
Mohammad Idris ( Departments of Radiology, Ayub Medicai College, Abbottabad. )
Mohammad Ilyas ( Department of Community Medicine, Ayub Medicai College, Abbottabad. )
Shah Jehan Afridi ( Department of Radiology, Ayub Medicai College, Abbottabad. )
October 1996, Volume 46, Issue 10
Original Article
Abstract
Gout an ancient disease not uncommonly seen in radiological practice. Twenty-two patients of suspected gout were examined aye: a period of 11 years (1984-1995). There were 20 males and 2 females with ages between 35-70 years. First metatarsophal geal joint was involved in 18 patients. Tophaceous deposits in hands were seen in one, whereas another patient had urate deposit in the lateral condyle of the humerus. One patient had O aqua renal stones bilaterally and lucent stones in the right kidney,: confirmed by ultrasound, were observed in one case. All of the patients had hyperuricemia. A definite family history was recorded in only three cases. Two patients in the present series were diabetic (JPMA 46: 218, 1996).
Introduction
Gout was known to Hippocrates (500 B.C.), Gallen and Celsius recognized that it affected rich and powerful people; Garrod included itin "inborn errors of metabolism” in 1909, although an inherited tendency to the disease was suspected by Romans 2000 years ago1. Gout results from the tissue deposition of monosodium urate or uric acid crystals from the extracellular fluid saturated with this end product of purine metabolism Radiology plays a vital role in confirming the clinical diagnosis and in elucidating various aspects of the disease process. Although the big toe is classically affected, yet the disease has a tendency to involve long bones, soft tissues and kidneys2.
Patients and Methods
Twenty-two consecutive patients with clinical diagnosis of gout were examined radiologically over a period of 11 years (1984- 1995). Brief clinical history, relevant laboratory investigations and radiological findings were recorded and analysed.
Results
Of twenty-two patients examined, 20 were males and only two females. Their ages ranged between 35-70 years (Table I).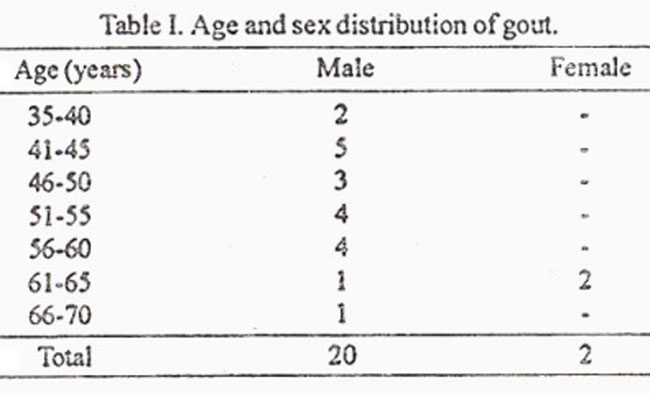
Right 2metatarsophalangeal joint was affected in 11 and the left in 7 patients. Acute episode with non-specific swelling of soft tissue was observed in two cases. Typical punched out erosions were present in 16 patients (Figure 1).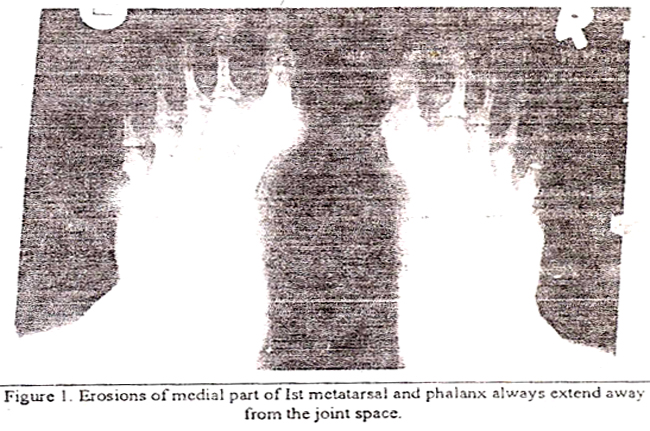
Lumpy tophy in hands, more marked on the right side were present in one patient, showing calcification and typical overhanging margins (Figure 2).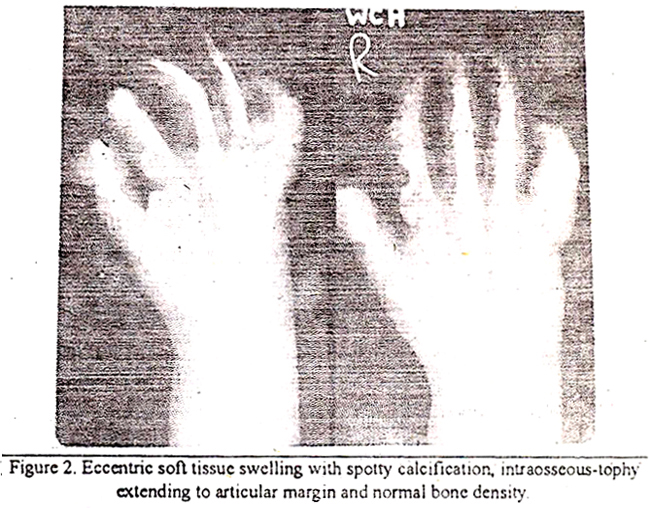
One patient had a large lytic deposit of urate cr stals in the lateral condyle of the humerus (Figure 3).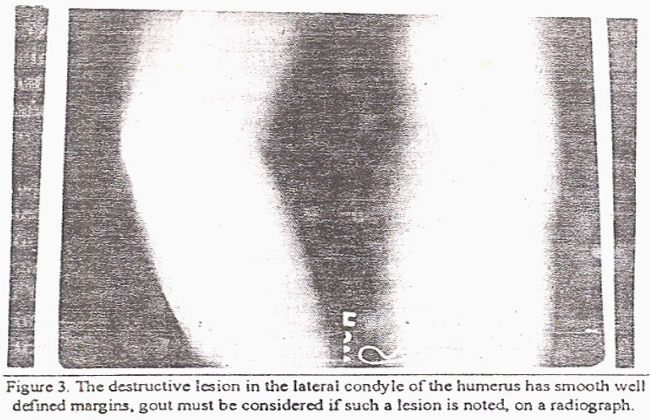
One patient showed bilateral opaque renal stones with hydronephrosis whereas, another had a history of passing stones. Plain radiograph of the abdomen was normal hut ultrasound examination showed stones in right kidney. All the patients in the series had hyperuricenila (Table II).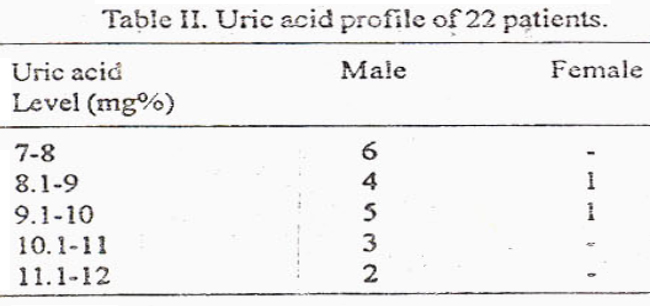
Discussion
Only man and great apes excrete uric acid a~ the end product of purine metabolism and are thus liable to develop gout. Exact prevalence of gout in Pakistan is not known. in USA and Europe, it is about 0.3% while in Newzealand, it is 10.3% in men and 4.3% in women3. Over 90% of patients with primary gout are men. The peak age in men is earlier than women, who rarely develop the disease before menopause4. Gout is rare before the third decade of life, therefore, an onset before the age of 30 years should raise the suspicion of a specific enzyme defectorsome intrinsic renal disease5.
In this study the age and sex distribution of disease matched closely with those quoted in literature4,5. None of our patient was below 35 years of age and the two females were 61 and 63 years old. Major radiographic findinngs in the initial episodc of gout is non-specific soft tissue swelling. Long standing gout displays asymmetric inflammatory erosive arthritis accompanied by soft tissue nodules. Bony and periarticular density is retained and joint space remains intact6. Sharply punched out round/oval defects with sclerotic margin are situated in the periarticular region. First metatarsophalangeal joint is classically involved and is most common site affected. This finding was observed in 18 of our patients.
Bony tophaceous lesion almost always antedates subcutaneous tophi and may be seen in a non-inflammedjoint7. This was noticed in the lateral condyle of humerus in one patient. In patients with gouty erosion in bone, an elevated margin extends outward into the soft tissue covering the tophaceous nodule. This overhanging margin of bone is characteristic of gout. Another feature typical of gout is paucity ofperiarticular osteoporosis5. One of our patients with tophi in hands showed typical overhanging margins and calcification of the tophi which is an unusual feature8. Chondrocalcinosis and punched out lesions with sclerotic margins in the sacroiliac joint9,10were not seen in this study. Uric acid stones account for 5-10% of renal lithiasis11. These are radio-lucent and appear on the contrast film as filling defects. Ultrasonography easily detects these stones as was the case in one of our patients. Radio-opaque stones also occur frequently in gouty subjects and are largely composed of calcium oxaiate These stones often contain a small amount of uric acid which serves as a nidus for the deposition of calcium oxaiate.
Hereditary tendency has long been suspected in gout. Gout has been reported in family members of 38-81% of patients12. In United States familial incidence ranged from 6-18%13.. In our series three (15%) patients had a definite f mi lv history which corresponds well with the latter series.
References
1. Hitchings. G.H. Unc acid Chemistry and synthesis: I Uric acid; handbook of experimental pharmacology. Edited by Kelly, W N and Werner. I M Volume 5. New York, Spring Verlag, 1978, pp. 378-80.
2. Bloch C. and Hermann, G. A radiological reevaluation of gout. Am.J.Radiol., 1990,134 781-87
3. Lawrence, J S Heritable disorders of connective tissue Proc R.Soc Medicine 1960,53 522-26
4. Berthalmy CR. Nakayamo. DA. Carrera, G.F. etal. Gouty arthritis,a prospective ographyic evaluation of 60 patients Skeletal Radiol., 1984,1 1.14.
5. Wallac, S.L. Preliminary critena for the classification ofgout. Arthritis Rhesus., 1977;20:895-900.
6. Walt, I. and Middlemiss, H. The radiology ofgout. Clin. Radial., 1975;26:27-30.
7. Nakayema. D.A. Tophaceaous gout; A clinical and radiological assessment Arthritis Rheum., 1984;27:468-71.
8. Good, A E. and Rapp, R. Bony ankylosis. A rare manifestation of gout. J. Rheumatol., 1978 ;5:335-37.
9. Dodds, W. J. and Steinbach, H.L. Gout associated with calcification of cartilage N. Engl. 3. Med , 1966,275 .745-49.
10. Jagie, I Gout in the spine and sacroilac joints. Skeletal Radiol., I 983;8::209-10.
11. Herring, I.J, Obscrvation on the analysis of ten thousands calculi, J. Urol., I 962;88:545-62.
12. Cohen, H. (‘out and other metabolic disorders producing joint diseases; Is textbook of Rheumatic diseases. Edited by Copeman, W.S.C. Living stone, Edinburgh. 1965, pp. 182-86.
13. Resneit, 0. and Reir.ka, R.M Early onset gout) arthritis, Radiology 1975;1 14:67-73.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: