
Talat J. Hassan ( Pakistan Medical Research Council, Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Rakhshanda Baqai ( Pakistan Medical Research Council, Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
Sadiqua N. Jafarey ( Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. )
S. Ejaz Alam ( Pakistan Medical Research Council, Research Centre, Jinnah Postgraduate Medical Centre, Karachi. )
September 1991, Volume 41, Issue 9
Original Article
ABSTRACT
Maternal morbidity was observed in 377 obstetric cases at Jinnah Postgraduate Medical Centre (JPMC) during a period of one year. Morbidity rate was 4.4% of total deliveries. Three hundred and twenty-four (86%) mothers had no proper antenatal supervision. Infection was more common after abdominal delivery and injury to genital tract after vaginal delivery. The most serious injury was rupture of gravid uterus. Thirty-seven cases of ruptured uterus were admitted in one year and 5 cases occurred within the hospital (1 in 1225 deliveries). (JPMA 41: 223, 1991).
INTRODUCTION
Maternal morbidity is difficult to defineand, therefore, definitions differ. Recently, WHO1 defined reproductive morbidity as morbidity or dysfunction of the reproductive tract or any morbidity which is a consequence of reproductive behaviour including pregnancy, abortion, childbirth or sexual behaviour and has divided it into three groups: i) obstetric morbidity (ii) gynaecological morbidity and (iii) contraceptive morbidity.
Obstetric morbidity is further subdivided into direct and indirect. Direct obstetric morbidity results from obstetric complications of pregnant states (pregnancy, labour and the puerperium). Indirect morbidity results from previous existing disease which was aggranted by the physiologic effects of pregnancy.
Maternal morbidity is closely related to both maternal mortality and morlidity2. Some hospital date is available on maternal and perinatal mortality,3-9 but no published data or global estimate is available on maternal morbidity although it is a better index of maternal penalty of childbirth as the number of mothers suffering or invalidated greatly exceeds the number of deaths. Datta et al10 in a small study on 270 women in one Indian village, reported 16 episodes of illness for every maternal death. Thus a study was undertaken to obtain a baseline data regarding direct obstetric morbidity related only to
labour and delivery, their nature, extent and causes.
SUBJECTS AND METHODS
Subjects were selected from JPMC as this Institute drains a wide area of Karachi. During a period of one year, all patients developing complications during and after labour and delivery within the hospital, or admitted with complications after labour and/or delivery outside, were included in the study. Mothers with associated disease aggravated by pregnancy like anaemia, cardiac problems, hypertension, diabetes, or complications due to current pregnancy, like pre-eclampsia, eclampsia, antepartum haemorrhage or late sequelae after delivery like secondary infertility systocoele, were not included. Detailed history including previous obstetric history, details of present pregnancy, labour, medication and obstetric examination by medical and paramedical personnel were recorded on a specially designed proforma. Complete physical and obstetric examination at the time of admission was carried out. Any rise of oral temperature to 100.4°F (38°C) or above during first fourteen postoperative days excluding the first 24 hours was taken as puerperal pyrexia. Specific information about the complication was notified in detail. Investigation included complete blood picture, urine analysis, bacteriological examination, high vaginal swabs and wound swab if indicated. Other investigations like serum electrolytes were done only if necessary.
RESULTS
During a period of one year there were a total of 6249 obstetric admissions (excluding abortions) and 6128 deliveries (vaginal 5336 and abdominal 728).
Morbidity was observed in 377 patients. Of these, 324(86%) had not received antenatal care at JPMC. Of 272 mothers delivered at JPMC, 252(93%) had greater part of their labour conducted outside and only 48(17.6%) had their entire labour and delivery atJPMC (Table I).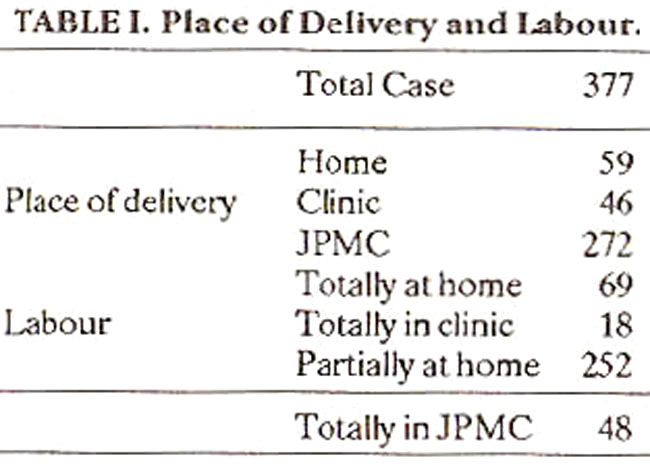
Different types of morbidity is shown in Table II.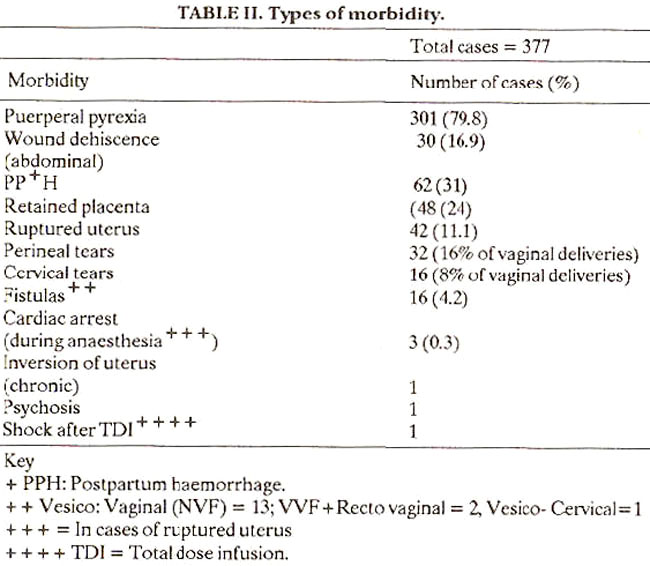
Pucrperal pyrexia was seen in 301 (79.8%) of 377 mothers, and 4.9% of total deliveries. It is possible that some more may have developed fever after being discharged as a large number are sent home after 24-36 hours and were therefore, not included in the study. Abdominal wound dehiscence requiring resuturing and or prolonged use of more than one antibiotic occurred in 30 (3.8%) cases of total abdominal deliveries. Most common infecting organisms were E.coli followed by Staph. aureus and Klebsiella11. Post partum haemorrhage (PPH) occurred in 62 cases, 29 amongst JPMC deliveries and 33 were admitted having delivered outside.
Injury to genitourinary tract included ruptured uterus, cervical and perineal tears (3rd degree) injury to rectal mucosa and bladder resulting in fistulae.
Sixteen cases of recent vesicovaginal fistula (VVF) were seen, 12 were admitted with the problem and 3 developed the complication in the hospital, 2 after emergency lower segment caesarean section (LSCS) for TABL11 II. Types of morbidily.
obstructed labour in nonbooked cases and 1 after forceps delivery following prolonged labour. Two cases of VVF referred from outside also had rectovaginal fistula (RVF). One case had vesicocervical fistula.
Forty-two cases of ruptured uterus were seen in 1 year, 37 were admitted with the problem and 5 sustained the injury in the hospital giving a rate of 1 in 1225 deliveries. Seven were dehiscence of previous LSCS scar and 33 were ruptures of unscarred uterus. Main cause of rupture was obstructed labour. Foetal mortality in complete rupture was 96.2% and in incomplete rupture 27.3%. One patient died giving a maternal mortality of 2.4%. Cardiac arrest during anaesthesia for laparotomy of suspected ruptured uterus was seen in 3 cases. All 3 were revived and did not suffer any permanent morbidity.
DISCUSSION
Maternal morbidity rate observed in this series is 4.4%, 377 patients developing intra and post-partum complications. This rate is the minimum morbidity rate as some cases of puerperal pyrexia and other complications may have been missed, being discharged before the development of the complication and may not necessarily come back to JPMC. Superficial wound dehiscence, often seen in the ward, were not included in the study.
Fortytwo cases of ruptured uterus were encountered in one year, 5 occurred within the hospital (1 in 1225 deliveries) which is higher than the reported incidence of 1 in 8649 to 1 in 2500 deliveries hut less than that reported from developing countries.12,16 Leading cause of rupture is obstructed labour (64%) mainly due to cephalopelvic disproportion. A careful obstetric history and careful systematic clinical pelvimetry is essential to confirm the presence or absence of this condition. Careful monitoring in labour and timely intervention is necessary before any damage to the mother or foetus occurs.
Puerperal pyrexia is more common after caesarean section (Table II). E. coli frequently present in obstetrical8-9 infection was isolated from 47,5% of cases11, indicating possible cross infection. This can be prevented by strictly observing labour room and theater discipline.
Main cause of morbidity from this study appears to be lack of prenatal care as 86% of mothers did not attend any antenatal clinic regularly. Other possible causes could be poor intranatal supervision and late referral to the hospital, 93% being brought to JPMC very late in labour when the complication had already occurred or was unavoidable (Table I). This is due to inability on the part of the birth attendant to recognize the problem in time and/or reluctance of the patient to seek hospital admission.
The extent and severity of obstetric morbidity among mothers can be reduced if all pregnant women have proper prenatal care and all births are assisted by a properly trained attendant.
REFERENCES
1. Measuring reproductive morbidity, report of a Technical working Group. Geneva. WHO, 1989. p.1.
2. Khan, H.A.M. Organization ofmaternal and child health services. JPMA., 1969; 19:517.
3. Rahimtoola, R.J., Saced, M. and Bhutta, T. Perinatal mortality. A three years study at Jinnab Postgraduate Medical Centre. Karachi. JPMA.. 1969; 19:136,
4. Jafarey, S.N. Review of maternal mortality over 10 years period at Jinnah Postgraduate Medical Centre, Karachi. JPMA., 1972: 22:71.
5. Women’s health and the midwife. A global perspective, report of a collaborative pre-congress workshop. Geneva, WHO, 1987, p.4.
6. Ahmad, Z... Maternal mortality in an obstetric unit. JPMA.. 1985; 35:243.
7. Kaunitz, A.M.M.. Hughes, 3M., Grimes, D.A., Smith, JCM., Rochar, R.W. and Kafrissen, ME. Causes of maternal mortality in the United States. Obstet. GynecoL. 1985; 65:605.
8. Clarke, M., Clayton, D.G., Mason, ES. and MacVicar, J. Asian mothers risk factors for perinatal death.the same or different ? A 10 year review of Leicestershire perinatal deaths. Br. Med. 3., 1988; 297:384.
9. Grant, J.P. Maternal deaths: Statistics of Shame. The state of The Worlds Children. (UNICEF), 1989, p.42.
10. Darts. K.K.. Sharnia, R.S., Razack. P.M.A., et al. Morbidity pattern amongst rural pregnant women in Alwar, Rajasthan- A cohort study. Health and population-perspee. Live and issues, 1980,3:282.
11. Baqai, R., Hasan, T.J. and Jafarey, S. Bacteriological study of genital tract infection in puerperium. JPMA., 1989; 39:70.
12. Falihallah, N.S., Al.Chalabi, H.A. and Al-Dahhan, F.H. Rupture of pregnant uterus. MJBU., 1988; 7:41.
13. Boulle, P. and Crighton, D. Rupture of unsearred uterus. Lancer, 1964; 1:360.
14. Palerme, G.R. and Friedman, E.A. Rupture of the gravid uterus in the third trimester. Am. .1. Obstet. Gynecol., 1966; 94:571.
15. Jafarey, SN. Rupture of ulerus. J PMA., 1973; 23:219.
16. Heij. HA., TeVelde, ER. and Cairms. 3M. The treatment of rupture of the pregnant uterus. Analysis of 93 cases treated in a rural hospital in 2.ambia. Int. 3. Gynaecol. Obstet., 1984; 22:215.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: