
Manzoor Ahmad ( Armed Forces Institute of Pathology, Rawalpindi. )
Azhar Mubarik ( Armed Forces Institute of Pathology, Rawalpindi. )
M. Mumtaz Khan ( Armed Forces Institute of Pathology, Rawalpindi. )
November 1990, Volume 40, Issue 11
Case Reports
INTRODUCTION
Hibernoma is a rare benign tumour of brown fat. It is also known as lipoma of brown adipose tissue, lipoma glandular and atypical lipoma. The hibernoma was first described by Merkelin 1906, who called it Pseudolipoma1. The name hibernoma is derived from its histological similarity to the brown fat of hibernating animals2. They have been found in the neck, back, popliteal space, thighs, axilla, abdominal wall and the mediastinum. They may recur if not completely excised. Malignant change in hiberqoma is not known to occur3. The purpose of this study is to document the cinicopatbological and microscopic features of this rare tumour. An attempt is also made to ascertain its relative frequency to other tumours arising from fatty tissue.
MATERIAL AND METHODS
All the tumours arising from fatty tissue were reviewed from 1984-1989. The specimens were received in AFIP from the various military hospitals of the country and the civil hospitals of the Northern Punjab, adjacent NWFP and Azad Kashmir. These specimens were fixed in 10 percent neutral buffered formaldehyde, and representative blocks were routinely processed, embedded in paraffin, sectioned, and stained with Hematoxylin- Eosin. Some tissue was frozen, sectioned and stained with oil red 0. During the six year period, a total of 1410 fatty tissue tumours were diagnosed. Out of which 28 (1.98%) were malignant and 1382(98.02%) were benign (Table).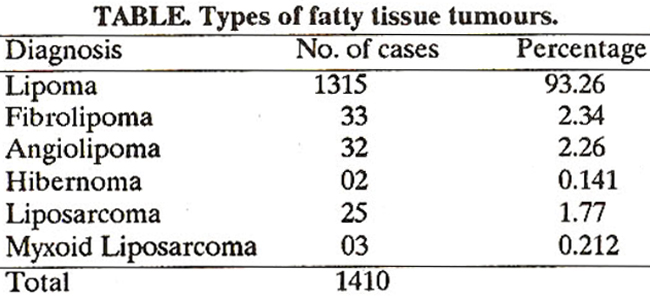
Out of these benign tumours only 2 cases (0.144%) were hibernomas.
CASE NO.1
A 24 years old male patient preselited with a painless swelling just below right scapula for the last two and a half years. Excision biopsy was done and a brownish fatty lump was removed having the size 3 x 2 x 1.5 cm. The surface was nodular. On cutting it was soft in consistency. Cut surface was brownish in colour On microscopic examination the tumour consisted of groups of cells with eosinophilic granular cytoplasm and a central bland nucleus. A few adult fat cells were also present (Figurel).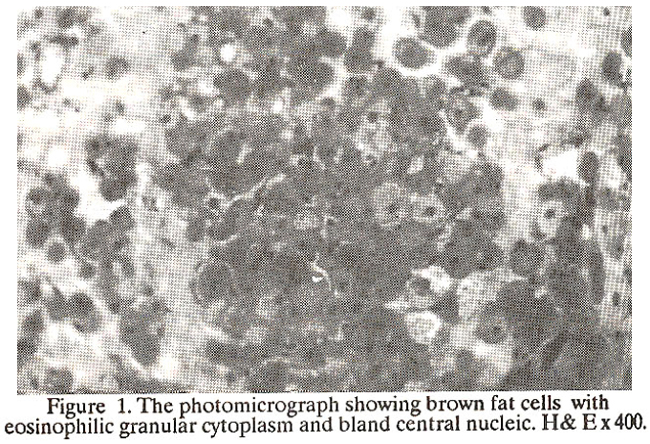
On higher magnification the cells were multinucleated-Mulberry cells (Figure 2).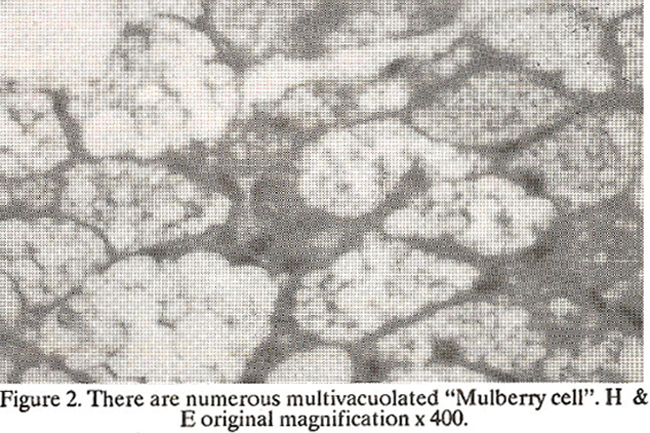
The swelling recurred after 2 years and attained a diameter of 8cms approximately. It was removed and submitted for histopathological examination. Microscopy revealed morphology similar to the previous picture.
CASE NO.2
A young man complained of gradually increasing painless swelling in the nape of the neck for the last few years. It was about 5 cm in diameter. The swelling was not giving any problem to the patient apart from being a cause of worry. Excision biopsy was done On gross examination the specimen consisted of a lump of fibrofatty tissue measuring 5 x 5 x 2cm in size. The external surface was irregular and granular in appearance (Figure 3).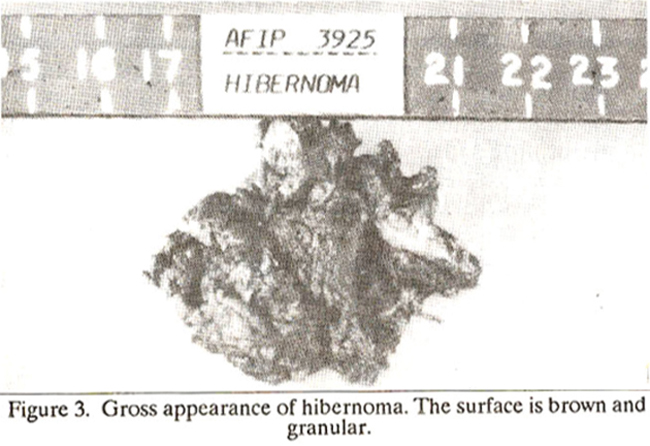
On cutting it was soft in consistency. Microscopic examination revealed sheets of cells having multiple small vacuolation with central round nuclei. Some of the cells showed large univacuolated cells with eccentric nuclei (Figure 4).
There was no evidence of malignancy seen in either case.
DISCUSSION
Although the benign tumours of white fat are extremely common, those arising from brown fat are among the rarest, with only 80 cases being reported in literature till 19864. We saw only two cases in six years. Hibernoma have occurred in all ages, from infants to adults in their sixties with peak incidence in the 2nd decade5. There is no sex preponderance6. Hibernomas have histological, histochemical ultrastructural, biochemical and metabolic similarly to brown fetal fat7. Brown fat occurs only in a few specific places in infants like in the neck, interscapular region, mediastinum, posterior abdominal wall, around the kidneys and adrenals and also in the pancreas. Brown fat rapidly decreases after the first eight weeks of life, although small quantities remain in all age groups, principally in deep locations such as around the kidneys and adrenals8. However, increased amounts of brown fat have been reported in sudden infant death syndrome9, in adults with chronic hypoxemia, hypothermia and in outdoor workers10 and in patients with pheochromocytomas11. Interestingly endocrine like activity resembling that of adrenal cortical tissue has been detected in one case. Brown adipose tissue can develop preferentially in certain anatomical locations in response to local, environmental, hormonal or immunological stimuli7. Majority of hibernomas have been reported to arise from the inter-scapular region. In both our cases the tumours rose from the scapular region. However, hibernoma may arise even where brown fat is absent, such as the thigh, buttock and popliteal fossa13. Histologically, the cells are arranged in small lthules separated by delicate well-vascularized fibrous septa. Three principal cell types could be distinguished in each hibernoma but their proportion varies from case to case7.
(1) A round cell (average size 47 urn) with granular eosinophilic cytoplasm, (2) a large, multivacuolated cell (average size 54 urn) with scanty granular eosinophilic cytoplasm (mulberry cells) and (3) a univacuolated adipocyte (average size 65 urn). Nuclei of granular and mullivacuolated tumour cells are usually central and nuclei of univacuolated adipocyte are eccentric. On frozen sections stained with Sudan Black, anisotropic crystals resembling cholesterol crystals can be seen in the cytoplasm of many cells. Electron microscopic studies have revealed a similarity between hibernoma cells and those found in animal brown fat. A characteristic finding is the presence of moderately pleomorphic mitochondria having transverse cristae. 14The superficial resemblance of hibernomas, microscopically, to granular cell myoblastoma, lipoblastoma and histiocytic fibrous histiocytoma should be kept in mind at the time of diagnosis. Hibernomas are cured by simple excision. Some consider round cell liposarcoma to be the malignant counterpart of hibernoma but no definite evidence exists4. However, Symmers15 reported a possible malignant form in a 3 months old boy who died with brownish red nodules throughout the abdominal cavity which on histological examination resembled brown fat.
REFERENCES
1. Merkl, H. Uberein Pseudolipom der Mamma., Beitr. Pathol. Anat., 1906; 39: 152.
2. Dardick, I. Hibernoma : A possible model of brown fat histogenesis. Hum. Athol., 1978; 9: 321.
3. Stout, A.P. and Lanes, R. Tumours of the soft tissues. Wahington Armed Forces Institute of Pathology, 1967.
4. Rigor, V.U., Goldstone, S.E., Jones, J. et al. Hibernoma a case report and discussion of a rare tumour. Cancer, 1986; 57: 2207.
5. Seemayer, T.A., Knaack, J., Wang, N.S. and Ahmed, M.N. On the ultrastructure of hibernoma. Cancer, 1975; 36: 1785.
6. Lawson, W. and Biller, H.F. Cervical hibernoma. Laryngoscope, 1976; 86: 1258.
7. Gafney, E.F., Hargreaves, H.K., Semple, E. and Vellios, F. fibernoma; distinctive light and electron microscopic features and relationship to brown adipose tissue. Hum. Pathol., 1983; 14: 677.
8. Heaton, J.M. The distribution of brown adiposed tissue in the human. J. Anat., 1972; 112 : 35.
9. Naeye, R.L. Hypoxemia and sudden infant death syndrome. Science, 1974; 196: 837.
10. Huttenunen, P., Hirvonen, J. and Kinnula, V. The occurrence of brown adipose tissue in outdoor workers. Eur. J. AppI. Physiol., 1981; 46: 339.
11. Medeiros, L.J., Katsas, G.G. and Balogh, K. Brown fat and adrenal pheochromocytoma. Hum. Pathol., 1985; 16: 970.
12. Allegra, S.R., Gmuer, C. and O’Leary, G.P. Jr. Endocrine activity in a large hibernoma. Human Pathol., 1983; 14: 1044.
13. Kindblom, LG., Angervall, L., Stener, B. and Wickborn, 1. Inter muscular intramuscular lipomas and hibernomas, a clinical, roentgenologic, histologic, and prognostic study of 46 cases. Cancer, 1974; 33: 754.
14. Levine, G.D. Hibernoma; an electron microscopic study. Hum. Pathol., 1972; 3: 351.
15. Symmers, D. Spindle and giant cell sarcoma arising from unidentified precordial bodies. Arch. Pathot., 1944; 37: 180.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: