
Zarina Khan ( Ultrasonic Clinic, 70-E, A.A. Plaza, Blue Area, Jinnah Avenue, Islamabad. )
November 1994, Volume 44, Issue 11
Original Article
Abstract
Hundred cases of preterm labour (before 36 weeks) with cervix 4cm or less dilated and’ preterm prelabour rupture of membranes (excluding cases of uterine over distension, maternal medical disorders and fetal congenital abnormalities) were treated with bed rest and sedation. Labour set in within 2-6 days with high fetal morbidity and mortality. Another fifty similar patients were given in addition to rest in hospital for 48 hours, 1000 ml of 5% dextrose in six hours, intravenous antibiotics (after sending off cultures from the vagina per speculum), cotricosteroids and a single dose of analgesia/sedation injection. In 85% painful contractions ceased and membranes stopped leaking until near term. In 10% painful contractions ceased, but leakage continued for 2-7 weeks, and the gain in intrauterine life led to 100% neonatal survival with short hospital stay in the neonates born after 31 weeks. Only 5 % failed to respond to treatment and after delivery these premature neonates developed pneumonia and septicaemia from the same organisms that were colonizing their maternal genital tract and had entered the fetus via the infected amniotic fluid. It is recommended that all patients in preterm labour or preterm prelabour rupture of membranes (excluding over distension) be given besides bed rest and sedation, corticosteroids and antibiotics intravenously for 48 hours and then orally for eight more days. Tocolytics are not recommended. This regime saves babies (JPMA 44:258,1994).
Introduction
Preterm labour or spontaneous preterm prelabour rupture of membranes with the pregnancy less than 36 weeks, if left to nature causes high perinatal mortality inspite of long and expensive intensive hospital care. About 6-15% of pregnancies end up in preterm labour1 or rapture of membranes with the inevitable dangers to the fetus of being born too soon. These premature babies develop respiratory distress syndmme due to poor lung expansion caused by low surfactant (lecithin/sphingomyclin ratio), which increases in the lungs as pregnancy matures. These neonates cannot suck or swallow pmperly and choke easily. They have an increased incidence of periventricular brain hemorrhage and later develop physical and mental handicaps. In order to overcome all these complications intensive care by highly trained neonatologists with sophisticated equipment becomes necessary but is very expensive. There is therefore, no better incubator than the mother’s womb. Every effort should be made to keep the fetus inutem as long as possible. Until a few years ago preterm labour (before 36 weeks) or preterm prelabour rapture of membranes was a sure indication of impending psychological, emotional and economic disaster for the parents, obstetrician and paediatrician alike. Bed rest in a noisy hospital with an occasional injection of Pethidine for pain relief or sedation was all that was available. Tocolytics like Ventolin or Ritodrine were sometimes, used causing unacceptable side effects in the mother and her baby with labour postponed for 2 or 3 days. Recently infections in the vagina have been implicated, by spreading to the membranes with release of prostaglandins and other inflammatory products, resulting into preterm labour and preterm prelabour rapture of membranes. In more severe cases amnionitis may result in maternal signs as fever and tachycardia and foul. smelling purulent liquor amnii. In order to test the hypothesis hundred case records of preterm labour and pretermprelabour rupture of membranes were collected retrospectively dating before July 1992. From then onwards management policy, of such patients was changed by admission to hospital for 48 hours with bed rest, running ina5%Dextrose drip, sending off vaginal cultures before starting intravenous antibiotics for 48 hours which was followed on by oral antibiotics for another eight days at home (onbed rest). Moreover, Corticosteroids in large doses were given intravenously to the mother quickly to suppress infection, to help in earlier maturation of the fetal lungs and to decrease the incidence of intracranial hemorrhage. The latter need 24 hours to work and if labour is inevitable within a few hours their use would be superfluous as they cannot benefit the fetus. A comparison of 50 patients actively treated in the current manner with a hundred conservatively treated is presented. The Ultrasonic Clinic where this study was carried out is a small private hospital in the center of Islamabad. Ninety percent of the mothers were educated and follow-up was therefore possible for six weeks postnatal.
Patients and Methods
From January, 1988 to July, 1992, hundred patients in premature labour (before 36 weeks gestation), with cervix 4 cm dilated along with spontaneous rapture of membranes without labour pains (excluding those with Over distension, medical disorders or fetal congenital abnormalities), were treated as was then the policy by prolonged bed rest to decrease the pressure on the cervix which is supposed to cause diminished uterine contractions. The recumbent position also prevents liquor from draining out quickly and causing more tonic contractions. Vaginal examination was not done if labour pains were absent to avoid introducing infection into the cervix. Ventol in was titrated in a 5% Dextrose drip in 20 patients only, in early labour, and Inj. Promethazine (Phenergan) 25 mg was given intravenously to calm the patient. From August,1992 onwards in the next fifty patients who although were similarly selected and admitted for bed rest for 48 hours and had administration of Inj. Pentazocinef Promethazine (Phenergan) 25 mg intravenously and collection of cultures from the lower vagina via a sterile speculum. Further management was altered to combat infection and to enhance foetal lung maturity. Thus a 5% Dextrose drip was run rapidly over 4 hours to dilute the circulating Prostaglandins/oxytocin, withholding Tocolytics like Ventolinor Ritodrine. Antibiotic coverwas givenwithout waiting for the culture report, intravenously for48 hours and there after orally for another eight days. The type of antibiotics were initially selected and altered in 48 hours if necessary, on the basis of the sensitivity reports of majority of the pathological organisms found in the vagina in gynae patients, keeping in mind the presence and duration of pregnancy. The organisms grown and their sensitivity was determined. Metronidazole intravenous Infusion was given twice daily for 48 hours, then continued orally 400 mg twice daily for eight days to cover anaerobes and bacteroides, along with a first generation Cephalosporin (Ceporan) 500 mg 8 hourly for 48 hours intravenously and then in the same dose orally for next eight days to cover other non specific infections. Corticosteroids were given to help lung maturation and suppress infection thereby reducing neonatal mortality and expensive hospital stay in the form of Inj. Hydrocortisone 500 mg I.V. for four doses at 12 hourly interval (total 2g)or Dexamethasone 12mg I.M. in two doses 24 hours apart. A single weekly injection was repeated if membranes continued to leak or labour threatened to set in. It was not given if the cervix was more than 5 cm dilated, or if the liquor amnii was foul smelling or purulent.
Results
The conservative management of hundred patients in preterm labour and prelabour preterm rupture of membranes with bed rest and sedation alone resulted inagainof2 to 6 days only, before laboursetin. Of the 20 patients given Ventolintwo fetuses had cardiac arrest in utero (at 29 and 31 weeks). The use of this drug was then discontinued. Only 89% of babies over34weeks survived and were sent home on breast milk. All those under 30 weeks shifted to large hospitals with intensive care units in Islamabad but all died of pneumonia, respiratory distress syndrome or septicaemia. The babies born prematurely after expectant treatment were limp, less active, with weak ciying and sucking reflexes. The result of conservative management are summed up in Table I.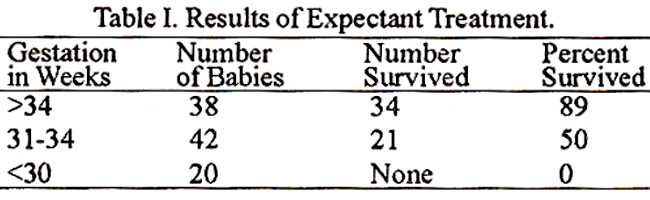
Out of 42 babies of this group born between 31-34 weeks only 21(50%) survived. Of the 38 babies of more than 34 weeks gestation, 34 (89%) survived, while all babies less than 30 weeks died of pneumonia/septicaemia. The babies of fifty patients given active treatment were more alert, active, crying loudly and sucking better. Their mothers on admission, after receiving antibiotics and corticoids, 42 (85%) stopped leaking liquor and their painful contractions subsided completely and they delivered normally near term. Five mothers (10%) stopped contracting for 3-5 weeks, but continued to drain liquor amnii and the neonates, even those of 2000g did not develop respiratory problems and were successfully tube fed until sucking reflex developed. For them the incubator was required for 4-10 days and they went home by 5 to 15 days on breast milk. Only three patients did not respond and the fetus was expelled within 3-5 days. Their vaginal cultures showed a heavy growth of Klebsiella, Proteus or Pseudomonas that were not sensitive to the antibiotics given. Neonatal loss was due to pneumoma/septicaemia from these organisms. The results of active management are summed up in Table II.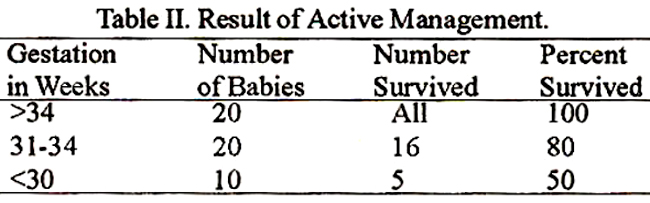
All of the 20 babies of more than 34 weeks gestation survived. Out of 20 babies between 31-34 weeks gestation 16(80%) survived. While 5 out of 10 babies less than 30 weeks gestation (50%) survived. The sensitivities of the colonizingbacteriaof5O patients given active management are shown in Table III.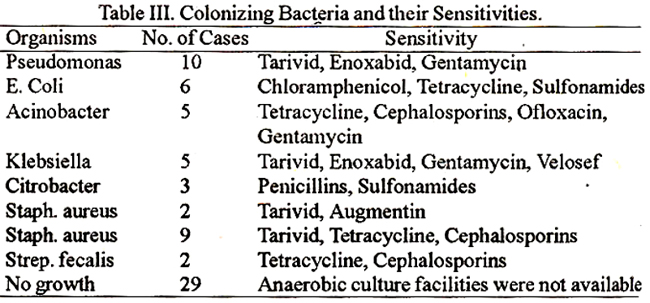
Discussion
A premature baby is a catastrophe, emotionally for the parents, psychologically for the obstetrician, economically for the nation and a time consuming challenge for the pediatrician. A baby weighing less than 1500Gm in intensive care needs Rs. 30,000 worth of pediatrician/nursing time along with sophisticated equipment. Untila few years ago no cause could be pinpointed for the onset of premature labour and preterm prelabour rupture of membranes except over distention, severe urinary tract infection, diarrhoea or severe physical and mental shocks. Hormonal imbalance or cervical incompetence was a possibility. Now genital tract colonization by pathogenic bacteria followed by membrane rupture is considered a very important cause of preterm labour and preterm rupture of membranes preceded by amnionitis and placentitis and if decidual tissue is involved systemic signs of inflammation can occur in the mother. It is postulated that bacterial endotoxins may increase prostaglandins in the uterus. Clinical signs of maternal fever and fetal tachycardia may be evident. In a controlled trial by Makepeace2 from Liverpool in 1992, organisms were cultured from the cervix and vagina in all 105 cases of preterm prelabour rupture of membranes prior to 34 weeks gestation, but in 105 controls at term only 25% grew pathological organisms. Another study by Celine3, proved that there was an increased incidence of bacterial colonization and membrane rupture in premature labour as compared to controls at term with intact membranes. Since bacteria can initiate preterm labour and prelabour rupture of membranes the right antibiotics should be the first line of defence. As prostaglandins were thought to be released, prostaglandin synthetase in hibitor4 e.g., Indomethacin was used to remove the same, but when used for more than 72 hours it can cause oligohydramnios, premature closure of ductus arteriosus, pulmonary hypertension and bleeding disorders in the fetus. Karim5 conducted a controlled trial of antibiotics and corticosteroids in preterm labour between 26-34 weeks and noticed a prolongation of pregnancy by 15 days and drop in neonatal morbidity to 23%, when the control group delivered in 2.5 days and the neonatal morbidity was raised to 40%. According to him, coiticoids in preterm labour benefit in many ways. There is a five-fold reduction in neonatal mortality, a reduction in duration of stay and hospital care of neonates, decrease in respiratory distress syndrome by 40-60% by increase in surfactant, decrease in periventricular haemorrhages and diminished necrotizing enterocolitis. Our study also proves that antibiotics and corticoids given early6, save babies. In our study babies born before 34 weeks on expectant treatment, 89% survived, but with active treatment 100% survived. Of the babies born between 31-34 weeks on expectant treatment only, 50% survived, but on active management 80% survived. Similarly babies born at less than 30 weeks gestation with expectant treatment none survived, but with active treatment 50% survived. It is therefore recormnended that potential mothers and fathers with previous abortions, preterm labour and preterrn prelabourrupture of membranes be screened before pregnancy for genital colonization. If pathogenic organisms are found, the patient and partner should be treated with the antibiotic to which the organisms are sensitive prior to embarking on a new pregnancy. If seen for the first time these patients with pretenn labour or preterm pre labour rupture of membranes should be actively treated with the above regime to gain more intrauterine life and hence achieve a more mature neonate who can survive without intensive care. Tetracycline and Quinolones are not recommended in pregnancy. Sulfonamides are to be avoided in last two months as they may cause jaundice in the neonate, leaving the choice of Cephalosporins and Augmenlin. Metronidazole should be used to cover anaerobes and Bactcroides.
References
1. Body, W, Kalehan, P. Natural hiatozy of preterm prelabour spontaneous rupture ofmembranes (Abstract). 2dthBritish Congress of Obstetrics and Gynaecology, Manchester, 7-10 July, 1992, p.2.
2. Makepeace, P. A. and Ramsdcn, 0. Role of bacterial colonization in preterm premature rupture ofmcmbranes (Abstract). British Congress of Obstetric and Gynaecology, Manchester, 7-10 July, 1992, p.404.
3. Celine, 0. and Knox, R. Infection and the pretcrm premsture rupture of membranes. British Congress ofObstetrics and Gynaecology, Manchester, 7-10 July, 1992, p. 170.
4. Murray, H. G. Fetal pleural effusion following matemal indomethacine therapy. Br. J. Obstet. Gynaecol., 1993;100:277.
5. Ksrim, N. and Pattison, R. A prcterm labour management randomized controlled trial investigating antibiotic intervention on a multicentre basis. (Abstrct) 26th British Congress of Obstetrics and Gynaeeology, Manchester, 7-10 July, 1992:p.3.
6. Briggs, 0. 0. eds. A reference guide to Fetal and Neonatal Risk: Drugs in Pregnancy and Lactation. 2nd ed., Baltimore, London, Sydney, William and Wilkins, 1986, pp. 292-93.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: