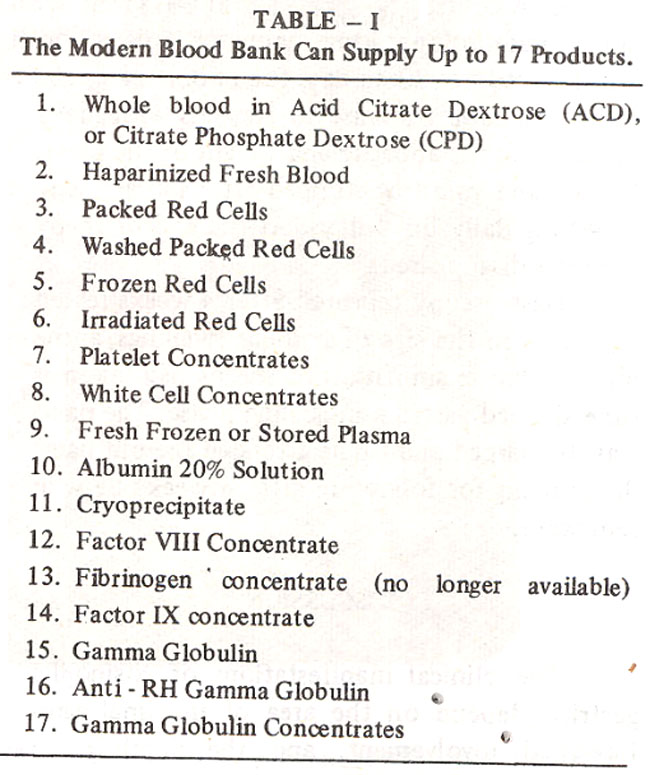
It is therefore appropriate to recapitulate the history of blood transfusions and review how much progress has been made possible. According to Bernheim, “If the history of blood transfusion were charted it would present a picture not unlike that of an intermittent fever with it’s even ups and downs, it’s periods of quiescence, some longer than others, followed by acute outbreaks until the gradual drop to normalcy and recovery.1
Egyptians were said to have advocated the use of blood baths for rejuvenation. The Romans were encouraged to drink the blood of the fallen adversary. Blood is mentioned more than 500 times in the bible and in Quran. The eating of blood, however, is forbidden in Christianity. Jehovan’s Witnesses interpret this very rigidly, therefore they refrain from all sorts of transfusion therapy.
As late as the fifteenth century, blood was used to treat lunacy, fits, palsy, and melancholia, but not anemia. Up until the 17th century blood was given only by mouth. In the seventeenth century when Harvey discovered circulation and wrote his latin treatise called “De Motu COrdis” which means the motion of the heart, the modern era of blood transfusion had just begun.2
The first transfusions were carried out in animals. In 1667, Richard Lower of Oxford performed direct transfusions from one dog to another. At the same time, in France, Denis was performing transfusions in sheep. The first human transfusion were performed later that year. Since animals were used as donors, transfusion reactions were soon being reported. Here is a description of one of the first transfusion reactions reported by Denis: “His arm became hot, the pulse rose, sweat burst out on his forehead, he complained of pain in the kidneys, and was sick at the stomach. The next day the urine was very dark, in fact, it was black.3 In 1667 the first death due to sheep blood transfusion was recorded4. Nothing new was accomplished until 1774 when Priestley and LaVoisier discovered the role of oxygen in respiration5. In 1817, Blundell found that death from hemorrhage could be prevented by blood transfusion in dogs6. Further progress in this area is shown in Table II.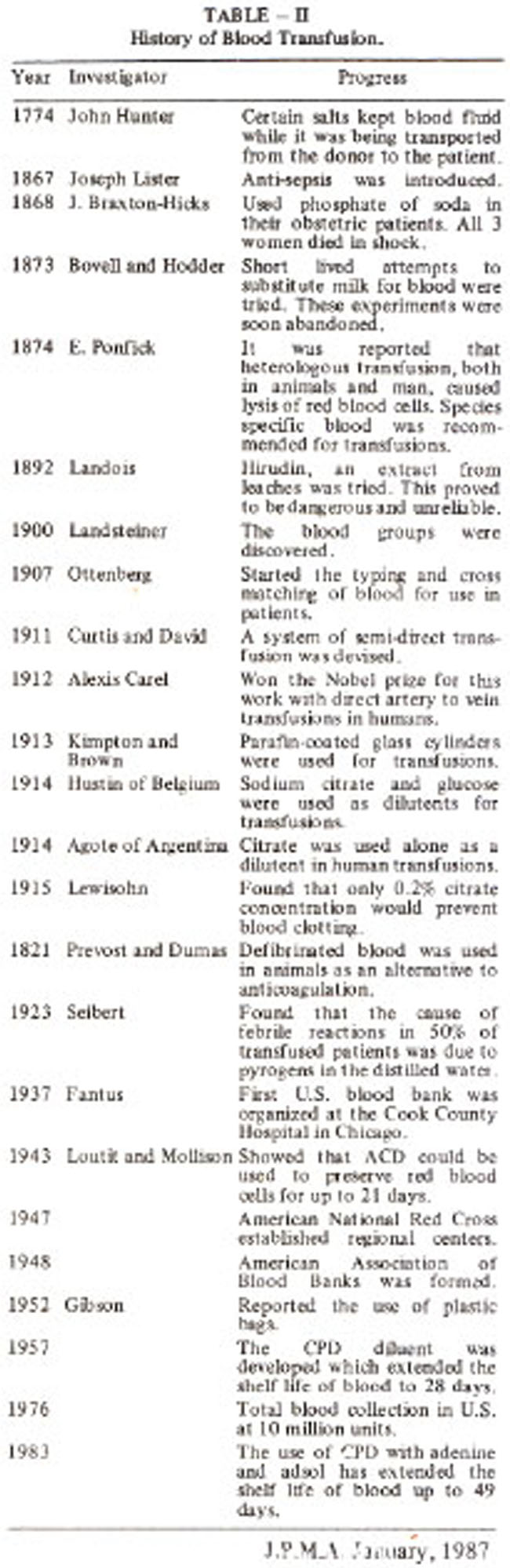
RATIONAL USE OF BLOOD PRODUCTS
PRINCIPLES OF TRANSFUSION THERAPY
1) The cause of deficiency should be identified.
2) The deficient component should be replaced.
3) The blood product selected should be as safe as possible for the need of the patient.
PROCEDURE FOR RED CELL TRANSFUSION
A 19 gauge or larger needle should always be used for transfusing red cells. The duration of the transfusion should not extend beyond four hours per unit. For patients who experience febrile - transfusion reactions with red cells (presumably due,to the presence of white cell), leukocyte poor red cell components are available.
Traditionally leukocyte poor red blood cells have been processed by two methods, centrifuge and the automated cell washer methods. The RBC obtained by the centrifuge method are cheaper than those obtained by the cell washer. The centrifuge method, of course, does not remove as many of the white cells as the cell washer. A third method which is called the spin and filter method has been described recently6. This method is cheaper than the other two, and it removes as many leukocytes as the buffy coat poor blood obtained by the other two methods. This method is being promoted as more cost effective. The technique is quite simple and is described below (Table III).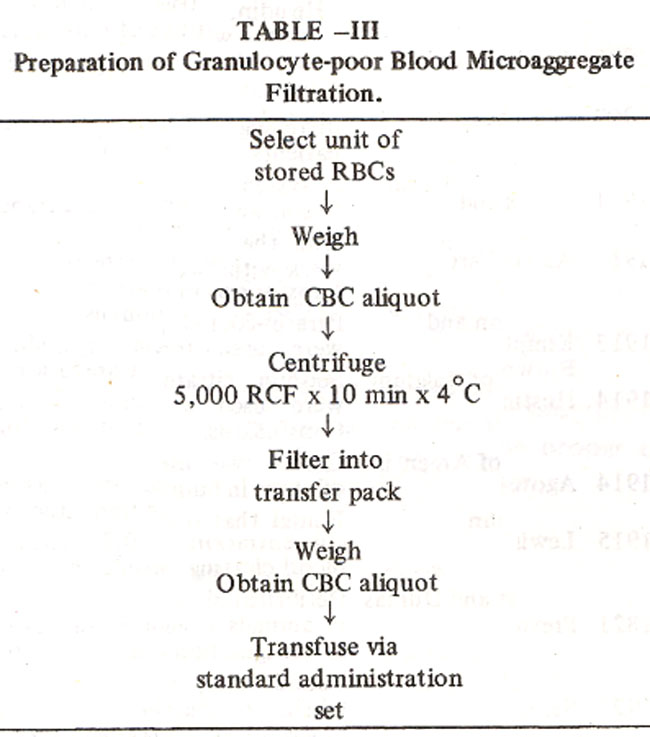
The unit is centrifuged at 5,000g for 10 minutes at 4°C. A microaggregate filter, such as a Pall filter, is used during the administration. This method is very effective in removing most of the contaminating white cells which are usually responsible for the febrile reactions seen in the patient who has received multiple transfusions. A comparison of these three methods is shown in Table IV.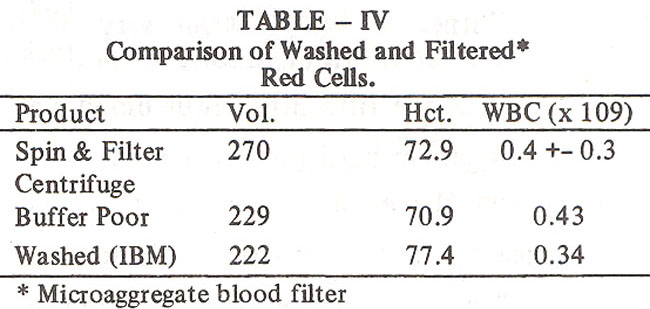
Another red cell product available is the frozen red cells. The advantages and disadvantages of frozen red cells are listed in Table V.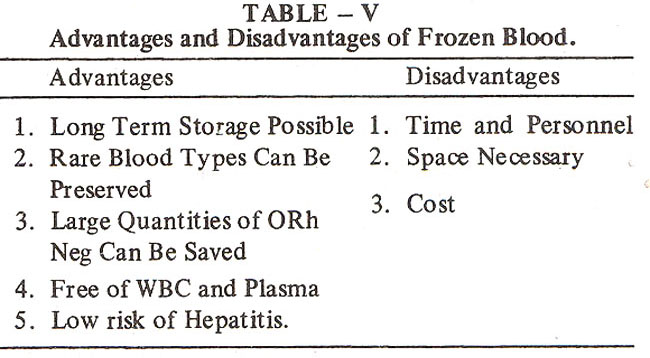
The need for the’ red cell transfusion can easily be calculated. A good rule to remember is: one unit of packed red cells in an adult raises the hemoglobin by one gram or the hematocrit by 3%.
This formUla makes it simple to calculate the requirement for red cells in adults.
DVERSE EFFECTS OF BLOOD
TRANSFUSION
Besides the transmission of various diseases such as hepatitis-B, non-A non-B hepatitis, infectious mononucleosis, cytomegalovirus inclusion disease, malaria, and acquired immune deficiency syndrome (AIDS)8, one can also transmit bacteria during transfusions which can cause septicemia, especially if there is an infection present in the donor. The dilution of blood constituents can cause thrombocytopenia and clotting factor deficiencies. Embolism can occur, microemboli from aggregates of blood may cause problems. Circulatory overload is not an uncommon result. This could be in the form of fluid or electrolyte imbalance, such as hyperkalemia. Iron overload can occur in the chronically transfused individuual This can be prevented and treated by using iron chelating ..compound such as deferoxamine to chelate the
The unit is centrifuged at 5,000g for 10 minutes at 4°C. A microaggregate filter, such as a Pall filter, is used during the administration. This method is very effective in removing most of the contaminating white cells which are usually responsible for the febrile reactions seen in the patient who has received multiple transfusions. A comparison of these three methods is shown in Table IV. Another red cell product available is the frozen red cells. The advantages and disadvantages of frozen red cells are listed in Table V.
The need for the’ red cell transfusion can easily be calculated. A good rule to remember is: one unit of packed red cells in an adult raises the hemoglobin by one gram or the hematocrit by 3%.
Advantages Disadvantages
This formUla makes it simple to calculate the requirement for red cells in adults.
ADVERSE EFFECTS OF BLOOD
TRANSFUSION
Besides the transmission of various diseases such as hepatitis-B, non-A non-B hepatitis, infectious mononucleosis, cytomegalovirus inclusion disease, malaria, and acquired immune deficiency syndrome (AIDS)8, one can also transmit bacteria during transfusions which can cause septicemia, especially if there is an infection present in the donor. The dilution of blood constituents can cause thrombocytopenia and clotting factor deficiencies. Embolism can occur, microemboli from aggregates of blood may cause problems. Circulatory overload is not an uncommon result. This could be in the form of fluid or electrolyte imbalance, such as hyperkalemia. Iron overload can occur in the chronically transfused individuual This can be prevented and treated by using iron chelating compound such as deferoxamine to chelate the extra iron from the body and prevent or delay the onset of an iron overload state9.
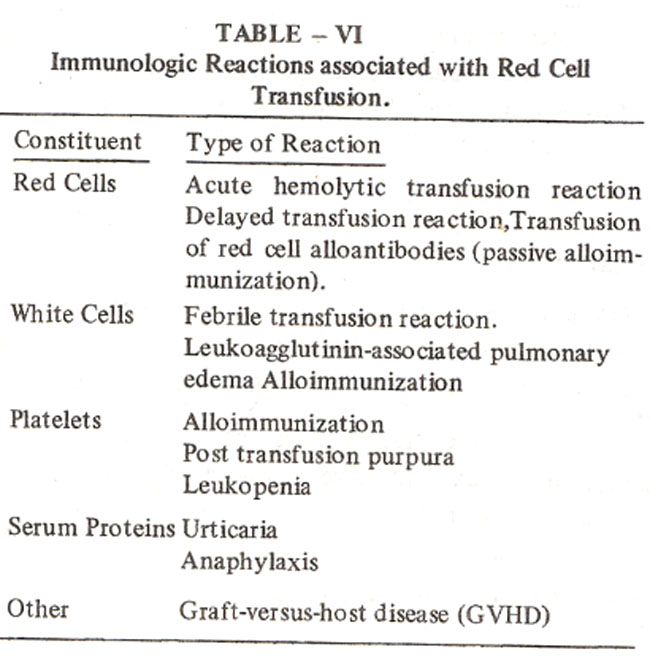
The immunologic reactions shown in Table VI indicate that red cells can cause either immediate or delayed hemolysis. White cells can cause febrile reactions and pulmonary infiltrates. Platelet antibodies can cause post-transfusion purpura. Plasma proteins can cause anaphylactic shock, urticaria and nonspecific protein febrile reactions which are quite common. Graft versus host disease is uncommon and only occurs in patients who are extremely immunocomprised10. in such patients we suggest the use of irradiated blood cells. Of the fatal hemolytic reactions reported to the Federal Drug Administration in the U.S.A. over a three year period of time, 44 were immediate reactions and two were delayed. Of these, 33 were due to ABO incompatibility. Five were presumed ABO incompatibffity and the rest were due to a variety of other problems11.
Most of the errors that accounted for the incompatibility were clerical and occurred during collection or ordering of the blood. The sample was either drawn from the wrong person or given to the wrong recipient. To emphasize what has just been said, most of the deaths from transfusions are not because of a difficulty in matching the blood or because of a, serologic problem, but due to human or ,clerical ewors. Therefore, everyone handling blood or blood samples for transfusion should continue to be very careful with the identification of the proper donor samples as well as transfusing the correct unit of blood to the receipient. These problems are magnified in the specialized units, such as the operating rooms or the Intensive Care Units. Therefore, it is important to have proper procedures to prevent such accidents in these units.
WHAT SHOULD BE DONE IF THE HEMOLYTIC TRANSFUSION IS SUSPECTED?
1) Stop the blood transfusion.
2) Check for clerical information.
3) Obtain blood samples from the patient and order tests to look for infection, coagulation dysfunction, and renal function abnormalities. The blood samples should be sent to the blood bank for further serologic testing.
WHAT ARE THE COMPLICATIONS OF MASSIVE
BLOOD TRANSFUSION?
Bleeding is due to the dilution of clotting factors and platelets. This occurs only after two blood volumes have been replaced which would be equal to a 5-10 liter transfusion in an adult. Citrate toxicity occurs in patients who are given very rapid transfusions of over one unit every five minutes, or those who have impaired liver function. Hypothermia can result in arrhythmias and poor release of oxygen. Stored blood is deficient in 2,3-DPG, this can cause less efficient delivery of oxygen. At three weeks the stored blood also has a high potassium content (30 mEq/L). The rapid transfusion of such blood may potentiate hyperkalemia in the susceptible individuals.
WHAT ARE THE DIFFERENCES BETWEEN THE
TYPE AND SCREEN AND TYPE AND CROSSMATCHING OF BLOOD?
Type and screen may uncover patient donor incompatibility in 1 in 1,000. The cost is higher and it takes about 5 minutes more to process the request when blood is needed, safety is the same. There is no blood wasted this way and this product should be used for bloodless surgery. If a type and cross match is done, the blood is typed and screened and in addition, a compatibility check is performed. Rare incompatibility will be found by this method. The cost is about 3 times higher. The safety is the same because the typed and screened blood is cross-matched before it is released. Two days of the shelf life are lost this way. The main use of this product should be expected for surgery during which blood replacement is usually necessary.
PLATELET TRANSFUSION
It should be noted that when the platelet count is over l00,000/pl there is no risk of any significant bleeding, either from trauma or otherwise. When the platelet count falls below 50,000 there is a significant risk of bleeding from minor trauma or spontaneous bleeding. This risk continues to go up as the platelet count falls and in patients with platelet counts below 20,000 there is a moderate risk of spontaneous bleeding and below 5,000 the risk of serious bleeding is quite high. Therefore, prophylactic platelet transfusions are suggested for patients who have platelet counts below 10- 20,000 range. In adults each unit of platelets is expected to raise the platelet count by approximately 5-8,000/pl. Therefore,6-8 units of random donor platelets are transfused in adults at one given time. Platelets cannot be stored for long periods of time in the blood bank. They are stored at room temperature and can only be used for 72 hours. Therefore, it is a good practice to inform the blood bank about your expected needs in advance.
WHITE CELL TRANSFUSIONS
Bodey has shown that patients do not get an increase in the infection rate until their absolute neutrophil count falls below 1,000/u12 Below this level there is a step-wise increase in the number of infections because of neutropenia. Several series have studied the use of white cells to control infection in patients with malignancy2. From 1972-1982 at least seven such series were reported. Some were randomized and cross-matched, some reported significant benefit, while others reported little or no benefit at all13-16 White cell transfusions are not free of hazards or side effects, like anything in medicine, the risk benefit ratio has to be considered. Acute toxicity includes fever, hypotension, the transmission of CMV, hepatitis, toxoplasma, graft-versus host disease, pulmonary toxicity from leukoagglutinin reactions and from CMV pneumonia.
We recommend the use of white cell transfusions in the neutropenic patient only after appropriate antibiotics have been given for 24-48 hours. Therapeutic leukocyte transfusions of more than 1 x 1017 can benefit a patient who has the following criteria: 1) An absolute neutrophil count of less than 500/u 2) a documented bacterial infection, 3) no response to appropriate antibiotics within 48 hours, and 4) a marrow recovery is expected to occur within a few weeks. Such patients are expected to benefit from therapeutic granulocyte transfusions. There are presently no recommendations for prophylactic use of granulocyte transfusions, as one cannot maintain the body’s massive demand for granulocytes, and the risks of such an approach far outweigh the benefits.
THE RATIONAL USE OF FRESH FROZEN PLASMA (FFP)
We surveyed 364 units of fresh frozen plasma that was used at the Medical College of Ohio Hospital between April and July, 1982. We developed the criteria for appropriate use of these products and analyzed the patterns of their use. One hundred twenty two units were used solely for blood pressure support, 126 units were used for clotting support, and 52 units were used for the combined reasons of blood pressure and clotting support. Forty units were used for therpatuic pheresis17. It is clear from this study that a substantial number of FFP units are used mainly for volume expansion. This is no longer justified as safer and cheaper products such as human serum albumin, dextran and starch solutions are available as good colloid substitutes.
REFERENCES
1. Bernheim, B.M. Adventures in blood transfusion. New York, Smith and Durrell, 1942; p.182.
2. Harvey, W. Exercitatio Anatomica De Motu Cordis et Sangiunis in Animalibus. Birmingham, The Classics of Medicine Library, 1978.
3. Wiener, A.S. Blood groups and transfusion. 3rd ed. Sprinfield,Thomas, 943; p. 51.
4. Siewers, A.B. A case of madness cured by blood transfusion. Bull. Hist. Med., 1938; 6: 1010.
5. Wintrobe, M.M. Blood, pure and eloquent; a story of discovery, of people and of ideas. New York, McGraw-Hffl, 1980; p. 665.
6; Blundell, J. Observations on transfusion of blood by Dr. Blundell with a description of his gravitator. Lancet, 1828;2: 321.
7. Parravicini, A., Rubella, P., Apuzzo, J., Wenz, B. and Sirchia, G. The preparation of leukocytepoor red cells for transfusion by a simple cost-effective technique. Transfusion, 1984; 24:508.
8. Conrad, M.E. Diseases transmissible by blood transfusions; viral hepatitis and other infectious disorders. Semin Hematol., 1981; 18 : 122.
9. Propper, R.D., Cooper, B., Rufo, R.R., et al. Continuous subcutaneous administration of deferoxamine in patients with iron overload. N. Engl. J. Med., 1977; 297: 418.
10. Ford, J.M., Lucey, J.J., Cuilen, M.H., Tobias, J.S. and Lister, T.A. Fatal graft-versus-host disease following transfusion of granulocytes from normal donors. Lancet, 1976;2 : 1167.
11. Myhre, B.A. Fatalities from blood transfusion. JAMA., 1980;244:1333.
12. Bodey, G.P., Buckley, M., Sathe, Y.S. and Freireich, E.J. Quantitative relationships between circulating leucocytes and infection in patients with acute leukemia. Ann. Intern. Med., 1966; 64 : 328.
13. Graw, R.G. Jr., Herzig,G., Perry, S. and Henderson, E.S. Normal granulocyte transfusion therapy; treatment of septicemia due to gram negative bacteria. N. EngI. j Med., 1972; 287:367.
14. Higby, D.J., Yates, J.W., Henderson, E.S., et al. Filtration leukapheresis for granulocyte transfusion therapy; clinical and laboratory studies. N. Engl. J.Med., 1975;292 :761.
15. Schiffer, C.A., Aisner, J. and Wiernik, PH. Current status of granulocyte transfusion therapy, In the granulocyte; function and clinical utilization. New York, Alan R. Liss, 1977; p.281.
16. Higby, D.J. and Henderson, E.S. Supportive care of the seriously ill cancer patient. Platelet and granulocyte transfusion therapy, in oncologic emergencies. Eds. Yarboro, J.W., Boinstein, R.S. Newyork, Grune and Stratton, 1981; p. 323.
17. Shaikh, B.S., Wager, D., Lau, P.M. and Campbell, E.W. Jr. Transfusion pattern of fresh frozen plasma in a medical school hospital. Vox Sang., 1985;48 : 366.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: