
Mohammad Iqbal ( Department of Orthopaedic Surgery, Bloan Medical College, Quetta. )
Habib-ur-Rehman ( Department of Orthopaedic Surgery, Bloan Medical College, Quetta. )
June 1994, Volume 44, Issue 6
Original Article
Abstract
Vascular complications associated with supracondylar fracture of humerus are well recognised. Less well recognised are neurological injuries associated with this fracture. A prospective study was conducted to explore the role of open reduction and internal fixation of this fracture. The article presents the incidence of nerve lesions in 46 cases of supracondylar fracture of humerous; review of pertinent literature is also included (JPMA 44:148, 1994).
Introduction
Supracondylar fracture of the humerus are commonly accompanied by neurological complications due to closed proximity between radial, median and ulnar nerves, to the supracondylar region. The nerves are either contused or actually severed as a result of initial injury, or during injudicious repeated attempts at closed reduction1. Nerve deficit may also occur due to haemorrhage or as a result of vascular compromise2. This report presents the pattern of nerve injuries associated with supracondylar fracture of the humerus.
Patients and Methods
Forty-six cases of supracondylar fracture of humerus attended our hospital during the year 1988 to 1990. All patients were treated by different methods advocated in different situations. Neurovascular status of the involved extremity was assessed in all cases, at the time of initial examination and discharge from the hospital. All patients were reviewed after 6-18 months.
Results
A total of 46 patients of both sexes were studied. The age of patients ranged from 1.5 to 12 years. The maximum age group was between 7-9 years. The peak age for this injury was 6.5 years. Transient nerve palsies were encountered in five patients (10%). Three patients had radial and 2 median nerve involvement. No cases of ulnar or anterior interosseous nerves were seen in this series.
Discussion
Incidence of nerve injuries depends upon the type of fracture, extent of injury and the initial management3.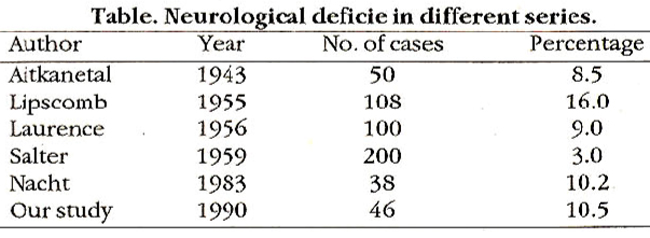
Table shows the frequency of nerve lesions reported in some of the previous series. Our findings are similar to those of Nacht4. Aitken et al5 reported four cases of nerve injury out of fifty cases. All these occurred as a result of markedly displaced fractures. In our series of forty-six cases nerve involvement occurred in five patients; in all these cases distal fragment was displaced posteriorly and angulated medially and four had open fracture. It is thus evident that postero-medial angulation and open fractures are most common causes of neurological deficit. Highest frequency (25%) of neurological complications as a result of initial injury and after reductionwas reported by spitzer6. Similar (20%) findings have also been reported by Kirz7. Nerve lesions were seen in 2.8% of 1,377 cases of supracondylar fracture of the humerus Hellinger’s Series8. Radial Nerve Injury is the most frequent5,9 followed by median nerve. Ulnar nerve involvement is seen occasionally and is more with flexion type of supracondylar fracture of the humerus3. Anterior interosseous nerve injury is rare. In this study 3 (6.5%) patients had radial nerve injury. There is a good anatomical explanation for the higher frequency of radial nerve injury. It occurs due to postero-medial displacement, the lateral spike of the proximal fragment protrudes laterally, the radial nerve is thus susceptible to be tented across this lateral spike whereas the lateral displacement of the distal fragment pulls the radial nerve away from the sharp edge of the proximal fragment3. In our patients with radial nerve paralysis, there was significant correlation between the radial nerve injury and postero-medial displacement of the distal fragment5. Median nerve injury is the second most common type and is caused by ischaemia2. Two (4%) patients in this study had median nerve involvement. In one, there was sensory and motor loss alongwith impending Volkman\\\'s ischaemia. Open reduction was done and after 5 weeks the sensations and power returned spontaneously. Spontaneous recovery points to ischaemia as cause of deficit in this patient2. Injury to median nerve also occurs as a result of postero-láteral displacement of the distal fragment which was not seen in this series. The second patient with median nerve deficit in this series also had branchial artery severed. Finding in this case correlates with cases reported by Liddel10. Ulnar nerve is rarely injured with extension type of supracondylar fractures. Fowles3 described one case of ulnar nerve, in his series of fifty cases. As observed by others2,11 also none of our cases had ulnar nerve injury. Lowincidence ofulnar nerve palsy could be explained on anatomical basis. In extension type of fracture ulnar nerve is relaxed and carried backward away from the sharp distal end of the proximal fragment. Therefore, it is rarely injured whereas in flexion type of supracondylar fracture the distal fragment carries the ulnar nerve along with it and the nerve may be sharply angulated and stretched over the fracture margin as this jets posteriorly3. None of our patients had fractures of extension type so we did not encounter ulnar nerve lesion. Anterior interosseous nerve palsy is a rare complication of supracondylar fracture of the humerus. Spinnar found six cases of arterior interosseous nerve palsies after a review of literature. None of our cases had anterior interosseous nerve paralysis. The low frequency could be because of the fact that the lesion is easily missed when the median nerve paralysis is also present. The observation reported in this study indicates that neurological complications are commonly encountered in this fracture, the deficit depends upon the severity of the trauma. A search for thorough sensory motor and vascular lesion must be made at the initial examination and the recovery is spontaneous. However, if along with pulselessness, pain, pallor and paralysis are also noted immediate exploration for artery and nerve is mendatory10.
References
1. Bristo, R.W. Myositisossificans and Volkmans Paralysis note on two cases. Br.J.Surg,1923; 10:475-82.
2. Leurence, W. Supracondylar fractures of the humerus in children: a review oflOOcases. Br.J.Surg., 1956;44:143-47.
3. Fowles, V.3. and Kassab, M.T. Displaced supracondylar fractures of the elbow in children. A report on the fixation of extension and flesxion fractures by two lateral percutaneous pins. J.Bone Joint5urg., 1974;56B:490-500..
4. Nacbt, L., Jeffrey, H., Ecker, L., et al. Supracondylsr fracture of the humerus in children treated by closed reduction and percutaneous pinning. clin.orthop., 1983;177:203-9.
5. Aitken, M., Mitchell, D.R.W., Smith, B.K. Supracondylar fracture in children. Am.J.Surg., 1943;59:161-71.
6. Spitxer, GA. and Peterson, CD. Acute nerve involvement in supracondylar fracture of humerus in children. J.B.J.S., 1973; 53-A:219-27.
7. Kin, H. Supracondylar fractures of the humerus in children. Orthop. Rev., 1981;10:85.
8. Hellinger, 3. Supracondylsrfrscture of the humerus. Ninth international symposium on topical problems in orthopaedicsurgery. Switzerland. 1979, pp.141-43.
9. Lipscomb, R.P. and Burleson, JR. Vascular and neural complications in supracondylar fractures of the humerus in children. J.BoneJoint Surg., 1955;37A:487-92.
10. Liddell, A.W.M. Neurovasculsr complications in widely displaced supracondylar fracture of the humerus. J.Bone Joint Surg., 1967;49B:805-6.
11. Gruber, A., Martin, 0. and Hudson, C. Supracondylar fracture of humerus in children. End results of open reduction. J.Bone Joint Surg., 1964 ;46A:1245-5 2.
12.Griffiths, D.L.L Themanagement of acute circulatory failure in an injured limb. J.Bone Joint Surg, 1948;30B:280-89.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: