
Muhammad Tariq Baqai ( Department of Medicine, Islamic International Medical College, Rawalpindi. )
Mahmood Nasir Malik ( Department of Medicine, Allama Iqbal Medical College, Lahore. )
Faisal Ziauddin ( Department of Medicine, Ziauddin University, Karachi. )
June 2013, Volume 63, Issue 6
Original Article
Abstract
Objective: To study the efficacy and safety of cinitapride in the treatment of functional dyspepsia, and to evaluate the improvement of patients\\\' quality of life.
Methods: The prospective cross-sectional multi-centre phase IV study was conducted at Jinnah Hospital, Lahore, Ziauddin Medical University, Karachi and Pakistan Railways General Hospital, Rawalpindi, from July 2009 to June 2010 and comprised 121 patients of functional dyspepsia who were given cinitapride 1mg thrice daily 15 minutes before meals and were followed up for four weeks. Primary clinical response was assessed by using the Global Index Score. Secondary response was seen by percentage change of the total score as well as of each dyspepsia symptom compared with baseline and the overall subjective assessment of patients by using the 7-point Likert\\\'s scale. Reduction in Nepean Dyspepsia Index-Short Farm was used to evaluate the improvement in quality of life of patients at week 2 and 4. SPSS 15 used for statistical analysis.
Results: After 4 weeks of treatment, the Global Index Score showed statistically significant reduction in 58 (48.92%) patients (p<0.01). Similar reduction (p<0.01) was seen in individual dyspepsia symptoms; early satiety, post-prandial fullness, and abdominal distension. The 7 point Likert\\\'s scale also showed similar improvement in subjective response (p<0.01). The quality of life also improved significantly at week 2 and 4 (p<0.01). No abnormal results were seen in vital signs, physical and laboratory examination except an unexplained rise in globulin level. Only one adverse event (sore throat) was reported during the study.
Conclusion: The drug was effective in minimising dyspepsia symptoms, and improving the quality of life of patients. It was well tolerated and was almost free of side effects.
Keywords: Cinitapride, Functional dyspepsia, Global index score, Likert\\\'s scale. NDI-SF. (JPMA 63: 747; 2013).
Introduction
Functional dyspepsia can significantly influence the quality of life of patients. Because of the diversity of etiological factors and pathogenesis, there is still no satisfactory therapy available. It is a poorly defined symptom complex pertaining to the upper gastrointestinal tract (GIT) with worldwide distribution.1 Its prevalence varies in different countries. There is a significant socio-economic impact of dyspepsia on community.2 Guidelines for investigations and treatment are far from satisfactory because of the diversity of etiological factors and pathogenesis. Traditional and pharmacological interventions are widely used for treatment.
Cinitapride, a pro-kinetic agent of GIT activates myenteric nerve plexus and promotes the release of acetylcholine; which favours propulsive movement of GIT. Cinitapride indications include functional dyspepsia and functional gastrointestinal motor disorders. Clinical trials and patients\\\' feedback demonstrate its excellent therapeutic profile and safety. The current study was done to investigate the efficacy and safety of the drug in the treatment of functional dyspepsia, and to evaluate the improvement of quality of life in Pakistani patients.
Patients and Methods
The multi-centre phase IV randomised controlled trial was conducted at Jinnah Hospital, Lahore, Ziauddin Medical University, Karachi and Pakistan Railways General Hospital, Rawalpindi, from July 2009 to June 2010.
Patients >18 years of age with at least three symptoms from among early satiety, fullness, abdominal distension or bloating, nausea or vomiting, over the preceding three months occurring at least twice a week were included in the study.
Those with predominant symptoms of gastroesophageal reflux disease (GERD), patients with known history of peptic ulcer disease, malignancy, use of non-steroidal anti-inflammatory drugs (NSAIDs), pregnancy, age below 18 years, those with hepatobiliary disease, or breastfeeding were all excluded. Drugs with an anti-kinetic action (e.g.: calcium antagonists, beta-blockers, anti-cholinergic drugs, anti-convulsants, opiates, etc.), drugs with a pro-kinetic action (5-HT4 agonists, D2 antagonists, cholinergic, macrolide antibiotics, etc), proton pump inhibitors, antacids (more than twice a week) were discontinued two weeks prior to the commencement of the study. Antacids if taken less than twice a week, anti-depressants at a low constant dose (over the preceding 3 months) and other chronic medication judged not likely to interfere with the study medication and trial objectives were allowed.
After screening, 40 eligible subjects were enrolled at each of the three sites. Sample size of 125 subjects was calculated with 95% confidence level, 5.5% margin of error and taking the prevalence of functional dyspepsia at 11% among normal population. After selection all patients were explained about the use of the medicine. They were given free supply of medicine as well as free lab tests as incentives for followup. Patients refusing to participate were excluded. The treatment lasted for four weeks and the efficacy and safety was evaluated at week 2 and 4 after administration.
Initial workup included blood complete picture (CP), liver function test (LFT), renal function test (RFT), blood sugar, lipid profile, electrocardiogram, ultrasound abdomen and hepatitis B and C screening as it can cause alteration in parametres like CP, LFT etc. Moreover, the patient may be on anti-viral therapy which further interfers with the parametres. Those found positive for hepatitis B and C were excluded and referred for further investigations and treatment. Upper gastrointestinal (GI) endoscopy was performed on all patients except those who refused the procedure. Those who had endoscopic findings that were not considered clinically relevant (small hiatal hernia, grade A oesophagitis) were also included.
Efficacy was assessed by the number of subjects whose total score of dyspepsia symptoms were reduced by more than 50%. The calculation was based on the formula: (Total Score pre-treatment — Total Score post-treatment)/ Total Score pre-treatment×100%). Subjective and objective assessment was done by using the 7-point Likert\\\'s scale.3 The quality of life was assessed by Napean Dyspepsia Index Short Form (NDI-SF).4
The primary efficacy endpoint was percentage change of the total score of dyspepsia symptoms at the end of week 4 compared with baseline as well as in 3 individual symptoms; early satiety, post-prandial fullness, abdominal distension/bloating after food intake. Secondary endpoints included percentage change of the total score of dyspepsia symptoms at the end of week 2 compared with baseline reduced by more than 50%.
Safety and tolerability were assessed by the analysis of adverse events, abnormal results of vital signs, physical examination and laboratory examination that were done at the baseline and were repeated at the end of the study. All adverse experiences were rated by the study investigators for intensity and relationship to the study medication. Laboratory safety evaluation included haematology, RFT, LFT and lipid profile.
The study was approved by the institutional review board of Allama Iqbal Medical College for all the three sites. All patients gave their written informed consent, and the study was conducted according to the principles of Good Clinical Practice.
SPSS version 15 was used for all statistical analyses. Statistical significance was put at p<0.05. Descriptive statistics were calculated to analyze demography and other background data of subjects; all adverse events were listed and analysed by descriptive statistics. Efficacy was analysed by chi-square test to compare the categorical data like difference in efficacy in different age quartiles, males and females and diabetic and non-diabetic populations; and t-test was applied to other numerical data like change in the Global Index and Likert\\\'s scale. Normality test was also performed for numerical data.
Results
Of the 300 patients initially evaluated, 121 (40.33%) patients represented the final sample size. The normality test showed a value below 0.05, showing significant deviation from a normal distribution (Table-1).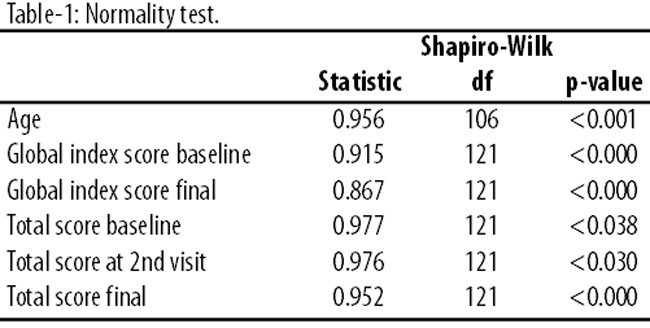
The most common reason of patients not being included in the study was abnormal laboratory results. The mean age of the patients included was 34.40±11.41 years; mean height in inches was 64.67±3.98; and the mean weight in pounds was 132.69±30.33. There were 53 (43.8%) males and 68 (56.2%) females. Helicobacter pylori was positive in 29 (24%) patients, and abnormal ECG was seen in 5 (4.1%). They completed the study without any problems.
Baseline Global Dyspepsia Index (GDI) was 13.02±6.31. At the end of four weeks the GDI came down to 6.65±4.05 (p<0.0001). Efficacy, as calculated by Chi-square, was more significant in females (n=34; 49.89%) compared to males (n=25; 47.42%). Efficacy was achieved in 58 (47.9%) cases after 4-weeks treatment (Figure-1).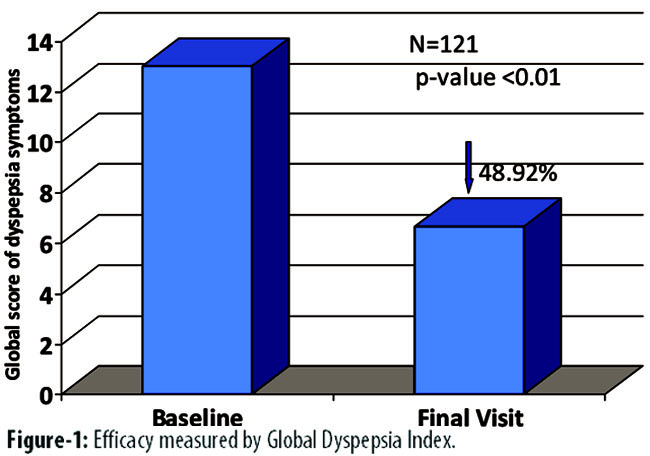
The overall subjective response assessed by the 7-point Likert\\\'s scale applying the t-test showed highly significant improvement of 185% (p<0.01). The scale at baseline was 2.12±0.96 which improved to 6.05±1 at the final visit.
The quality of life was evaluated by using the NDI-SF at week 2 and at final visit by applying the t-test. There was a marked improvement from baseline values 32.98±8.36 to 26.61±6.65 (p<0.01) at week 2 and at week 4 they further improved to 19.81+5.82 (p<0.01) (Figure-2).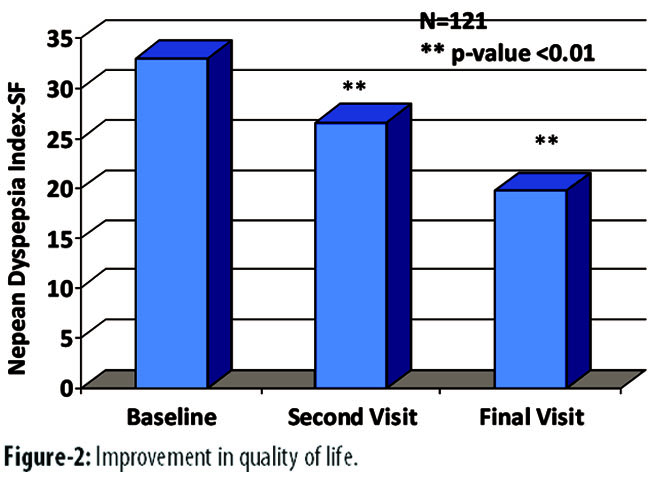
Analysis of individual symptoms (early satiety, post-prandial fullness, bloating and abdominal distension) also showed marked improvement by applying t-test from baseline to second visit to the final one. The drug significantly improved early satiety and at the final visit, 91 (75.2%) patients had mild symptoms (p<0.01); only 1 (0.82%) patient still complained of severity. The subjective improvement in early satiety was also statistically significant, and at the final visit 112 (92.56%) patients had either mild or only occasional early satiety (p<0.01). Five (4.13%) patients became symptom-free at the end of the final visit.
Post-prandial fullness improved highly significantly (p<0.01) as 114 (94.21%) patients rated their symptoms as mild or moderate. Objectively, 4 (3.30%) patients were symptom-free at the final visit. Only 3 (2.47%) patients complained of severe symptoms at the final visit. The subjective improvement was highly significant as well (p<0.01) with 115 (95.04%) patients rating their symptoms as rare or occasional, and 2 (1.65%) patients being entirely symptom-free.
Abdominal distension showed marked improvement in both objective and subjective assessment (p<0.01): 75 (61.98%) patients rated their symptoms as mild, and 37 (30.57%) rated it as moderate at the final visit; 2 (1.65%) patients had no symptoms at the final visit. The subjective improvement also matched this as 113 (93.38%) patients had rare or occasional abdominal distension on the final visit. Only 7 (5.78%) patients still complained of abdominal distension more than three times a week at the final visit, compared to 59 (48.76%) patients at the baseline.
The overall responder\\\'s rate to subjective pain assessment as evaluated by the Likert\\\'s scale was 73.55% (n=89). At the final visit, these patients were either \\\'much better\\\' or \\\'quite better.\\\' The difference between baseline to 2nd visit to final visit was statistically significant (p<0.001).
Diabetes mellitus (DM) was present in 13 (10.7%) patients. Some were previously known to have diabetes, while others were diagnosed during the study. Efficacy could not be achieved in diabetic patients as per the study protocol (reduction in symptoms score by 50%). Nonetheless, the drug significantly (p<0.01) reduced mean GDI symptoms from the baseline to the final visit.
Profile of investigations done at the start and at the end of study included CP, LFT, and blood sugar, Gamma-gluamyl transpeptidase (GGT), haemoglobin and ECG. No significant side effects were observed during the study. Treatment continued in all the enrolled patients and none of the subjects dropped out. One (0.82%) patient complained of sore throat and the causal relationship to the drug could not be established, and the patient completed the study successfully. At the end of the week 4, there was a rise in the plasma globulin level. However, albumin and plasma protein levels did not change significantly during the study (Table-2).
Discussion
Comprehensive definition of dyspepsia is still undecided. Every few years wise men like cardinals gather in Rome and come out when they agree on a new version. Once Rome has spoken, it is accepted by all. Currently Rome III definitions is accepted.5,6
In Western societies prevalence of dyspepsia varies from country to country with highest reported from the UK, and the lowest from Sweden.7 In Asian countries like Pakistan, South Korea, Malaysia8,9 it is more common. Functional dyspepsia has a significant socio-economic impact on individuals as well as on the community.10
Presentation of functional dyspepsia varies from culture to culture. Usual manifestations include post-prandial bloating, heaviness, early satiety, belching. These may occur in combination or singularly. Sub-typing into reflux, ulcer like or dysmotility has been tried, but often overlapping features make it difficult to accurately sub-classify.11,12 An earlier local study came across unique description which it described as 3-G syndrome. Patients frequently used the term Gas, \\\'Gola\\\' (mass) or Gastric to describe their complaints.9
Extent of investigation for patients with dyspepsia is variable. Usually structural disease of the upper GIT is excluded by oesophago-gastro-duodenoscopy or barium studies. It is accepted that upper GI endoscopy should be performed on all patients with alarm features like anaemia, weightloss, GI bleeding especially in patients above 50 years of age.13
Pathogenesis of functional dyspepsia is unclear. Delayed gastric emptying has been reported in several studies in patients with functional dyspepsia.14 Most therapeutic interventions are based on accelerating gastric emptying with the use of pro-kinetics with variable results.15
Pro-kinetics like Cinitapride augment the contractility of GIT, promoting quick expulsion of gastric contents from stomach into the small intestine, thereby improving the symptoms of functional dyspepsia. Metoclopramide has been used for prompt emptying of barium during barium studies. Its effectiveness for short treatment of dyspepsia has been well documented.16,17 However, extra-pyramidal side effects have been a problem with its use.
Lately emphasis has been on the use of 5HT4 receptor agonists for the treatment of functional dyspepsia. Cisapride belonging to the same group was very successful when it was first launched. The drug was, however, withdrawn due to reports of sudden deaths due to cardiac arrhythmias.18
Cinitapride was introduced in 1990 and has a three-pronged mechanism of action; it acts as an agonist at 5HT4 serotonergic receptor and as an antagonist at 5HT2 serotonergic and D2 dopaminergic receptor. It is a potent inducer of GI peristalsis by way of its synergistic action at the level of myenteric plexus. Several phase II studies have demonstrated the beneficial effects of Cinitapride in improving gastric emptying as well as its safety profile.
In our phase IV study, we found a significant improvement in presenting symptoms of dyspepsia. Analysis of the presenting symptoms showed that commonest symptom the patients had at the time of enrolment in the study was delayed gastric emptying. The improvement at the end of four weeks was primarily due to the pro-kinetic activity of the drug.
Parametres we used for assessing the response are well accepted for the assessment of response in patients with dyspepsia. Symptoms of early satiety, post-prandial fullness and abdominal distension were present in almost all of the cases at the beginning of the study and showed significant improvement. We did not find any improvement in GDI score in diabetic patients, suggesting other factors may be involved in the pathogenesis of dyspepsia in diabetic patients. Since this was a short study (4 weeks) it is worth reasoning that the results could have been different in a longer study. Besides, we did not measure albumin loss by renal or GIT route to explain the increase in globulin levels. As initial RFTs were within normal limits they were repeated at the end of study, but not at the 2nd visit.
Conclusion
Standard uniform treatment has yet to be established for functional dyspepsia. However, pro-kinetics have shown good promise in several studies, and the current study also endorsed that view.
Acknowledgement
We are grateful to Highnoon Laboratories Limited for financial support, and to Dr. Asad Azeemi, Dr. Imran Haider, Dr. Sanam Dahri (Clinical Research Associates at Highnoon) who provided logistical support.
References
1. Talley NJ, Stanghellini V, Heading RC, Koch KL, Malagelada JR, Tytgat GN. Functional gastroduodenal disorders. In: Drossman DA ed. Rome II: The Functional Gastrointestinal Disorders. McLean, VA: Degnon, 2000; pp 299-350.
2. Haycox A, Elnarson T, Eggleston A. The health economic impact of upper gastrointestinal symptoms in the general population: result from the Domestic/International Gastroenterology Surveillance Study (DIGEST). Scand J Gastroenterol Suppl 1999; 231: 38-47.
3. Likert R. A technique for the measurement of attitudes. Archives of Psychology. 1932; 22: 1-55.
4. Talley NJ, Verlinden M, Jones M. Quality of life in functional dyspepsia: responsiveness of the Nepean Dyspepsia Index and development of a new 10-item short form. Aliment Pharmacol Ther 2001; 15: 207-16.
5. Drossman DA, moderator. AGA Clinical Symposium-Rome III: New criteria for the Functional GI Disorders. Program and abstracts of Digestive Disease Week; May 20-25, 2006; Los Angeles, California. (Sp461-469).
6. Drossman DA. The functional gastrointestinal disorders and the Rome III Process. Gastroenterology 2006; 130: 1377-90.
7. Knill-Jones RP. Geographical differences in the prevalence of dyspepsia. Scand J Gastroenterol Suppl 1991; 182: 17-24.
8. Mahadeva S, Yadav H, KL G. Impact and risk factors for dyspepsia in urban South East Asians: a population-based study. Gastroenterology 2007, 132S: A267.
9. Baqai MT, Iftikhar M, Khan R. A dyspepsia: description, division and distribution in urban community JRMC 2004; 8: 26-9.
10. Moayyedi P, Mason J. Clinical and economic consequences of dyspepsia in the community. Gut 2002; 50 suppl 4: 10-2.
11. Heikkinen M, Färkkilä M. What is the long-term outcome of the different subgroups of functional dyspepsia? Aliment Pharmacol Ther 2003; 18: 223-9.
12. Chiba N, Bernard L, O\\\'Brien BJ, Goeree R, Hunt RH. A Canadian physician survey of dyspepsia management. Can J Gastroenterol 1998; 12: 83-90.
13. Fransen GA, Janssen MJ, Muris JW, Laheij RJ, Jansen JBMJ. Meta-analysis: The diagnostic value of alarm symptoms for upper gastrointestinal malignancy. Aliment Pharmacol Ther 2004; 20:1045-52.
14. Talley NJ, Locke III GR, Lahr BD, Zinsmeister AR, Tougas G, Ligozio G, et al. Functional dyspepsia, delayed gastric emptying and impaired quality of life. Gut. 2005; 55: 933-9.
15. Sturm A, Holtmann G, Goebell H, Gerken G. Prokinetics in patients with gastroparesis: a systematic analysis. Digestion 1999; 60:422-427.
16. Moayyedi P, Soo S, Deeks JJ, Delaney B, Innes M, Forman D. Pharmacological interventions for non-ulcer dyspepsia. Cochrane Database Syst Rev 2000; CD001960. Published Online: 16 February 2011. DOI: 10.1002/14651858.CD001960.pub4.
17. Perkel MS, Moore C, Hersh T, Davidson ED. Metoclopramide therapy in patients with delayed gastric emptying: a randomized, double-blind study. Dig Dis Sci 1979; 24:662-666.
18. Griffin JP. Prepulsid withdrawn from UK & US markets. Adverse Drug React Toxicol Rev 2000; 19: 177.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: