
Razia Korejo ( Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. )
Sadiqua N. Jafarey ( Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. )
July 1991, Volume 41, Issue 7
Original Article
ABSTRACT
During the one year period from 1st January to 13 1st December, 1989, therewere6,826 deliveries and 695 perinatal deaths, of these 553 were still-born and 142 were neonatal deaths (died within 7 days of birth). The perinatal mortality rate was 101.8 per thousand total births. The still-birth rate was 81 per thousand total births. Of the perinatal deaths, 7.9% occurred in booked and 92.1% in non-booked cases. The commonest cause of death was antepartum haemorrhage (APH), 24.2% followed by mechanical which accounted for 23.6% deaths. Abruptio placentae was the leading cause among all still-births and low-birth weight (LBW) in all neonatal deaths. (JPMA 41:151, 1991).
INTRODUCTION
Perinatal mortality (PNM) is defined as stillbirths and neonatal deaths in the first 7 days of life. In Pakistan, as in any developing country, it is high. The magnitude and causes of it however are not clearly defined. Some figures, both national and hospital based, are available for maternal mortality and infant mortality1 but very few figures are available for perinatal mortality. In this paper the extent and causes of PNM in a large Government teaching hospital are being reported.
SUBJECT AND METHODS
The Department of Obstetrics and Gynaecology of Jinnah Postgraduate Medical Centre has officially 135 beds but most of the times 170- 180 patients are present in the wards. Annual admissions are over 10,000 and approximately 7,000 deliveries take place every year. Obstetric admissions include 40% booked cases and the rest are referred from other hospitals, clinics, private practitioners, dais, or are self referred (60%). The criteria of booking taken for this study was a minimum antenatal attendance of three. Some patients may have travelled from the interior of Sindh and Balochistan distances varying from 50 to 500 Km and these are with most serious problems and complications. A special proforma was filled up for all stillbirths weighing 1000 grams or more and all infants of 1000 grams or above dying in hospital either in the obstetric ward or in the neonatal nursery within the first 7 days of life (early neonatal deaths). The maternal data included age, parity, period of gestation, previous obstetric history, complications in present pregnancy. Infant data included weight, sex, Apgar score at birth, age at death (in NND) and the cause of death. The cause was based on clinical data available. Autopsy was not carried out in any case.
RESULTS
During the one year period 1st January to 31st December, 1989, there were 6,826 deliveries and 695 perinatal deaths. 553 were stillborn and 142 died within 7 days of birth. The PNM rate was 101.8 per 1000 total births and still-birth rate 81 per 1000 total births. 7.9% of the deaths occurred in booked patients and 92.1% in non booked patients (Table-I).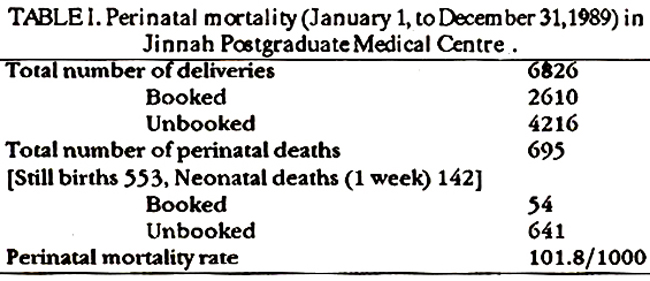
The age and parity of mothers in whom perinatal deaths occurred is shown in Table-II.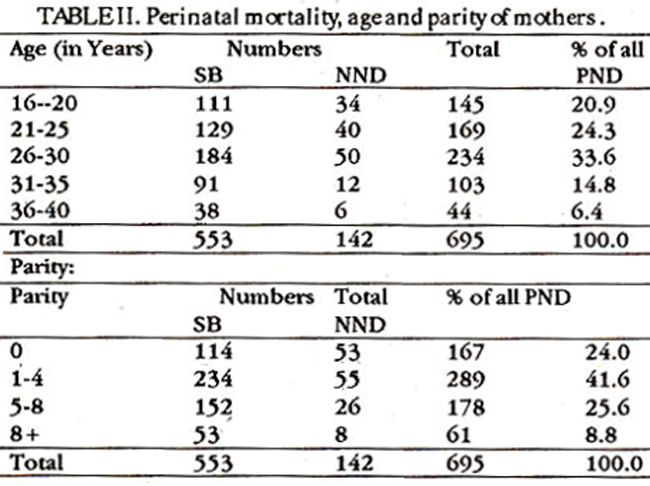
24.0% of deaths occurred in prinugravida, 289(41.6%) in para 1-4 and 239 (34.4%) in para 5 and above. The duration of pregnancy in 337 (48.5%) of the patients was less than 36 weeks and in the rest was 36 weeks or more (Table-III).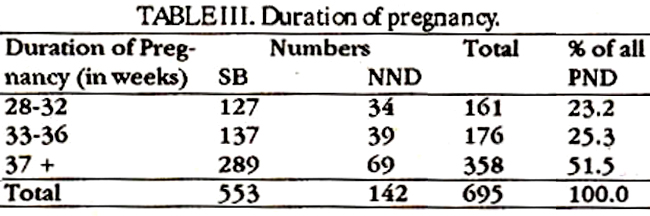
The weight distribution of the babies is shown in Table-IV.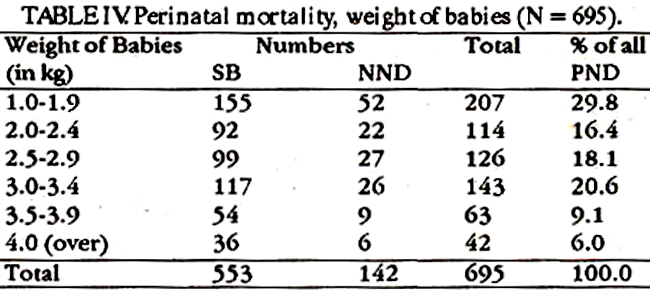
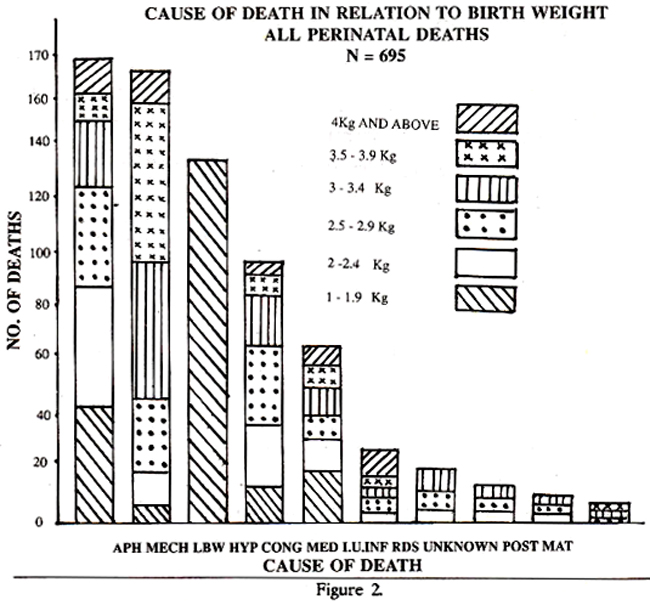
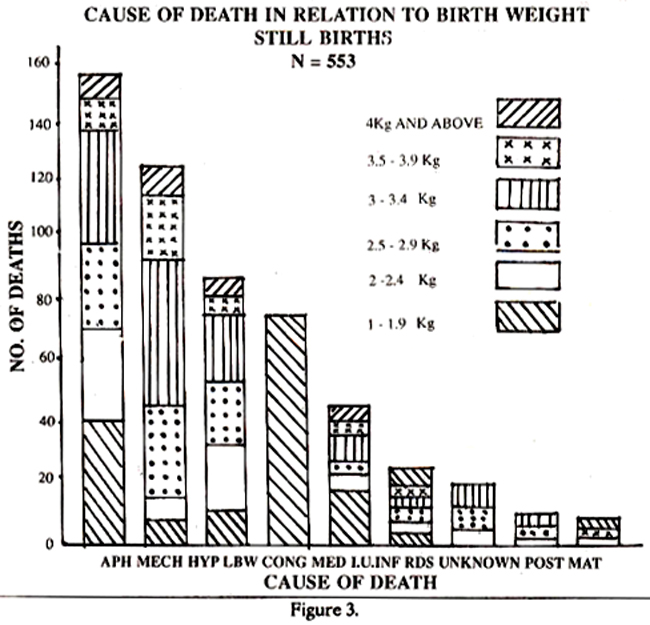
321 (46.2%) of the babies weighed less than 2.5 Kg, 269 (38.7%) weighed between 2.5 to 3.4 Kg, and 105 (15.1%), 3.5 Kg and above. 90 of the big babies in the last group were still-born mainly as a result of mechanical causes. The commonest (24.2%) cause of death was antepartum haemorrhage accounting for 168 deaths (161 still births and 7 NNDs). Of these abruptio placentae was responsible for 138 (19.9%), 134 being still-born thus constituting the single most common cause of still-birth (Table-V).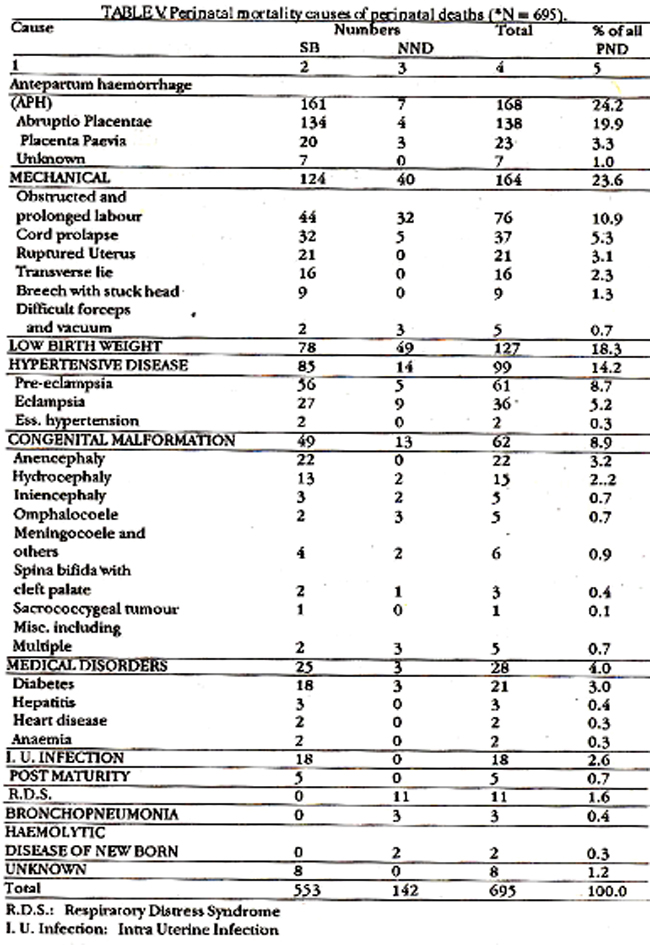
The next common cause was mechanical which accounted for 23.6% deaths. This group included patients with obstructed labour, ruptured uterus, difficult deliveries, cord accidents etc. Intrauterine anoxia and birth trauma were responsible for these deaths. In 127 (18.3%) cases low birth weight (LBW) per se caused perinatal deaths. Of these 78 were still-born and 49 NNDs. Babies with LBW where there were other obvious causes like abruptio placentae, hypertension etc., were not included in this group. LBW was the leading cause of death in NNDs. 99 (14.2%) of the deaths were due to hypertensive disease of the mother. This included pre-eclampsia (PE), eclampsia and hypertension due to other causes. Over one third of these deaths were seen in eclamptic patients, all non-booked. Of congenital malformations which caused deaths in 62 (8.9%) cases the commonest malformations seen were anencephaly (22) and hydrocephaly (15). The others are shown in Table-Vi.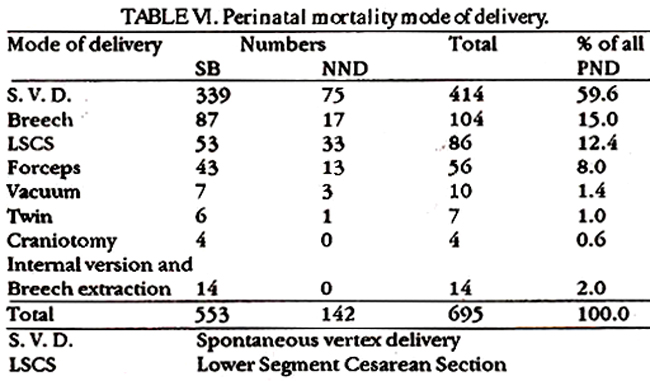
Medical disorders of the mother were responsible for 28 deaths, of which 25 were still-born. Diabetes meffitus was found in 18 cases and these patients were admitted with intra-uterine death of the foetus or uncontrolled diabetes. Intra-uterine infection of the foetus caused stillbirths in 18 cases whereas 11 NND occurred due to respiratory distress syndrome (RDS). The other causes of MMD were bronchopneumonia (3), haemolytic disease of newborn (NB) 2. In 8 cases of still-births the cause could not be determined. The total perinatal deaths, and still-births and neonatal deaths separately have been analysed according to the birth weight and cause of death and this is shown in Figures 1,2, and 3.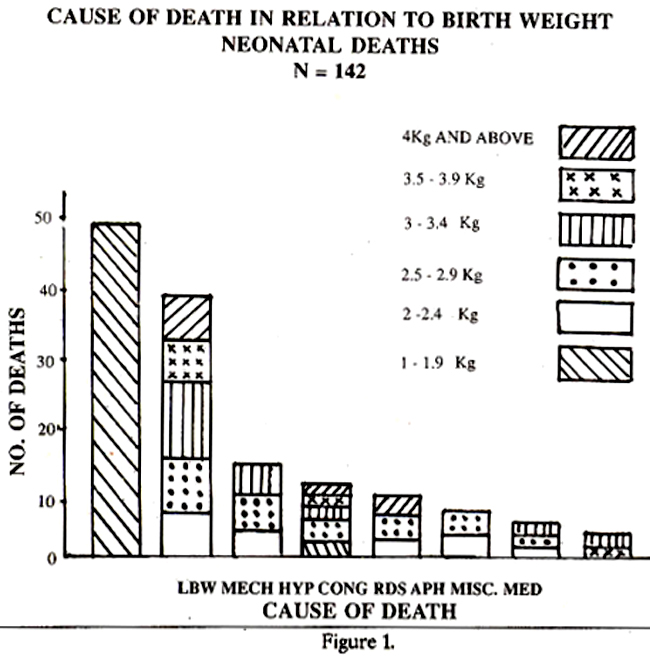
The mode of delivery is shown in Table-fl The incidence of abnormal delivery is high (40.4%). Fifty-three Caesarean sections had to be performed on foetuses already dead because of obstructed labour, placenta praevia, inefficient uterine action as a result of infection, cervical stenosis etc. Craniotomy was performed in 4 cases and internal version and breech extraction in 14. These were admitted with intra-uterine death.
DISCUSSION
The perinatal mortality rate of 101.8/1000 total births is very high. Even then it is not the actual rate as some of those babies that are discharged from hospital within 7 days of birth may die at home and are not included. Our figures, however, are hospital based - a hospital which deals with a large number of highly complicated cases and where even the ‘booked’ cases may not have had adequate care as the booking criteria of three attendances only is not ideal. These rates therefore should not be extrapolated for the community or the nation. From our experience of a community study in Mahmudabad the pen-natal mortality was 74. 7/1000 live births (Unpublished data). These figures should also not be compared with those of England and Wales, or of Denmark, Switzerland and Sweden as these are population based. In our study babies weighing 1000 grams or above only were included as smaller babies were considered unsalvageable. In a large number of cases multiple factors contributed to the death and it was difficult to assign a single cause. Attempts have however been made to put them under a single category. Abruptio placentae was the commonest cause of still-births and 50% of these babies weighed 2.5 Kg and above. Abruption is an important cause of perinatal mortality and morbidity in the developing countries and even in the U.S.A. 15% of deaths occurred due to abruption. In the low socioeconomic group of patients maternal malnutrition resulting in under perfusion of the placental site is said to increase the risk of abruptio2. Death of the big babies was due to difficult labour, ruptured uterus etc. About 90% weighed 2.5 Kg and above, and almost 30% were 3.5 Kg and over. These deaths are indicative of the lack or inadequacy of antenatal and intranatal care. LBW was the commonest cause of neonatal deaths (NND). 46.2% of all perinatal death weighed less than 2.5 Kg. As mentioned earlier it could not be ascertained whether these babies were premature or growth retarded. The mean birth weight of new borns in our department is 2.9 Kg. Congenital malformation (CM) has become an important cause of death in the developed world as other causes are being eliminated and is now responsible for more than 20% of deaths3. In our study only 8.9% had CM the most common being anencephaly. Though all CM were obviously not incompatible with life it is possible that other malformations existed which were not diagnosed as no postmortem was carried out. The high PNM rate shown here is to some extent an index of the inadequacy of maternity services of our country. It is however an overall reflection of the socioeconomic status and cultural pattern of the population. A malnourished community which is reluctant to seek medical advice during pregnancy and labour and refuses to limit the family is a high risk population in whom both maternal and perinatal morbidity and mortality are bound to be high. Chamberlain has aptly said that each country has different nutritional and morphological characteristics and PNM rates vary accordingly. The high mortality rates may not change completely even if the environment changes as the past medical history, childhood nutrition, and the education acquired in life play an important role. A comparative study among women delivering in England and Wales but born in Pakistan, India and the U.K. showed that whilst the U.K. and Indian group had similar PNM rate (9.9 and 11.2 per thousand total births respectively) the Pakistani population had a PNM rate of 18.8, the most vulnerable being babies below 2500 grams. Pakistanis, it is believed, perpetuate their dietary and social customs and do not change4. In order to reduce our PNM what is required is an overall improvement in the socioeconomic status of our population with better nourishment, better availability of social needs like education, change in cultural pattern and of course health awareness and availability of good maternal and neonatal services.
REFERENCES
1. Rahimtoola, R.J. and Qureshi, F. Perinatal mortality. Rawal Med.J., 1979;8:57
2. Golditch, l.M. and Boyce, N. E.Jr. Management of abruptio placentae. JAMA., 1970;212:288.
3. World Health Organization. Detennining the causes of perinatal death. Geneva WHO., 1984, p.1.
4. Chamberlain, GyP. Vital statistics for obstetricians, in Dewhurst\'s textbook ot obstetrics and gynaecology for postgraduates. 4th ed. Oxford, Blackwell, 1986, p 519.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: