
Najam Arif ( Department of Gastroenterology, Shaikh Zayed Hospital, Lahore. )
Anwar A. Khan ( Department of Gastroenterology, Shaikh Zayed Hospital, Lahore. )
Zafar Iqbal ( Department of Gastroenterology, Shaikh Zayed Hospital, Lahore. )
January 1990, Volume 40, Issue 1
Original Article
Abstract
Salmonella typhi has been reported to cause hepatic involvement. We studied nine patients with positive blood cultures in order to identify characteristic features of typhoid hepatitis which may help in early diagnosis. Patients who had an illness resembling enteric fever but negative cultures for Salmonella typhi were excluded.
No specific ôlinical features were found consistently and liver function tests were widely variable. Other biochemical abnormalities occurred due to vomiting and renal involvement. Liver biopsy showed focal hepatocellular necrosis and non specific inflammation. Although most responded to conventional antibiotics, it was generally a delayed response.
It is recommended that patients with fever greater than 38.5°C and liver abnormalities should undergo blood, urine, stool and/or bone marrow cultures. Liver biopsy may help to differentiate typhoid hepatitis from acute viral hepatitis (JPMA 40: 4, 1990).
INTRODUCTION
Enteric group of fevers is common in Pakistan1. Typhoid fever affects most of the body systems and simulates many infectious diseases. The classical step-ladder fever, relative bradycardia and leukopenia2 are not as frequent now as previously reported. The atypical features of typhoid fever are being increasingly noted3,4.
When typhoid fever involves the liver, the picture may resemble viral, malarial and amoebic hepatitis: all of which are common diseases in this region. It is important to differentiate between them as the treatment differs. A profile of nine patients with typhoid fever and hepatic involvement is being reported here to help identify characteristic features contributing to early diagnosis.
MATERIAL AND METHODS
Patients with blood culture positive typhoid fever who underwent evaluation of liver function tests and showed abnormalities in the history or laboratory tests, were selected for reporting. Patients with an illness resembling typhoid fever clinically, and/or positive Widal test but negative blood, urine and stool cultures for Salmonella typhi were excluded.
A detailed history was obtained and physical examination was carried out bn admission and laboratory tests were performed.
RESULTS
Eight patients with positive cultures and liver abnormalities were seen over a period of fifteen months (October 1987-December 1988) at the Shaikh Zayed Hospital, Labore, in the Department of Gastroenterology. One patient (No.9) was seen on reference from another hospital.
The symptoms, physical signs, haematological values, liver function tests, and other biochemical tests are shown in tables I-IV.
Ages ranged between 12 and 32 years (mean age 22 years). The only common features were non-specific symptoms like fever, vomiting and abdominal pain (Table I).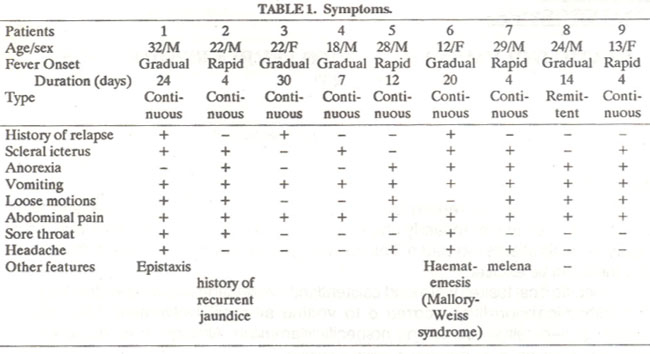
Relative bradycardia, scieral icterus, hepatomegaly and splenomegaly were not regular features (Table II).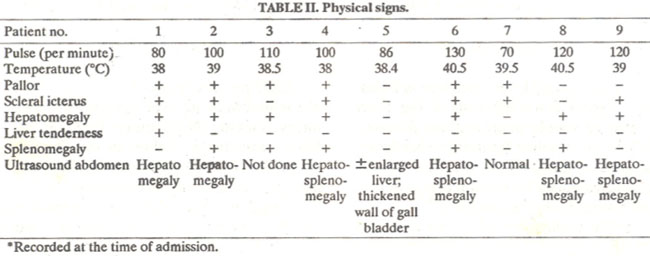
Most patients became anaemic during the course of their illness; ESR fluctuated from normal to veryhigh (Table III), leukopenia was seen in only two patients, thrombocytopenia in two and raild abnormalities of prothrombin time were noted.
Hyponatremia was a feature in all patients. Serum potassium was found to be low or at lower limit of normal (Table III). These biochemical changes were attributed to vomiting seen in all patients. Two patients developed renal failure which reverted to normal after recovering from the illness. Most patients had proteinuria and hematuna, regardless of development of renal failure (Table III).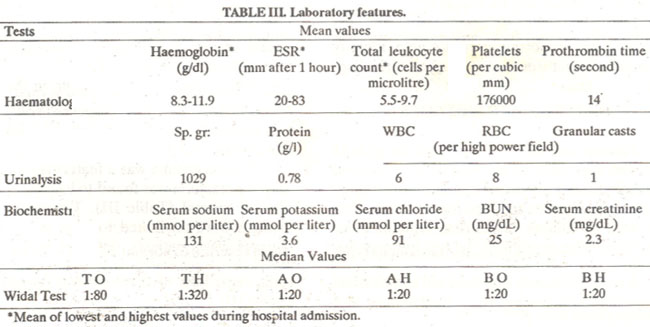
The picture of liver function tests was widely variable. Some patients showed normal serum bilirubin whereas in others it was more than 20 mg/dl. Generally, the illness was more severe when there was hyperbilirubinemia. The levels of alkaline phosphatase also varied widelybut did not correlate with the degree of hyperbilirubinemia. The levels of SGPT and SGOT ranged from normal to about 300 lU/I and these did not correlate with the severity of disease, degree of hyperbilirubinemia or the levels of alkaline phosphatase (Table IV).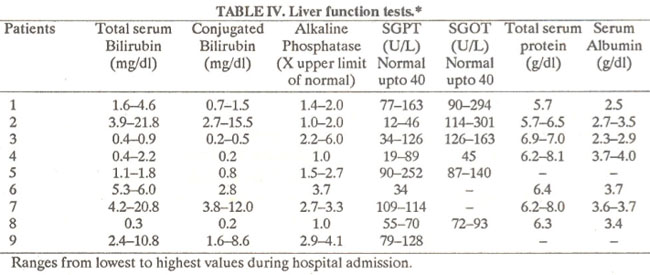
Serum albumen was frequentlyfound to be in the lower range.
Widal test became positive in all patients. S. typhi (TH) titers were more sensitive than S. typhi (TO) (Table III). All patients had positive blood cultures for Salmonella typhi and one grew Salmonella paratyphi B as well.
Four patients underwent liver biopsy which showed normal lobular architecture and liver cell plates, fatty change, bile stasis, bile plugs, mononuclear infiltrate in portal tracts, foci of hepatic inflammation and necrosis, Kupifer cell hyperplasia and acidophil bodies.
In addition, urine cultures were done in four patients: all were negative and stool culture in one case was also negative for salmonella typhi. Only one patient out of nine had liver biopsy culture and another had bone marrow cultures done: both were positive for salmonella typhi.
The total duration of illness ranged from 16 to 47 days (mean 31 days). Most patients required hospitalization for more than two weeks. A delay response to therapy for ten days or more was seen in most patients (Table V).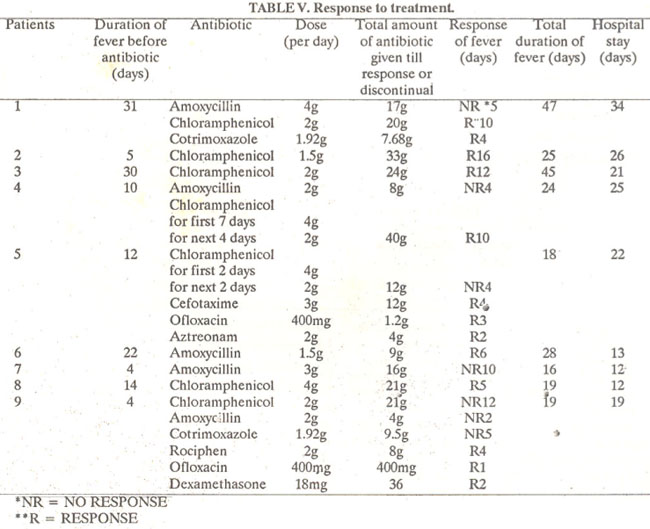
One patient had S. typhi resistant to chioramphenicol, amoxycillin and cotrimoxazole (Patient 5). Patient No.7 had not responded after 10 days of therapy and left against medical advice.
Large doses of antibiotics did not seem to produce a rapid response (Table V) but one patient (No.9) responded within two days of initiating dexamethasone therapy. Those who responded to chioramphenicol usually did so after more than 20 grams had been given. In all patients icterus and liver function abnormalities returned to normal as fever subsided.
DISCUSSION
Typhoid fever involving the liver may have no features of hepatic involvement or may manifest as icterus, hepatomegaly, abnormal liver function tests and abnormal liver histology. The reported incidence of different liver abnormalities in typhoid fever varies widely (Table VI).
The effect of typhoid fever on pre-existing liver disease is unknown. Except one patient who had a questionable history of recurrent jaundice, none of our patients had any history suggestive of past liver disease.
Numerous factors may predispose patients to hepaticinjuryin typhoid fever. Patients suffering from anaemia, malnutrition and poor health may have liver involvement and a more severe disease12. Although most of our patients belonged to the lower and middle class, none of them was apparentlymalnourished. All 7 cases with jaundice reported by Gupta et al4 had gut perforation and septic peritonitis, and jaundice was ascribed to ascending cholangitis. Although it was frequently suspected, none of our patients had proven gut perforation. It is perhaps due to the reason that most of our patients were not exposed to corticosteroid therapy unlike the patients reported by Gupta et al. Three out of four patients with jaundice reported by Wicks et al6 had haemolytic jaundice; two had G6PD deficiency and renal failure and one had hemolysis without renal failure. Only one of our patients showed evidence of haemolysis. G6PD level was not estimated.
The mechanism of hepatic damage is obscure. Although the incubation period and severity of disease are known to be related to the infecting dose of the organisms13,14, it is not known whether the occurrence of hepatitis is related to the infecting dose, virulence of (he organism, or susceptibility of the host. Hepatitis early in the disease indicates severity; its development during the period of defervescence has been suggested as a sequel to intestinal ulceration7. Other possible factors leading to hepatic injury in typhoid fever include endotoxic damage to hepatocytes, endotoxin induced consumptive coagulopathy33,36, localized DIC and arteritis14. Cholangitis4 and direct tissue invasion by salmonella typhi may be another reason. The role of endotoxins in the production of illness in typhoid has been speculative17.
Immune complexes have been shown in typhoid fever and significantly more frequently in those patients with complications including hepatitis18. The same studyalso showed consumption of complement suggested by a high ratio of antitrypsin to C3.
A reduced number of helper T cells and increased number of suppressor T cells was shown during the second week in patients with complicated typhoid fever16. Recovery from the illness to normal was correlated with the development of cell mediated immune response.
Case reports of typhoid fever with hepatitis have shown other associated abnormalities like nephritis21,22 thrombocytopenia22, haemolyticuraemic syndrome23, hacMolysis6,16, consumptive coagulopathy15 and a haemorrhagic slate due to liver dysfunction and clotting factor deficiencr24. Most of our patients had urinary abnormalities like proteinuria, haematuria, pyuria, and granular casts, indicating some degree of nephritis. One patient developed the hacmolytic-uraernic syndrome. Significant thrombocytopenia was seen in only one patient: no other significant clotting abnormalities were encountered.
Two patients of typhoid fever with non-A non-B hepatitis reported by Caredda et al25 were probably cases of typhoid hepatitis. A liver biopsy which could have differentiated the diffuse picture of acute viral hepatitis from the focal changes of typhoid hepatitis was not done in these patients. Thus many cases of typhoid hepatitis may be mislabelled as non-A and non-B hepatitis and a treatable cause ofjaundicc maybe missed.
This marks the importance of performing liver biopsy in such patients to differentiate between viral hepatitis and typhoid hepatitis. Although features of hepaticinvolvernent in typhoid hepatitis are variable, it is important to further investigate for liver abscess, cirrhosis and viral hepatitis as these diseases are commonly encountered in this patient population.
In summary this study shows that the clinical features of typhoid hepatitis are extremely variable. Liver function tests show no typical features. There should be a high index of suspicion of typhoid hepatitis in patients with fever greater than 38.5°C and liver abnormalities. Such cases should undergo blood, urine, stool and bone marrow cultures. Liver biopsy may help in differentiating it from non-A and non-B hepatitis.
Prospective studies are indicated to determine its incidence and the factors leading to liver damage in typhoid fever. Moreover the contribution of typhoid hepatitis to the number of cases labelled as non-A non-B hepatitis in this region should be determined.
ACKNOWLEDGEMENTS
The help of Mr. Amjad Ali, Mr. Fakhar Mehmood and Mr. Asghar Ali in preparation of manuscript is gratefully acknowledged.
REFERENCES
1. World Health Organization, World 1-Icaith Statistics Annual. Geneva, WHO., 1983, P. 380.
2. Stuart, B.M. and Pullen, R.L. Typhoid; clinical analysis of 360 cases. Arch. Intern. Med., 1946; 78:629.
3. Gulati, PD., Saxcna, S.N., Gupta, P.S. and Chutani. FI.K. Changing pattern of typhoid fever. Am. J. Med., 1968; 45: 544.
4. Gupta, S.F., Gupta, M.S., Bhardwaj, S. and Chugh, T.D. Current clinical patterns of typhoid fever: a prospective study. J. Trop. Med. Ilyg., 1985; 88:377.
5. Rowland, H.A.K. The complication of typhoid fever. J. Trop. Med. ilyg., 1961; 64: 143.
6. Wicks, A.C.B., Holmes, G.S. and Davidson, L. Endemic typhoid fever. A diagnostic pitfall. Q. J. Med., 1971; 159: 344.
7. Ramachandran, S., Godfrey, J. and Perera, M.V.F. Ty phoid hepatitis. JAMA., 1974; 230 :236.
8. Diem, LV., My, T.O., chi, N.y., Nhon, N.T. and Thuc, T.K. Typhoid fever with hepatitis. J. Trop. Med. Hyg., 1976; 79:25-27.
9. Sarnantray, S.K., Johnson, S.C. and Chakrabarti, A.K. Enteric fever, an analysis of 500 cases. Practitioner, 1977; 218:400.
10. Singh, D.S., Nair, P.N.R., Krishnasamy, S., Aurora, A.L., Chandrasekar, S. and Bisht, D.B. Jaundice in typhoid fever. J. Trop. Med. Ilyg., 1978; 81: 68.
11. Johnson, A.O.K. and Aderele, W.1. Entcric fever in childhood. J. Trop. Med. Hyg, 1981; 84:29.
12. Khosla, S.N., Singh, R., Singh, G.P. and Trehan, V.K. The spectrum of hcpatic injuty in enteric fever. Am. J. Gastroenterol., 1988; 83:413.
13. Naylor, G.RE. Incubation period and other features of food-borne and waterbome outbreaks of typhoid fever in relation to pathogenesis and genetics of resistance. Lancet, 1983; 1:864.
14. Homick,R.B.,Greisman,S.E.,Woodward,T.E.,DuPont, H.L., Dawkins, AT. and Snyder, M. J. Typhoid fever, pathogenesis and immunological control (second of two parts). N. Engi. J. Med., 1970; 283:739.
15. Allen, N., Nomanbhoy, Y., Green, D. and Dunea, 0. Typhoid fever with consuñtption coagulopathy. JAMA., 1969; 208:689.
16. Rao, P.N., Bhusnurmath, S.R. and Nailk, S.R. Typhoid fever manifesting with haematemesis, hepatitis and haemolysis. J.Trop. Mcd. Hyg., 1978; 81: 146.
17. Greisman, S.E., Hornick, RB., Wagner, H.N. Jr., Woodward, W.E. and Woodward, T.E. The role of endotoxin during typhoid fever and tularemia in man IV. The integrity of the endotoxin tolerance mechanisms during infection. J. Clin. Invest., 1969; 48:613.
18. Rajagopalan, P., Kuniar, R. and Malaviya, A.N. Immunological studies in typhoid fever f Immunoglobulins, C3, antibodies, rheumatoid factor and circulating immune complexes in patients with typhoic fever. Clin. Exp. Immunol.. 1981;44:68.
19. Rajagopalan, P., Kumar, R. and Malaviya, A.N. Immunological studies in typhoid fever II. Cell-mediated immune responses and lymphocyte suhpopulations in patientswith typhoid fever. Clin. Exp. Immunol, 1982; 47 269.
20. Balakrishna Sarma, V.N., Malaviya, A.N., Kumar, R.., Chai, O.P. and Bakhtary, M.M. Development of immune response during typhoid fever in man. am. Exp. Immunol., 1977; 28 35.
21. Abu Romeh, S.H.,Al-Jamal, H., Hakim, A. and Patrick,J. Tubulo.. interstitial nephritis; an unusual complication of typhoid fever. Trop. Doct., 1988; 18:153.
22. Faierman, D., Ross, F.A. and Seckler, S.G. Typhoid fever complicatedbyhepatitis,nephritisandthrombocytopenia. JAMA., 1972; 221:60.
23. Baker, N.M., Mills, A.E., Rachman, 1. and Thomas, J.E.P. Haemolytic-umemic syndrome in typhoid fever. Br. Med. J., 1974;2:84.
24. Greig, H.B.W. and Naidoo, P.D. A case of typhoid fever complicated by a severe bleeding syndrome due to deficiencyofthe prothrombin group of coagulation factors. J. Trop. Med. Hyg, 1981; 84:253.
25. Caredda, F., Antinori, S., Re, T., Pastecchia, C. and Moroni, M. Acute non-A non-B hepatitis after typhoid fever. Br. Med.J., 1986; 292: 1429.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: