
Zubair Ahmed Awan ( Department of Biochemistry, Army Medical College, Rawalpindi. )
Abdul Baseer ( Department of Biochemistry, Jinnah Postgraduate Medical Centre, Karachi. )
October 1995, Volume 45, Issue 10
Original Article
Abstract
Sera obtained from 42 patients of myocardial infarction, 28 of unstable angina and 25 healthy control subjects was assayed for total triglycerides, cholesterol, LDL cholesterol (LDL-C), HDL Cholesterol (HDL-C) and VLDL Cholesterol (VLDL-C). The level of cholesterol was also determined among the sub-fractions of HDL. The levels of total triglycerides, cholesterol, LDL-C and VLDL-C were significantly raised in both groups of patients. Total high density lipoprotein cholesterol was low in patients, which was highly significant in HDL2-C and not in HDL3-C. These results suggest that serum lipids are directly correlated with the severity of coronary heart disease (CHD). Total cholesterol when measured in major lipoprotein classes and further partitioned into sub fractions, increase their sensitivity, specificity and hence their predictive value as sensitive markers for the assessment of CHD risk (JPMA 45:263, 1995).
Introduction
Ischaemic heart disease develops due to a them sclerosis caused by accumulation of lipids, primarily cholesterol but also triglycerides, in the walls of coronary arteries which tend to narrow the lumen and decrease the blood flow1-3. The concentration of serum triglycerides is increased in patients of CHD4-8. The occurrence of elevated levels of serum cliolesterol in patients with CHD has been known over years6,9. Lipids are incorporated with lipoproteins for their transport. The incisive studies of lipoproteins for the last few years have contributed to significant advances in understanding and management of lipid disorders, in fact related to abnormalities in the metabolism of lipoproteins10-12. Clinically, the concentration of lipoproteins in the plasnm is assessed by quantifying the cholesterol moiety of lipoprotein particle, which are sensitive markers for the assessment of coronary artery disease (CAD) risk12-14. The concentration of HDL cholesterol especially HDL2 shows a strong inverse association with CHD12,15-18. The levels of LDL- cholesterol were consistently raised in patients with CHD as compared to controls in various studies21,18,19 Significant rise in VLDL cholesterol has been reported in CHD patients in some studies20. The present study was planned to evaluate the serum triglycerides as un variate risk factor for CHD. The changes occuring in different lipoprotcins cholesterol were also determined which are considered at present to be more sensitive means of assessing the persons at relative risk of developing ischaemic heart disease.
Patients and Methods
The patients of ischaemic heart disease ([HD) included in this study were either admitted or registered as out-door cases at National Institute of Cardiovascular Diseases (NICVD) Karachi. The clinical history was recorded with particular emphasis on age, sex, occupation, family history of IHD, smoking habits, blood pressure and weight. Patients with diabetes mellitus were excluded. The patients comprised of two groups:
a. Forty two patients with myocardial infarction, diagnosed on history, ECG changes and elevation of the cardiac enzymes, (AST, LDH and CPK). The interval between first attack and the time of taking the blood sample was one to two months.
b. Twenty-eight patients of unstable angina diagnosed on history, subjected to coronary angiography and found to have stenosis of coronar y arteries with different severity.
Control group comprised of healthy volunteers of similar age, sex and socioeconomic status. The information about their blood pressure, smoking habits, history of IHD in family was also recorded.
Blood sample (10-15 ml) was drawn from each patient and controlled after an overnight fast of 12 hours. Serum was separated and stored at -20°C till estimation. Samples were analysed for total triglycerides by the enzymatic colorimeteric method using kit supplied by Boehringer GmbH. Total cholestemi was determined by enzymatic method21 using the kit monotest cholesterol obtained from Boehringer GmbH. Total HDL cholesterol22 HDL3-cholesterol, HDL2-cholesterol23 were determined by different precipitation procedures. LDL-cholesterol and VLDL-cholesterol24 were estinmted by calculated formula.
Results
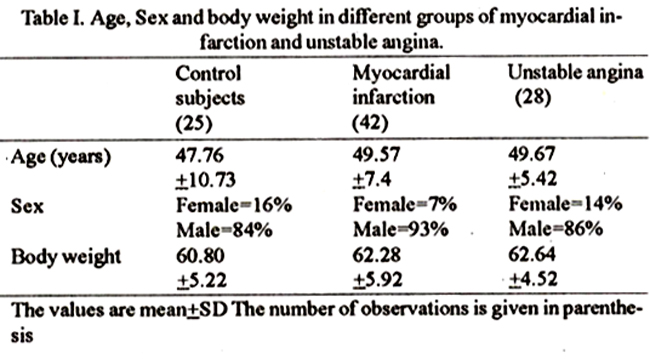
Table I shows that IHD is predominant among males and the body weight of the patients was not significantly higher than the controls. The patients of [HD had a significantly higher blood pressure as compared to controls and the percentage of smokers was more among patients than the controls (Table II).
The mean levels of total triglycerides, total cholesterol and different lipoproteins cholesterol for the patients and controls are given in Table III and IV.
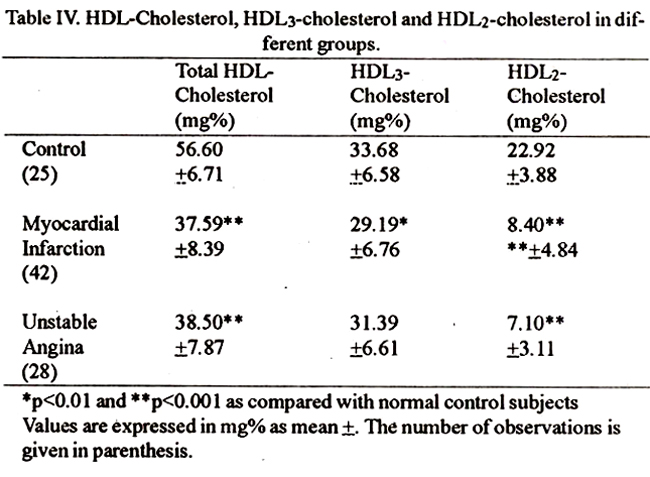
The values of triglycerides, total cholesteml, LDL-C and VLDL-C were significantly elevated in all patients as compared to controls (p<0.001). The values of total HDL-C were significantly low in patients as compared to controls (p<0.001), maximum decrease was in HDL2-C (p<0.001) in both patients of myocar dial infarction and unstable angina. HDL3-C was decreased in myocardial infarction (p<0.01) but not in unstable angina (Table IV).
Discussion
Epidenuological, clinical and animal experimental research has clearly demonstrated that increased serum lipid concentrations and abnormal lipoprotein metabolism are intimately involved in development of CHD12,13,25. Most of the studies demonstrate a univariate association of CHD with raised serum triglycerides4,5,26,27. Raised levels of total and HDL cholesterol along with modification of other risk factors have been reported in many studies27-30. In the present study, serum triglycerides was significantly raised in patients as compared to controls, which is in agreement with the previous data. Hypercholesterolemia in patients of CHD has been reported by many workers6,19,26,31 which was also found in this study. The increasing interest in detailed measurements of lipoproteins and their protein and lipid moities is based on experimental evidence linking the different fractions to specific functions, which may be important in the understanding and management of atherosclerosis of CHD. The serum LDL cholesterol and VLDL cholesterol were increased in all the çatients as compared to those reported by other workers20,31,32. The mean levels of total HDL-cholesterol in patient groups were significantl1 lower than the controls as shown by the previous workers12,15,33,34. This is useful for identifying patients at high risk of CHD. The strongest inverse relation was between the cholesterol concentration in HDL2 subfriction of HDL but not HDL3 in the patients of ischaemic heart disease. This observationis consistent with the reports of other workers13,18,35-38. The present study has demonstrated an apparent urn-variate association between hypertriglyceridemia and coronary heart disease which may have clinical utility if used in conjunction with raised blood cholesterol level. More studies are required to explore the role of triglycerides in the development of CHD. Measurement of cholesterol in major lipoproteins has more significant value especially LDL and HDL. This study also suggests that concentration of HDL2 cholesterol may provide a more sensitive predictor for subjects at risk of developing CHD.
Acknowledgement
We are grateful to Dr. S. N. Shah, Associate Professorof Cardiology, Dr. Jahangeer and Dr. Aqeel Resident Medical Officers of National Institute of Cardiovascular Disease Karachi for the clinical material used in this study.
References
1. Kissane. J. M. and Anderson, W A. D., Heart, I.N. Anderson’s pathology (8th ed). The C. V. Mosby company St. Louis, Toronto Princeton, C. B. Mosby Compnay, 1985, pp. _77-688.
2. Hulley, S. B., Roseman, R. H., Bawol, R. D. et at. The association between triglyceride and coronary heart disease. N. Engi. J.Med., 1980;302: 1382-89.
3. Strong, J. P., Restrepo, G. and Solberg, L. A. Introduction to geographic pathology of atherosclerosis. Circulation, 1966.34 (supp-3):31-34.
4. Albrink, M. J. and Man, E. B. Serum triglycerides in coronary artery disease. Arch. Intern. Med., 1959;103:4-8:
5. Antonss, A. and Bershon, I. Serum triglyceride levels in South African Europeans and Bantu in ischaemic heart disease. Lancet, 1960;1 :989-1002.
6. Goldstein, J. L., Hazzard, w. R., Schrott, H. G. et at. Hyperlipidemia in coronary heart disease Lipid levels in 500 survivors, of myocardial infarction. 3. Clin. Invest, 1973;52:1533-1543.
7. Salel, A. F., Riggs, K., Masson, D. T. et at. The importance of type IV hyperlipoproteinaemis as a predisponsing factor in coronary heart disease. Am. J. Med., 1974;57:897-903.
8. Hyden, S., Heiss, G., Hames, C. G. et al. Fasting triglycerides as predictors of total and CHD mortality in Evans Country, Georgia. J. Chronic Dis., 1980;33:275-82.
9. Kennel. W. B., Dawber, T R., Friedman, G. D. et al. Risk factors in CHD an evaluation ofseveral serum lipids as predictors of CHD The Framingham study. Ann. Intern. Med., 1964;61:888-899.
10. Brewer, H.B., Gregg, R. E., Hoeg, 3. M. et al. Apolipoproteins and lipoproteins in human plasma. Clin. Chem., 1988;34:4-7.
11. Hawel, R. J., Goldstein, 3. L. and Brown, M. S. Lipoprotein and lipid transport, In Vondy P.K. and Rosenberg, L.E., Metabolic control and disease 8th ed Philadelphia. WB Saunders Co., 1980, pp. 393-494.
12. Gordon, T., Castelli, W.P., Hijortland, C. et al. High density lipoprotein as a protective factor against coronary heart disease. Am. 3. Med., 1977;62:707-14.
13. Naito, H. K. The association of serum lipids, lipoproteins and apotipoproteins with coronary artery disease assessed, coronary angiography. Ann. N. Y. Acad. Sci., 1985,454:230-38.
14. Shefique, M., Mirza, W. B., Hussain, S. et al. Study of lipoproteins in patients of myocardial infarction in B. V. Hospital, Bahawalpur Pak.J. Med. Res., 1988;27: 186-90.
15. Jenkins, P. J., Harper, R. W. and Nestel, P. 3. Severity ofcoronary atherosclerosis related to lipoprotein concentration. Br. Med. J. 1978;2:388-91.
16. Pearson, T. A., Bulkley, B. H., Achoff, S. C. et al. The association of low levels of HDL cholesterol adn arteriographically defined coronary artery disease. Am. J. Epidemiol., 1979;109:285-95.
17. Gofman, J. W., Young, W. and Tandy, R. Ischaemic heartdisease, atherosclerosis and longevity. Circulation, 1966;34:679-697.
18. Anderson, D. W., Nichols, A. V., Pan, S. S. et al. High density lipoprotein distribution. Atherosclerosis, 1978;29: 161-179.
19. Steinberg, D., Calif, L. 3., Blumenthal, S. et al. Consensus conference. Lowering blood cholesterol to prevent heart disease. JAMA., 1985,253:2080-2086.
20. Zilversmit, D. B. Atherogenesis. A postprandiol phenomenon. Circulation, 1979;60:473-85.
21. Siedel, 3.. Schlumberger, H., Klose, S. et al. Determination of cholesterol after enzymatic hydrolysis. 3. Clin. Chem., 1981 ;19:838-40.
22. Burstein, M., Scholnick, H. R. and Morfin, R. Rapid method for the isolation of lipoproteins from human sera by precipitation with polyanions. 3. Lipid. Res., 1970;11:583-95.
23. Gidez, L. 1., Miller, G. T., Burstein, M et at. Separation and quantification of subclasses of human plasma high density lipoproteins by a simple precipitation procedure. J. Lipid. Res., 1982;23:1206-1223.
24. Delong, D. M., Delong, E. R., Wood, P. H. et al. Comparison of methods for the estimation of plasma low and very low density lipoprotein cholesterol. JAMA., 1986;256:2372-2377.
25. Khan, N. A., Shah, M. Z. and Roghani, M. T. Epidemiology of coronary heart disease in Peshawar. Pak. Heart 3., 1973;6:64-71.
26. Gianturco, S. H., Brown, F B., Gotto, A. M. et al. Receptor mediated uptake of hypertrig lyceridermic very low density lipoproteins by normal human fibroblasts. J. Lipid Res., 1982;23:984-993.
27. Lippel, K., TLyroler, H., Eder, H. et at. Relationship ofhypertriglyceridemia to atherosclerosis Arteriosclerosis, 1981;1:406-417.
28. Thind, 0. S. and Sandhu, R. S. Significance of high density and total cholesterol and triglycerides in acute myocardial infarction. Clin. Biochem, 1981 ;14: 57-61.
29. Brunzetl, 3. D., Albers, 3. 3.. Chait, A. et al. Plasma lipoproteins in familial combined hyperlipidemia and monogenic hypertriglyceridemia. J. Lipid Res., 1983;24: 147-55.
30. Tornvatl, P., Bavenholm, P., Landou. C. et at. Relation of plasma levels and composition of apolipoprotein B-containing lipoproteins to angiographically defined coronary artery disease in young patients with myocardial infarction. Circulation, 1993;88:21 80-2.
31. Ginter, E. Plasma cholesterol level and ischaemic heart disease, new finding and new approaches. Bratisl. Lek. Listy., 1992;93:67- 75.
32. Yamamura, T., Tajima, S., Miyake, Y. et at. Hyperlipoproteinaemia as a risk factorfor ischaemic heart disease. Jpn. Circ. 3., 1991 ;54:448-456.
33. Keys, A. Alpha lipoprotein (HDL) cholesterol in the serum and the risk of ,, coronary heart disease and death. Lancet, 1980;11:603- 606.
34. Muhonen, L. E., Burns, T. L., Nelson, R. P. et a!. Coronary risk factors in adolescents related to their knowledge of familial CHD and hypercholesterolemia. Pcdiatrics, 1994;93:441-451.
35. Miller, N.E., Hammett, F, Saltissi, S. et al. Relation ofangiographically defined coronary artery disease to plasma lipoprotein subfractions and apolipoproteins. Br. Med. J., 1981,282:1741-4744.
36. Wilson, H. M., Patel, J. C., Russell, D. et al. Alternations in the concentration of an apolipoprotein E containing subfractions of plasma high density lipoproteins in coronary heart disease. Clin. Chem. Acta., 1993,220:1755-87.
37. Shahid, A. and Surraiya, 0. The effect of suiphonylureas on HDL cholesterol and subfractions of HDL cholesterol in Type II diabetic patients. Pak. J. Med. Res., 1988;27:86-90.
38. Simson, L. A. Interrelations of lipids and lipoproteins with coronary artery disease mortality in 19 countries. Am. J. Cardiol., 1986;57:5G10G.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: