
Waquar Uddin Ahmed ( Pakistan Medical Research Council, Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Huma Qureshi ( Pakistan Medical Research Council, Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
S. Ejaz Alam ( Pakistan Medical Research Council, Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Sarwar Jehan Zuberi ( Pakistan Medical Research Council, Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
October 1990, Volume 40, Issue 10
Original Article
ABSTRACT
Two hundred and forty-five endoscopically proven or surgically treated duodenal ulcers were retrospectively evaluated to see if the site of ulcer has any influence on the clinical presentation, and healing and relapse rates. Anterior wall ulcer was present in 42%, posterior wall in 33%, lesser curve side of the cap in 12% and greater curve side in 13% cases. Ulcer site showed no correlation to age, sex, duration of illness, analgesic intake or smoking habits. Bleeding (116 cases) and perforation (15 cases) were the major complications encountered; of these perforation was invariably found on the anterior wall, while bleeding was more frequent in ulcers present on the lesser curve side of the cap. Better healing and high relapse rates were seen in ulcers situated on the greater curve, and low healing and relapse rates in lesser curve duodenal ulcers (JPMA 40 : 238, 1990).
INTRODUCTION
The site of duodenal ulcer and its influence on the mode of presentation has been studied by many workers1,2. Earlier studies have shown a higher frequency of perforation in anterior wall ulcers and bleeding in posterior wall ulcers1,2. Anatomical protection of the other sites of the duodenal cap except the anterior wall and the close association of blood vessels on the posterior wall are said to influence perforation and bleeding in such cases2, however supportive evidence to correlate repeated bleeding episodes and the presence of blood vessels in the ulcer crater is lacking3. The present study was done to determine if the site of duodenal cap ulcers had any correlation to its presentation, healing or relapse rates in our patient population.
PATIENTS AND METHODS
Retrospective analysis of 599 patients with duodenal ulcer diagnosed either on endoscopy or at surgery was done. The site of duodenal ulceration was recorded as anterior wall, posterior wall and lesser curve and greater curve side of the cap. Only those cases in whom the site of duodenal ulcer was known were included in the analysis. Patients with prepyloric and postbulbar ulcer were excluded from the study. The site of duodenal ulcer was correlated with its mode of presentation, healing and relapse rates and its relation to the risk factors. Statistical analysis was done using x2 and student ‘t’ test.
RESULTS
Five hundred and ninety nine cases of duodenal ulcer were reviewed retrospectively. Complete information on the site of ulcer was available in 275 cases; of these, prepyloric (17), post bulbar (6) and big ulcers involving the whole cap (7) were excluded. Finally 245 cases were found fit for analysis. Site of ulcer: Anterior wall ulcer was present in 42%, posterior in 33%, greater curve side of the cap in 13% and lesser curve side in 12% cases. Age, sex & addictions: Duodenal ulcer was maximally seen in the 3rd and 4th decade of life, with a strong predominance of male sex (4: 1 to 9: 1) in all age groups. Age, sex and smoking habits showed no correlation to the site of ulcer (Table I). Duration of illness: There was wide variation in the duration of the disease in various groups, which ranged from 1 month to 50 years, mean being 52 months. Patients with anterior wall duodenal ulcer had a significantly longer duration of the illness than others (P <0.001). Analgesic intake: History of analgesic intake especially NSAIDs was present in 24% cases having a lesser curve side duodenal ulcer, 13% in greater curve and 2.4% in posterior wall ulcers while none of those with anterior wall ulcer were on such drugs (Table I).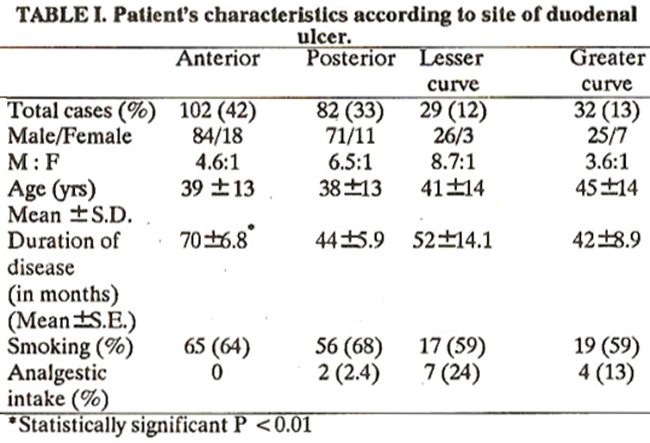
Presenting features: The main presenting features of duodenal ulcer disease are pain, bleeding, perforation and stenosis. Although epigastric pain was the commonest presenting symptom in all the patients, it was significantly more frequent in those with an anterior wall ulcer (Table II).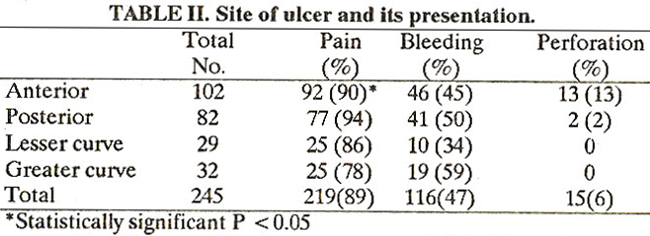
Except for lesser curve duodenal ulcers, which bled infrequently, all other ulcers showed equal bleeding rates. Of 15 patients who underwent laparotomy for perforated duodenal ulcer, 13(13%) had an anterior wall perforation. Site of perforation at surgery was not mentioned in two cases but both of them showed a posterior wall duodenal ulcer on post-operative endoscopy. None of the patients in the present series presented with pyloric stenosis. Healing and relapse rates: Of 245 patients with duodenal ulcer, 163 (66%) patients came for follow up. Repeat endoscopy after 4-6 weeks of therapy with one of the H2 receptor antagonists showed complete healing in 104 (64%) cases. Healing rates were highest (84%) in patients with a greater curve and lowest (50%) in lesser curve ulcers (Table III).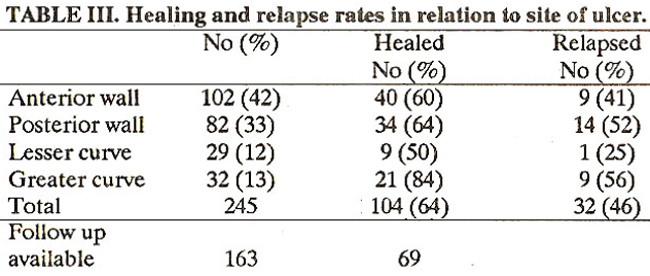
Sixty-nine cases completed a 2 years follow up while they were on a maintenance therapy of H2 receptor antagonists. Of these 32 (46%) showed a relapse despite taking the drug regularly (Table III). Healing and relapse rates showed direct correlation to the ulcer site, i.e., sites showing highest healing rates also showed the highest relapse rate and vice versa.
DISCUSSION
Specific anatomical features have not been detected so far which can explain the usual sites of duodenal ulcer; however site of duodenal ulcer reported initially in postmortem studies which was later coitfirmed at operation and on endoscopy, have shown that ulcers ile close to the pylorus, either on anterior or posterior wall and lesser curve or greater curve side of the bulb2,4,5. Present study has shown that duodenal ulcers mostly (75%) lie on the anterior or posterior walls of the bulb and a few (25%) lie on lesser or greater curve side, which confirms earlier studies. Perforation was invariably found on anterior wall of the bulb in this series. At operation duodenum is usually found flattened so surgeons can recognize only anterior or posterior wall and it is nearly impossible to recognize lesser and greater curve. Perforation of duodenal ulcer is known to occur mostly on anterior wall, as has been reported before4; Ischaemia at the site of ulcer is probably the cause behind it4. Earlier observations have shown that traction on the stomach causes an area of pallor on the anterior duodenal wall at the similar site where anterior duodenal ulcers often form6. Thus filling of the stomach, with food might be producing some gastric displacement and duodenal traction to produce an ischaemic area. Subsequent attack of acid on this area might be leading to ulceration and perforation. On the contrary posterior wall ulcers are less likely to perforate as no such ischaemia is produced on traction and that part is provided and added protection by stomach bed. Hemorrhage is the most likely complication of posterior wall ulcer due to its anatomical relation to big duodenal blood vessels7. Fortunately most of the bleeding duodenal ulcers donot erode major vessels so the magnitude of this problem in relation to the site of ulcer still has to be sorted out. We could not find any significant preponderance of posterior wall ulcers in patients who presented with hemorrhage, except for comparatively low frequency of bleeding in lesser curve ulcers and high frequency among greater curve side, without any statistical significance. The present study showed highest healing (84%) and relapse rates (56%) among ulcers situated on the greater curve side as compared to those at other sites. Lowest healing (50%) and relapse (25%) rates were found among lesser curve side ulcers. Although both (lesser and greater curve sides of the cap) of these areas are very vascular because of close proximity of gastroduodenal and left gastric artery, both these areas behaved differently when healing and relapse were evaluated. Further studies on a larger group of patients are required to determine the affinity of various sites of ulcers to various complications and their varied response to healing and relapse rates.
REFERENCES
1. Bailey, H. Emergency surgery, edited by Hugh A.F. Dudley, 10th ed. Bristol, Wright, 1977, p.401.
2. Kang, J.Y., Nasiry, it, Guan, R., Labrooy, S., Lim, K.P., Yap,!. and Piper, D.W. Influence of the site of a duodenal ulcer on its mode of presentation. Gastroenterology, 1986; 90: 1874.
3. Storey, D.W., Bown, S.G., Swain, C.P.,Salmon, P.R., Kirkham, J.S. and Northfield, T.C. Endoscopic prediction of recurrent bleeding in peptic ulcers. N. Engl. J. Med., 1981; 305 : 915.
4. Kirk, R.M. Site and localization of duodenal ulcers; a study at operation. Gut, 1968 ; 9 : 414.
5. Nanivadekar, S.A., Tandon, N.H., Kuloor, P.L., Bichile, L.S., Tahiliani, R.R., Vijan, V.and Sahu, C.P. Comparative frequency of duodenal and gastric ulcers in Bombay. Indian J. Gastroenterol., 1984; 3: 77.
6. Mayo, WJ. Anemic spot on the duodenum which may be mistaken for ulcer. Surg. Gynecol. Obstet., 1908; 6: 600.
7. Swain, C.P. When and why do ulcers bleed and what can be done about it. Aliment. Pharmacol. Therap., 1987; 1: 455.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: