
Azizun-Nisa ( Department of Pathology and Microbiology, Faculty of Health Sciences, Medical College, Aga Khan University Hospital, Karachi, Pakistan. )
Zeeshanuddin ( Department of Pathology and Microbiology, Faculty of Health Sciences, Medical College, Aga Khan University Hospital, Karachi, Pakistan. )
Naila Kayani ( Department of Pathology and Microbiology, Faculty of Health Sciences, Medical College, Aga Khan University Hospital, Karachi, Pakistan. )
May 2013, Volume 63, Issue 5
Case Reports
Abstract
Angiosarcomas account for less than 0.05% of the malignant neoplasms of the breast. We present here 7 cases of malignant vascular neoplasms of the breast, including 2 cases of post-mastectomy Stewart-Treves syndrome. In this case series, most of the patients were young. Tumour was bilateral at presentation in one case. The size of the tumours ranged from 1.6 cm to 11cm. Although breast angiosarcomas are rare neoplasms, with the increasing use of radiation therapy for breast cancer patients, post-radiation skin lesions should not be ignored.
Keywords: Angiosarcoma, Malignant vascular tumours of breast, Stewart-Treves syndrome, Lymphangiosarcoma, Breast neoplasms.
Introduction
Primary breast sarcomas, excluding phyllodes tumour, are exceedingly rare tumours, accounting for less than 0.1% of all the malignant tumours of the breast and, among these, angiosarcomas account for less than 0.05% of all the malignant neoplasms of the breast.1 They can arise de novo (primary) or as a consequence of treatment of an epithelial breast cancer (secondary). Post-mastectomy angiosarcoma (Stewart-Treves syndrome) is usually a complication of the treatment of mammary carcinoma in which the angiosarcoma arises in association with lymphoedematous upper extremity.2
Angiosarcoma arising in the setting of radiation therapy for breast carcinoma is a well-established iatrogenic phenomenon and mainly involves the skin, with or without occasional invasion of the subjacent breast parenchyma. In contrast, primary mammary angiosarcoma arises within the breast parenchyma and may secondarily infiltrate the overlying skin and subcutaneous tissue.
Herein, we present 5 cases of breast angiosarcoma and 2 cases of Stewart-Treves syndrome along with review of relevant literature.
Case Series
Case-1
The first case was of a 16-year-old female with no clinical details. We received a right breast lump measuring 4x2.5x2cm, showing greyish white to brown firm cut surface with intervening areas of haemorrhage and necrosis. Microscopy revealed solid sheets of markedly pleomorphic cells exhibiting occasional foci of lumina formation. Diffuse positive staining of Factor VIII immunohistochemical marker confirmed the vascular nature of the tumour cells. Ultimate diagnosis was of poorly differentiated angiosarcoma.
Case-2
The second case was of a 74-year-old woman with past history of infiltrating ductal carcinoma followed by chemoradiotherapy. Microscopy of the material revealed complex slit-like intercommunicating vascular channels lined by atypical endothelial cells. Surrounding the vascular channels were clusters of cells showing variably pleomorphic nuclei. In certain areas, tumour cells were seen dissecting through and entrapping the collagen bundles, creating pseudopapillary arrangement. The case was diagnosed as moderately differentiated lymphangiosarcoma (Stewart-Treves syndrome).
Case-3
A 30-year-old female presented with breast lump that was excised followed by mastectomy. The tumour measured 3.5x3x1cm and had a greyish brown haemorrhagic cut surface. Histological examination revealed an infiltrating lesion showing capillary-like slit structures with solid component consisting of spindle-shaped tumour cells (Figure 1-1).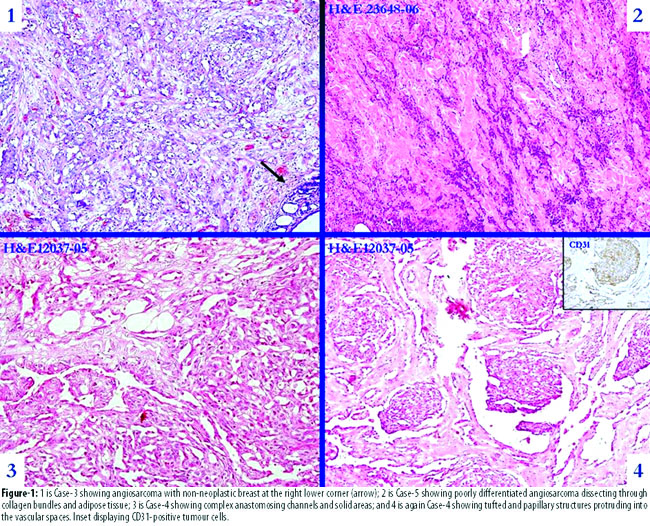
Scattered mitotic figures and intermingled foci of haemorrhage were seen forming blood lakes. Tumour cells were positive for CD31 stain. The diagnosis was well-differentiated angiosarcoma.
Case-4
The fourth case was of a 32-year-old female with no clinical history provided. Microscopy revealed anastomosing vascular channels lined by atypical endothelial cells. Few dilated vascular channels exhibited the protrusion of nested and tufted tumour clusters (Figure-1-3). Focally solid areas were seen with increased mitotic activity. On immunohistochemical staining, tumour cells were positive with CD31 (Figure 1-4). This was diagnosed as moderately differentiated angiosarcoma.
Case-5
The fifth case related to a 72-year-old patient with prior history of infiltrating carcinoma with chemoradiotherapy. She presented with left-arm swelling with clinical impression of lymphangiosarcoma. Microscopy revealed an infiltrating neoplastic lesion composed of clusters and groups of polygonal to spindly atypical cells having vesicular pleomorphic nuclei and prominent nucleoli. Few areas showed well-formed closely-packed vascular channels lined by atypical endothelial cells (Figure 1-2). Positive CD31 immunohistochemical staining confirmed the vascular nature of the tumour. The case was diagnosed as poorly differentiated lymphangiosarcoma (Stewart-Treves syndrome).
Case-6
A 22-year-old patient presented with bilateral involvement of the breasts with past history of lumpectomy of the left breast a year ago. We received left breast mastectomy specimen and right breast lump. On sectioning of the left breast specimen, a fairly circumscribed multi-nodular blackish brown, mostly solid firm lesion was identified (Figure 2-1)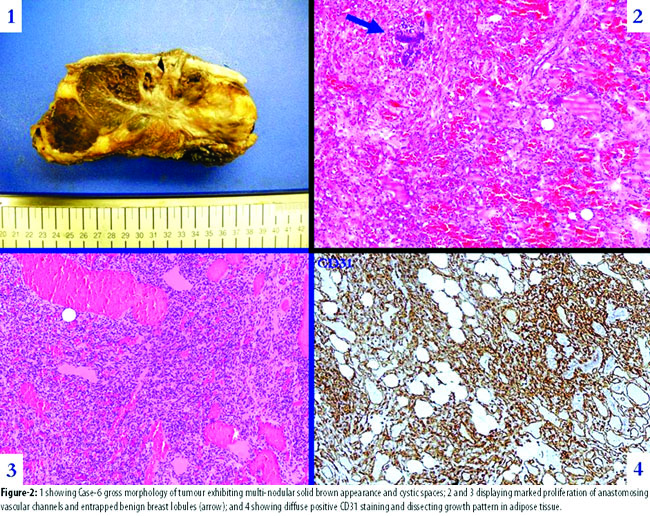
showing multiple cystic spaces filled with blood clots, measuring 11x10.5x7cm. Right breast lump composed of two nodules of 4 and 1.5cm each and the largest nodule of 9.5cm size, showing more or less the same gross morphologic picture.
Microscopy revealed an infiltrating neoplastic lesion composed of variably-sized anastomosing vascular channels lined by plump endothelial cells with areas of haemorrhage and focal necrosis. In some areas, solid proliferation of the tumour cells with small vascular lumina formation was noted. The tumour cells showed moderate amount of eosinophilic and vacuolated cytoplasm and round to oval nuclei with coarse chromatin and prominent nucleoli in few areas. Scattered mitotic figures were also noted (Figures-2-2 and 2-3). The tumour was only located in the breast and there was no skin involvement. The case was diagnosed as well-differentiated angiosarcoma (Figure 2-4) with bilateral involvement.
Case-7
A 17-year-old female underwent a Tru-cut biopsy for a mass in her right breast. The material was scanty and showed vascular proliferation along with few atypical cells and, therefore, it was non-diagnostic overall. A repeat biopsy was asked for before a major surgery, but, instead, the clinician decided to go for a simple mastectomy due to strong clinical suspicion of malignancy. The mastectomy specimen showed a partly solid, partly cystic, dark brown tumour with irregular margins and extensive haemorrhage, measuring 12x11x4cm. The cystic areas were filled with blood clots. On histology, the tumour was composed of irregular vascular channels lined by plump endothelial cells with nuclear pleomorphism and hyperchromasia. In certain areas, solid spindle cell proliferation was noted. The tumour cells were strongly positive for CD31. It was labelled as moderately differentiated angiosarcoma.
Results
Specimens including both lumpectomy and mastectomy were received in 10% buffered formalin and were processed routinely. Immunohistochemical analysis was performed on the formalin-fixed, paraffin-embedded tissue using the streptavidin-biotin complex with diaminobenzidine (DAB) as chromogen. One or more of the following antibodies were used after microwave antigen retrieval: Cytokeratin AE1/AE3 (CK AE1/AE3, Dako, Germany, prediluted); CD31 (Dako, Germany, 20:1000); CD34 (Dako, Germany, 10:1000); Factor VIII (Dako, Germany, 20:1000); CD68 (Dako, Germany, 10:1000); and Epithelial Membrane Antigen (EMA, Dako, Germany, 5:1000).
The ages of the patients ranged from 16 to 74 years with a median of 32 years. The tumour was bilateral at presentation in one case. The size of the tumours ranged from 1.6 cm to 11cm. In two cases, prior history of infiltrating ductal carcinoma followed by surgery and chemoradiotherapy was provided, which later presented with arm swelling. In all cases, one or more vascular markers including CD31 or CD34 were diffusely positive in tumour cells.
Discussion
Primary soft tissue sarcomas are malignant tumours arising from the connective tissue within the breast. They can arise de novo (primary) or as a consequence of treatment of an epithelial breast cancer (secondary).3 As with other non-breast soft tissue sarcomas, primary breast sarcomas are histologically heterogeneous. In general, fibrosarcomas, angiosarcomas, malignant fibrous histiocytomas (MFH), phyllodes tumour and myxoid/round cell liposarcomas comprise the major histological subtypes.4 In all the subtypes, angiosarcoma is the commonest sarcoma affecting the breast parenchyma.
Although the aetiology of most soft tissue sarcomas remains unknown, angiosarcoma of the breast has increasingly been associated with prior use of breast external beam radiation therapy and with lymphoedema that occurs after surgery, with or without radiation treatment for primary breast cancer. A study reported the observation that angiosarcoma constitutes more than 50% of all the sarcomas identified in patients previously treated with radiation therapy, but only 20% of sarcomas identified in patients who had not been previously treated with radiation therapy.5
Literature search revealed that patients of secondary angiosarcoma, whether resulting from lymphoedema or post-radiation, were significantly older than patients who had primary or de novo tumours;6 a similar finding was observed in this series.
Because of the rarity and the uncommon deceptively benign histological appearance, angiosarcomas of the breast are often misinterpreted as benign lesions at initial biopsies. Therefore, it is necessary to perform a surgical biopsy and an immunohistochemical analysis to establish the diagnosis of primary angiosarcoma of the breast. However, an accurate preoperative diagnosis may be difficult, even with the aid of fine-needle aspiration cytology (FNAC) and biopsy. Both mammogram and ultrasound tend to be non-specific, like with ill-defined masses or skin thickening. Although macroscopically the tumour is well-circumscribed, there may be foci of invasion in the surrounding breast tissue composed of intricate vascular channels surrounding and invading the breast lobules.7
Immunohistochemical analysis is an important adjunctive procedure in the diagnosis of angiosarcoma, particularly for poorly differentiated forms in which vascular channel formation is difficult to identify. Angiosarcomas express (to a greater or lesser degree) the usual vascular antigens, including von Willebrand factor, CD31, and CD34. Although von Willebrand factor is the most specific of the vascular markers, it is also the least sensitive, often present in a few angiosarcomas as weak focal staining. On the other hand, CD31 combines relative specificity with excellent sensitivity, and it is positive in approximately 90% of the angiosarcomas of all types. Cytokeratin is present in about one-third of soft-tissue angiosarcomas, particularly the epithelioid subtype, reflecting the fact that cytokeratin cannot be used as an absolute discriminant between angiosarcoma and carcinoma.8
Until recently it was considered that the histological grade of the tumour in primary mammary angiosarcoma plays a pivotal role in predicting patients\\\' prognosis.7 However, in more recent papers, the histological grade of the angiosarcoma showed no correlation with the likelihood of local recurrence, distant metastasis and death.8
Conclusion
Angiosarcoma of the breast in radiation therapy-naïve patients is a rare disease that arises chiefly in younger women. However, in view of increasing use of adjuvant external-beam radiation therapy for breast cancer treatment over the past 15 years, the incidence of soft-tissue sarcoma may increase in the future. Attention to post-irradiation skin lesions and timely diagnostic interventions including biopsies are, therefore, encouraged.
References
1. Adem C, Reynolds C, Ingle JN, Nascimento AG. Primary breast sarcoma: clinicopathologic series from the Mayo Clinic and review of the literature. Br J Cancer 2004; 91: 237-41.
2. Rosen PP. Rosen\\\'s Breast Pathology. 3rd ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins 2009; pp 918-53.
3. Blanchard DK, Reynolds C, Grant CS, Farley DR, Donohue JH. Radiation-induced breast sarcoma. Am J Surg 2002; 184: 356-8.
4. Sher T, Hennessy BT, Valero V, Broglio K, Woodward WA, Trent J,et al.Primary angiosarcomas of the breast. Cancer 2007; 110: 173-8.
5. Yap J, Chuba PJ, Thomas R, Aref A, Lucas D, Severson RK, et al. Sarcoma as a second malignancy after treatment for breast cancer. Int J Radiation Oncol Biol Phys 2002; 52: 1231-7.
6. Cafiero F, Gipponi M, Peressini A, Queirolo P, Bertoglio S, Comandini D, et al. Radiation-associated angiosarcoma: diagnostic and therapeutic implications - two case reports and a review of the literature. Cancer 1996; 77: 2496-502.
7. Zhou SA, Wei H, Ding K. A Rare Case of Metachronous Bilateral Angiosarcoma of the Breast. Breast Care (Basel) 2009; 4: 405-7.
8. Muzumder S, Das P, Kumar M, Bhasker S, Sarkar C, Medhi K, et al. Primary epithelioid angiosarcoma of the breast masquerading as carcinoma. Curr Oncol 2010; 17: 64-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: