
Mohd Aslam ( Division of Cardiothoracic Surgery, Department of General Surgery and Tuberculosis, Jawahar Lal Nehru Medical College, Aligarh Muslim University, Aligarh, U.P., India. )
Mujahid Beg ( Chest Diseases Unit of the Department of Medicine, Jawahar Lal Nehru Medical College, Aligarh Muslim University, Aligarh, U.P., India. )
June 1993, Volume 43, Issue 6
Original Article
Abstract
This study endeavours to evaluate the need for sedation in fibreaptic bronchoscopy and response of the patients when sedation is not used. One hundfed and five patients divided into three groups of 35 patients each, received buprenorphine (0.3 mg), diazepam (10 mg) and normal saline (0.5 ml) respectively alongwith atropine (0.6 mg) in each case The study emphasizes that sympathetic explanation of the details of the procedure to the patients, administration of careful topicd anaesthesia and avoidance of sedation makes the procedure acceptable, safe, comfortable with less complications and the need for admitting the patients to the ward is by and large avoided (JPMA 43:120, 1993).
Introduction
The invention of flexible fibreoptic bronchoscope1 improved the evaluation and management of patients with a variety of pulmonary disorders. Since general anaesthesia is not required flexible fibreoptic bronchoscopy can be easily performed in any clinical setting and is associated with a low complication rate2. Opinions differ on the premedication required and the need for general anaesthesia3. While there is universal agreement over the use of atropine as an anticholinergic agent there is neither uniformity of opinion regarding the choice of sedation nor any absolute rationale behind its use4,5. The purpose of this study was to evaluate the patients’ response to fibreoptic bronchoscopy with and without sedation and whether sedation is mandatory in all patients undergoing fibreoptic bronchoscopy.
Patients and Methods
This study comprised 105 consecutive diagnostic fibreoptic bronchoscopies in adult patients divided into 3 groups of 35 patients each. Detailed and sympathetic information regarding the procedure was given and a few likely associated discomforts like unpleasant taste of anaesthetic of the urge to cough and of the dysphonia which follow passing the fibreoptic bronchoscope through the glottis were explained.Awritten consentwas obtained from the patients undergoing the procedure. After 6-7 hours fast all patients were given 0.6mg of atropine intramuscularly 30-40 minutes prior to the bronchoscopy. The other injection was chosen from among the buprenorphine (0.3 mg), diazepam (10 mg) and normal saline (0.5 ml) administered intramuscularly alongwith atropine. 30-40 minutes after the premedication 2% lignocaine solution was sprayed into the nasal passages and pharynx with the help of hand atomiser. The dose oflignocaine was not allowed to exceed 400 mg in any case. Fibreoptic bronchoscopy was performed in supine position with flexible fibreoptic bronchoscope (model Olympus BF-3) via transnasal route. The tip of the fibreoptic bronchoscope was smeared with 2% lignocaine jelly and introduced through the patient’s nostril. Lignocaine solution 2% was instilled over the vocal cords and further 2 ml into the tracheawhichwas then entered. After examining the bronchial tree biopsies were taken from 72 cases before withdrawing the instrument. All the patients were questioned regarding the procedure and their responses were recorded.
Results
All 105 patients who underwent fibreoptic bronchoscopy were cooperative. Significant apprehension before bronchoscopy was shown by only two patients in atropine plus buprenorphine group. Majority of patients (91 patients) had no pre-procedural apprehension. During the procedure only 1 patient who had buprenorphine complained of discomfort. The addition of buprenorphine and diazepam in two groups of 35 patients each alongwith atropine added to the drowsiness which lasted for more than three hours in 31 and 28 patients respectively in the above mentioned groups (Table).
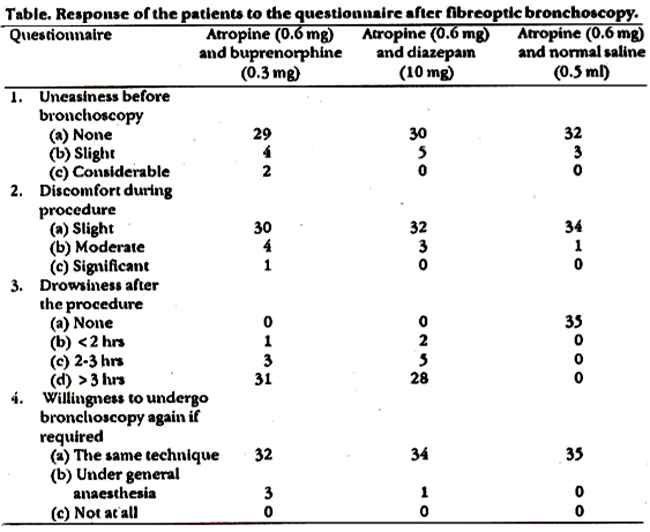
This necessitated to keep the patients fasting and extended the duration of hospital stay: However 35 patients in whom only atropine and normal saline was used as premedication, displayed excellent cooperation were at ease during the procedure, experienced no drowsiness after the procedure and were allowed to go home immediately. Two patients had hemoptysis and three slight epistaxis.
Discussion
Fibreoptic bronchoscopy has become a valuable tool in the early diagnosis of many pulmonary disorders. It has essentially replaced the rigid open tube bronchoscope in the diagnosis and management of inflammatory, infectious and malignant diseases of the chest6,7. To achieve best results the procedure should be made as comfortable as possible. Another objective to be fulfilled is to minimise the time of hospital stay and avoid loss of work days. The use of atropine as an anticholinergic agent helps reduce secretions in the pharynx and airways, prevents vasovagal phenomenon and minimizes cardiac dysrhythmias5,8,9. Different workers have used different sedative agents as an adjunct to atropine in order to relieve anxiety, alleviation of cough and to enhance cooperation during the procedure. However, the use of sedatives was associated with drowsiness and increased time of hospital stay of the patients. Rees et al9 used combination of diazepam or papaveratum with atropine and found that most patients were drowsy after the procedure. Similar observations have been documented by Dorward et al10. Pearce3 attempted to assess patients’ reaction to bronchoscopy without sedation or in a few cases with very mild sedation using benzocaine lozenges or intramuscular diazepam. His evaluation suggested that without sedation fibreoptic bronchoscopy remained quite acceptable to the patients. In our series all patients were sympathetically briefed about the procedure and all their queries replied and apprehensions removed. In two groups where buprenorphine or diazepam was used as a sedative agent, patients had more apprehension and unpleasantness as compared to the patients to whom no sedation was given. The patients without any sedation were more cheerful, experienced negligible discomfort, were allowed orally after the procedure and the hospital stay was minimized. Our study lays emphasis on the fact that the use of sedative agents as an adjunct to atropine has no significant role in carrying out fibreoptic bronchoscopy. The incidence of complications after fibreoptic bronchoscopy is low11 and is often related to sedation. We therefore, suggest that the use of sedation should be deferred in cases undergoing fibreoptic bronchoscopy unless special circumstances warrant it.
References
1. Ikeda, S., Yanai, N., Ishikawa, S. Flexible bronchofibrescape. Keio. J.Med., 1968;17:1-16.
2. Khan, MA., Whitcomb, ME.. Snider, G.E. Flexible libreoptic bronehoscopy. Am.J.Med., 1976;61:151-55.
3. Pearce, S.J. Fibreoptic bronchoscopy: Is sedation necessary? Br.MedJ., 1980;281:77980.
4. Shah, AC. Flexible fibreoptic bronchoscopy in pulmonary medicine. 3. Assoc. Physiciana, India, 1983;31:659-62.
5. Iseman, M.D. Flexible libreoptic bronehoscopy in: Pulmonary diagnostic techniques. PETT/TL ed. Philadelphia, Lea and Febiger, 1975.
6. Zavala, D.C. Flexible libreoptic bronchoacopy. A training hand boot Iowa City, University of Iowa, Deptt. of Publications, 1978.
7. Landa, J.F. indications for bronchoscopy. Chest, 1978;72 (Suppl):686-90.
8. Zavala, D.C., Godsey, K., Bedell, G.N. The response to atropine sulphate given by aerosol and intramuscular routes to patients undergoing fibreoptic bronchoscopy. Chest, 1981;79:512-15.
9. Rees, P3., Hay, 3.0., Webb, J.R. Premedication for fibreoptic bronchoscopy. Thorax, 1983;38:624-29.
10. Dorward, A.J., Berkin, ICE., Elliote, J.A., Stack, B.H.R. A double blind controlled study comparing tomazepam with papaveratum as premedication for libreoptic bronchoscopy. Br.J.Dis.Chest, 1983;77:60-65.
11. MacDonald, 3.B. Fibreoptic bronchoacopy today: a review of 255 cases. Br.Med.3., 1975;3:753-55.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: