
Mohammad Z. Tahir ( Department of cardiology and Endocrinology, Al Hada Military Hospital, P.O. Box 1347, HHRC 698, Taif, Saudi Arabia. )
October 1992, Volume 42, Issue 10
Case Reports
INTRODUCTION
Cardiac manifestations of hypothyroidism are pericardial effusion, increased left ventricular dimension with left ventricular dysfunction, wall motion abnormality, asymmetric septal hypertrophy and mitral valve prolapse. Pericardial effusion occurs in 30-37% of cases and is mild to moderate but is occasionally large and cardiac tamponade is rare1. We describe a case of hypothyroidism secondary to Sheehan’s syndrome who presented with signs and symptoms of cardiac tamponade.
CASE REPORT
A 58 years old Saudi female was admitted in emergency with 3-4 days history of malaise, vomiting and anorexia. She had significant post partum haemorrhage 249 30 years ago and since then she was amenorrhoeic and had weight loss, anorexia, weakness, cold intolerance, constipation and breast atrophy. There was no past history of tuberculosis, headache or visual impairment. Physical examination revealed thin, cachectic, weak and lethargic female with dry, cold skin and absent pubic and axillary hair. Her blood pressure was 54/38 mmHg, pulse 85/mm regular but weak. Pulsus paraduxus could not be appreciated and she was afebrile. There was jugular venous distension even at 900, with low volume carotid upstroke, no carotid bruit, no lymphadenopathy, no visual defect. Her mouth and throat were clear. Cardiovascular examination showed absent apex beat with distant heart sound and no pedal oedema. Both breasts were small in size. Abdominal examination was unremarkable. The reflexes showed slow relaxation phase with decreased muscle power but normal tone.
INVESTIGATIONS
On admission her white cell count was 8,500/mm3, haemoglobin 11.5 G/dl; MCV 87; HCT 35; ESR 75, electrolytes Na 136, K 3.7 HCO3 24, Cl 97, Bun 3.8, creatinine 86mg. X-ray chest showed mild cardiomegaly, no pulmonary congestion (Figure 1).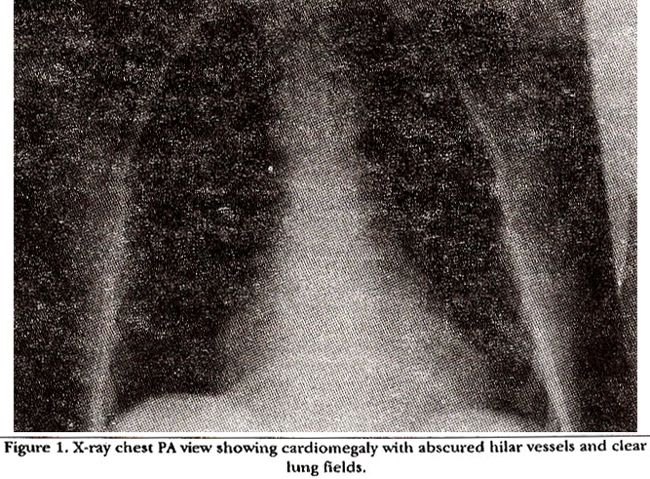
EKG showed low voltage in limb leads with diffuse non-specific ST-T changes, occasional ventricular ectopics, HR 100/mm. No electrical altemans seen (Figure 2).
mode echocardiogram showed diastolic notching of right ventricle and two dimensional echocardiogram showed diastolic collapse of right atrium and right ventricle. Echo, clinical features and BP 54/38 mmHg suggested cardiac tamponade. Pericardiocentesis was done and 205 ml of yellowish straw coloured fluid was aspirated which had a glucose of 5.7 mmol/L, LDH of 125 IU and serum LDH of 325 IU. Fluid to serum LDH ratio was 0.38:1. Protein in fluid was 40 mg/dl and in serum 76 mg/dl. Fluid was negative for AFB, bacterial growth and for viral neutralizing antibodies. Serum was PPD was negative. Thyroid function test showed a pericardiocentesis, BP came up to 100/70 mmHg, with pulse rate of 70/mm and on EKG there was some increase in voltage in chest leads (Figure 3).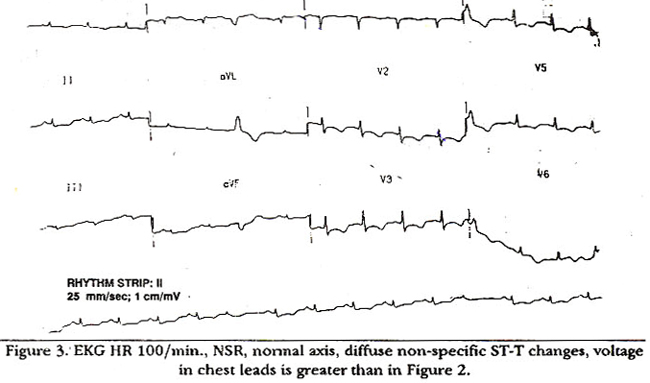
pericardiocentesis Post, x-ray chest showed normal heart size without any pulmonary congestion (Figure 4).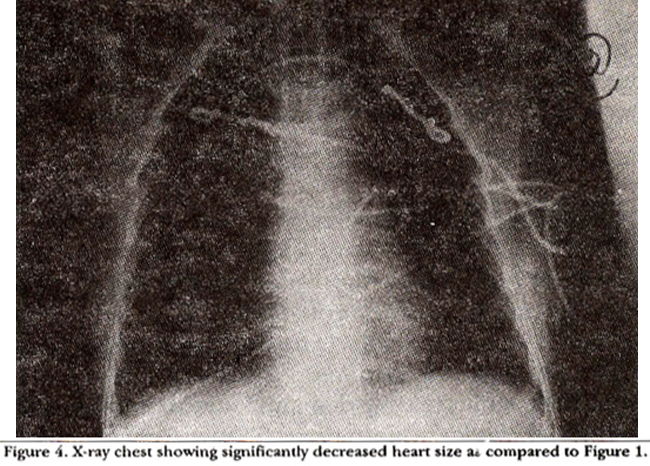
low T3 of 1.9; pmol/L (normal 4-8), T4 1.6 pmol/L (10-25), TSH 1.77 IU/L (normal 0.15-3.20). TSH was not elevated. Her LH was 1.6 JU/L (normal 30-150) arid FSH 6 IU/L (normal 27-113), both were low for a woman in the post menopausal age. Serum prolactin level was also low {39 in IU/L (normal 41-613)}. Cortisone stimulation test using synthetic ACT H 250 Ugms. IV was done. Baseline serum cortisol level was 108 nmol/L. 30 minutes after IV ACT H, serum cortisol level was 157 nmol/L and after 60 minutes it was 163 nmol/L, suggesting an insufficient response to ACT H stimulation test. X-ray lateral view of skull did not show any sella turcica abnormality. From above results, most likely diagnosis of Sheehan’s syndrome was made. To test the pituitary reserve, TRH stimulation test was done with 200 microgram W TRH. Baseline TSH level was 1.16 IU/L (normal 0.15-3.2) and prolactin level 110 IU/L (normal 41-613). After 30 and 60 minutes of injection the levels were 2.09 IU/L and 2.01 IU/L for TSH and 100 arid 76 IU/L for prolactin respectively. Both TSH and prolactin did not respond adequately to TRH stimulation. Patient was put on cortisone and thyroid supplementation and was discharged on tablet cortisone acetate 25 mg in morning and 12.5 mg in evening and L-thyroxine 50 microgram daily.
DISCUSSION
Hypothyroidism in elderly is asymptomatic and usually the diagnosis is made when patients present with pericardial effusion. Pericardial effusion in such patients is picked on routine examination with cardiomegaly on x-ray chest. Hemodynamically significant pericardial effusion is present with symptoms of hypotension. Pericardial effusion is attributed to an increased capillary permeability with protein extravasation, combination of sodium and water retention and slow lymphatic drainage3. Pericardial fluid is rich in protein and cholesterol. Pericardial fluid accumulates very slowly and may become large if remains undetected and asymptomatic. Pericardial tamponade has been reported but is a rare finding and can result into serious consequences4-7. Pericardial effusion resolves after several months of treatment for hypothyroidism. Other cardiac manifestations of mitral valve prolapse, asymmetric septal hypertrophy, LV dilatation and LV impairment resolve slowly with thyroxine replacement but regional wall motion abnormality remains unimproved2. Our patient presented to us when she was hemodynamically compromised. This fluid accumulation must be there for long time but it did not cause her symptoms 4nd she did not require medical advise. Pericardial fluid was rich in protein. Fluid cholesterol level could not be obtained. With thyroxine replacement therapy, she is not accumulating pericardial fluid any more. Pericardiocentesis is recommended in patients with cardiac tamponade as slow resolution of the pericardial fluid may lead to prolonged compromise when only medical therapy is used7.
REFERENCES
1. Kerber, R.F. and Sherman, B. Echocardiographic evaluation of pericardial effusion in myxoedema. Circulation, 1975;52:823-27.
2. Nouh, S.M., Famuyiwa, 0.0., Sulaimani, WA. and Nuaim, AR. The apectrum of echocardiographic abnormalities in hypothyroidism and the effect of hormonal treatment. Ann. Saudi Med., 1991;11:611.
3. Parving. H., Hansen, 3M., Nielsen, s.v., Rosaing, N., Munck, 0. and Lassen, NA. Mechanism of oedema formation in myxoedema- increased protein extravaaation and relatively slow lymphatic drainage. N.EngL3.Med., 301:460.
4. Smolar, RN., Rubin, J.E., Arramidea, A. and Career, AV. Cardiac tamponade in prinsaty myxoedema and reviewof the literature. Am.J. Med. Sd., 1976;272.345.
5. Kelly, 3K. and Butt, J.C. Fatal myxoedema pericarditia in a christian scientist. Am.J.Clin.Pathol., 1986:86:113.
6. Davis, PJ. and Jacobson, S. Myxoedems with cardiac tamponade and pericardial effusion of gold paint’ appearance. Arch. Intern. Med., 1967;120:615-19.
7. Daa, S., Liebennan, AN. and Sehusaler, G.C. Prolonged persistence of a large pericardial effusion and hemodynamicevidence of cardiac tamponade duringtreatment of myxoedema. Clin. Cardiol., 1982, 5:459-63.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: