
Shahbano Syed ( Dr. Ishratul Ebad Khan Institute of Oral Health Sciences, DUHS, Bahria Dental College, Karachi. )
Sobia Bilal ( Dr. Ishratul Ebad Khan Institute of Oral Health Sciences, DUHS, Bahria Dental College, Karachi. )
Narendar Dawani ( Dr. Ishratul Ebad Khan Institute of Oral Health Sciences, DUHS, Bahria Dental College, Karachi. )
Kulsoom Rizvi ( Community Dentistry Department, Bahria Dental College, Karachi. )
May 2013, Volume 63, Issue 5
Original Article
Abstract
Objective: To evaluate the dental anxiety levels and to assess its correlation with self-assessed dental status and treatment needs of patients.
Methods: The study was conducted at the Out Patient Department of Dr. Ishrat-ul-Ebad Khan Institute of Oral Health Sciences, Karachi. Using non-probability quota sampling, the study included the first 32 patients between 18 and 35 years of age, visiting the facility. Over a period of one month (22 working days) 704 patients comprised the study population. They were interviewed using a structured questionnaire to self-assess their dental anxiety levels, oral health status and treatment needs. The data was analysed using SPSS 17.0 with descriptive frequencies and chi-square test.
Results: Of the total participants, 650 (92.32%) patients provided consent. Average dental anxiety scale score was 12.46, representing high anxiety score. There were 174 (26.8%) smokers; only 234 (36%) had visited a dentist less than a year ago; 385 (59.2%) considered their dental health to be satisfactory; 306 (47.1%) thought of their treatment needs to be \\\'little\\\'; 222 (34.2%) brushed their teeth twice daily. Dental anxiety was statistically significant with treatment needs and dental status. Relation of tooth-brushing with last dental visit and treatment needs was also found to be significant.
Conclusion: A high level of dental anxiety was observed among the study population. The dental professionals should seek ways to help dentally anxious individuals.
Keywords: Dental anxiety scale (DAS), Last dental visit, Self-assessed treatment needs, Oral health status. (JPMA 63: 614; 2013).
Introduction
Oral disease burden is an unsolved global problem. Oral ailments include dental caries, periodontal diseases, edentoulousness, oral cancers and human immunodeficiency virus (HIV) related oral conditions which have a profound effect on overall general health.1 Dental diseases are detrimental to the quality of life from childhood through old age. They may have a deep impact on the self-esteem, eating ability as well as nutrition of an individual. Oral diseases are often associated with considerable pain, anxiety, and impaired social functioning; thereby leading to the impairment of daily routine at workplace and schools, resulting in loss of enormous working hours yearly.2 The increasing prevalence of dental diseases is associated with a number of barriers such as lack of access, poor awareness, limited resources and healthcare budgets as well as anxiety related to dental treatment.
Dental anxiety is a common condition among the masses worldwide and remains a barrier to dental care for a consistent proportion of the population.3 It is anticipated to begin from early childhood and may regress as age progresses. Several studies have estimated the prevalence of dental anxiety to range from approximately 5% to 30% in the general population depending on the population and case definition used.4 It has been established that subjects who are highly anxious have the greatest likelihood of avoiding dental treatment.5 A universal problem as it is, dental fear approximates in 25% of patients avoiding dental visits and treatments, and nearly 10% reach phobic levels of anxiety.5 The issue of dental anxiety needs to be probed for several possible reasons: (a) avoidance causes poor oral health and quality of life; (b) high levels of anxiety and phobia may impinge on the dentist-patient relationship, and may prevent proper dental treatment, and be a cause of intra-operative complications; and (c) the sympathetic response to stress caused by anxiety may yield harmful reactions, such as vasovagal syncope, hypertension, tachycardia and cardiovascular accidents.6 It has many endogenous and exogenous causes. Endogenous factors pertain to internal stressors, while exogenous causes may include conditioned fear (yielded by previous bad experiences), distrust of dental professionals, and somatic intra-operative reactions, which may affect dental experience.7
A clear correlation exists between dental fear, avoidance behaviour, and dental health problems. Dental fears and dental health problems are associated with other physical and mental health problems and, therefore, add to the financial burden on the healthcare system in the shape of lost working hours and growing treatment needs.8 Hence, from the public health point of view, individuals with dental anxiety or fear suffer considerably from impaired oral health related quality of life (OHRQoL), the extent of which is related to the magnitude of OHRQoL level. The perceptions of OHRQoL raises issues that are reflective of personal value, not only of the patients but also makes the discrepancies obvious between the patient\\\'s present behaviour and the goals which the patient himself wants to reach through his/her treatment.9
The present study aimed at evaluating the relationship between self-assessment of dental status, oral hygiene habits and the dental anxiety of adult patients. Another target was to assess the association of dental anxiety with factors such as age, gender and perceptions towards dental treatment needs as well as their dental status.
Introduction
Oral disease burden is an unsolved global problem. Oral ailments include dental caries, periodontal diseases, edentoulousness, oral cancers and human immunodeficiency virus (HIV) related oral conditions which have a profound effect on overall general health.1 Dental diseases are detrimental to the quality of life from childhood through old age. They may have a deep impact on the self-esteem, eating ability as well as nutrition of an individual. Oral diseases are often associated with considerable pain, anxiety, and impaired social functioning; thereby leading to the impairment of daily routine at workplace and schools, resulting in loss of enormous working hours yearly.2 The increasing prevalence of dental diseases is associated with a number of barriers such as lack of access, poor awareness, limited resources and healthcare budgets as well as anxiety related to dental treatment.
Dental anxiety is a common condition among the masses worldwide and remains a barrier to dental care for a consistent proportion of the population.3 It is anticipated to begin from early childhood and may regress as age progresses. Several studies have estimated the prevalence of dental anxiety to range from approximately 5% to 30% in the general population depending on the population and case definition used.4 It has been established that subjects who are highly anxious have the greatest likelihood of avoiding dental treatment.5 A universal problem as it is, dental fear approximates in 25% of patients avoiding dental visits and treatments, and nearly 10% reach phobic levels of anxiety.5 The issue of dental anxiety needs to be probed for several possible reasons: (a) avoidance causes poor oral health and quality of life; (b) high levels of anxiety and phobia may impinge on the dentist-patient relationship, and may prevent proper dental treatment, and be a cause of intra-operative complications; and (c) the sympathetic response to stress caused by anxiety may yield harmful reactions, such as vasovagal syncope, hypertension, tachycardia and cardiovascular accidents.6 It has many endogenous and exogenous causes. Endogenous factors pertain to internal stressors, while exogenous causes may include conditioned fear (yielded by previous bad experiences), distrust of dental professionals, and somatic intra-operative reactions, which may affect dental experience.7
A clear correlation exists between dental fear, avoidance behaviour, and dental health problems. Dental fears and dental health problems are associated with other physical and mental health problems and, therefore, add to the financial burden on the healthcare system in the shape of lost working hours and growing treatment needs.8 Hence, from the public health point of view, individuals with dental anxiety or fear suffer considerably from impaired oral health related quality of life (OHRQoL), the extent of which is related to the magnitude of OHRQoL level. The perceptions of OHRQoL raises issues that are reflective of personal value, not only of the patients but also makes the discrepancies obvious between the patient\\\'s present behaviour and the goals which the patient himself wants to reach through his/her treatment.9
The present study aimed at evaluating the relationship between self-assessment of dental status, oral hygiene habits and the dental anxiety of adult patients. Another target was to assess the association of dental anxiety with factors such as age, gender and perceptions towards dental treatment needs as well as their dental status.
Patients and Methods
The analytical study was conducted from October 2011 to March 2012 and included adults attending the OPD of Dr. Ishrat-ul-Ebad Khan Institute of Oral Health Sciences, a public dental facility. A non-probability quota sampling technique was used for the study purpose i.e. first 32 patients fitting the defined age-bracket of 18-35 years and visiting the dental OPD were asked to participate in the interview-based study. This enrolment procedure was followed for a period of one month (five working days in each week). Thus, a total 704 patients were approached to respond to the questionnaire.
The evaluation of dental anxiety can be performed with a variety of scales/instruments/methods available. However, Corah\\\'s Dental Anxiety Scale (DAS) is the most widely used.10 DAS is a reliable, simple and valid tool. A validated questionnaire was used to collect the data, which consisted of questions on the self-assessment of dental status and frequency of tooth-brushing habits along with Corah\\\'s DAS questionnaire to assess dental anxiety.10 Ethical Approval was obtained from the Dean of the institute and the respective (OPD) heads. Consent was also obtained from the subjects prior to the collection of data, and complete anonymity and confidentiality were assured. The interviews were conducted during the OPD hours; starting from 9:00am till 1:00pm five days a week. The data was analysed using SPSS 17. Descriptive frequencies and Chi-square test were applied. Statistical significance was defined at p <0.05.
Result
The response rate was 92.32% as 650 of the 704 prospective subjects agreed to fill the questionnaire. Of them 313 (48.2%) were males and 337 (51.8%) were females (Table-1).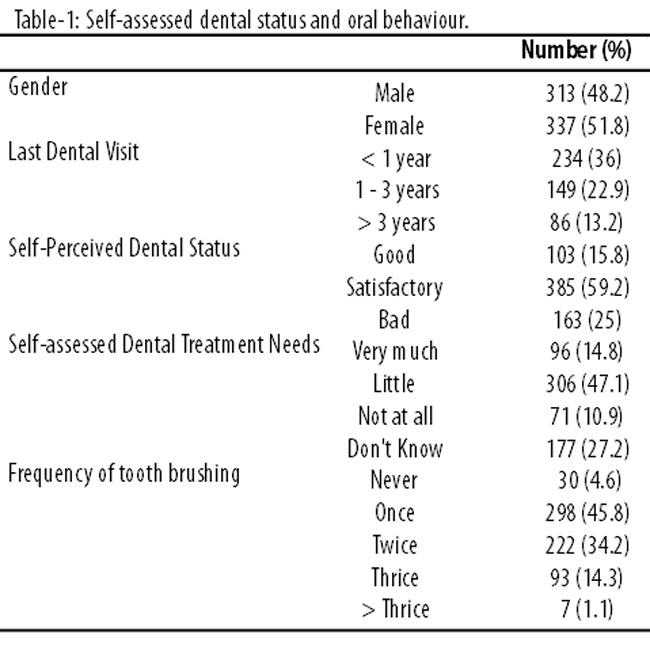
The mean age was 29.40±14.99 years.
Of the participants, 103 (15.8%) rated their dental status as \\\'good\\\', 385 (59.2%) rated \\\'satisfactory\\\'; and 163 (24.9%) rated it as \\\'bad\\\'. Of the total, 96 (14.8%) assessed their treatment needs to be \\\'very much\\\', 306 (47.1%) as \\\'little\\\', 71 (10.9%) as \\\'don\\\'t need it at all\\\', and 177 (27.2%) \\\'did not know\\\' whether they require any dental treatment. Only 298 (45.8%) brushed their teeth once daily; 222 (34.2%) brushed twice daily; while 30 (4.6%) had never brushed their teeth.
The average DAS score was calculated to be 12.46±3.2. When results were compared with gender, males were found to be less anxious compared to the females, though the difference was not significant (p< 0.675).
There was statistically significant correlation among self-assessed dental treatment needs and the level of anxiety of the study population (p<0.004). Similar significant association was observed between dental status of the individuals and their level of anxiety (p<0.016) (Table-2).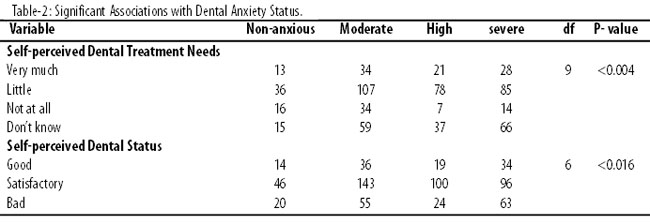
Statistically significant correlation was also found between tooth-brushing frequency and last dental visit (p <0.001), as well as treatment needs of the patients (p <0.001) (Table-3).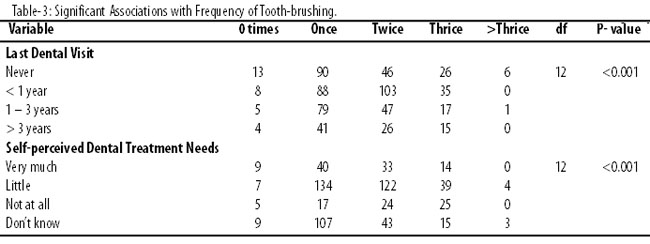
Discussion
Human psychology and behavioural sciences are gaining its impact in dental education and clinical practices. As more and more percentage of patients have fear regarding their dental health and treatment needs, such actions lead to treatment delay and avoidance behaviour towards oral care and health in general. Hence, assessment of anxiety levels and treatment needs may be very helpful for the provision of good quality dental care, better management and psychological uplifting of an individual. Behavioural modification can play a vital role not only in disease prevention, but also help to streamline adequate oral hygiene habits and regular dental visit compliance among populations.11
Corah\\\'s DAS is a renowned and recognised scale as it is validated, simple, reliable and reproducible as well as focussed on measuring dental fear in the most prompt way. It has proven efficacy for both children and adults alike. It asks four questions related to dental setting, each having five responses. The sum of the responses ranges from four to 20; a score of 9-12imply moderate anxiety; score of 13-14 signify anxious patients; while a score of 15 and above indicates phobic levels of dental anxiety.10
A high DAS score not only corresponds to low literacy rate and lack of awareness among those attending the public dental setting, but also reflects sample variability, cultural differences across nations and within.6 Many myths and false perceptions regarding dental care exist in the subcontinent; these may also perpetuate the results.12 The treatment being offered increases the likelihood of patients to be more anxious; for example before going for dental surgery.6
Young patients are comparatively more anxious than their older subjects, as they have been exposed to some form of dental treatment by this age. Females are more apprehensive towards dental treatment, exhibiting more anxiety compared to their male counterparts. An individual\\\'s personality is another factor predicting those who will develop high levels of dental anxiety and those who will not. Anxiety can be a conditioned process or a learned response that an individual has experienced in life.13
Levels of anxiety may change as a function of experience; may it be medical, dental or any life incident.7 Invasive treatments and chronic illnesses concerned with dentistry may raise anxiety intensity. Co-existence of ailments foster disease-related anxiety in some individuals.6
Subjects who declare to have had no dental checkup in the past year have high levels of DAS compared to those who did visit their dentist in the past year. Hence, time interval since the last checkup and the frequency of cancelled appointments is a significant predictor of high DAS scores. These concepts coincide with aversion to care, along with previous negative experiences,14 pains during the last dental visit,15 and unpleasant remarks by the dentist all seem to relate to anxiety.16
Preventive oral health behaviours and hygiene practices have several influential factors, like patients\\\' motivation, his/her attitude, and differences related to cultural and geographical variants.6 So, healthy practices towards oral hygiene may not be enough to reduce the anxiety levels, but early childhood education have been found to have a positive impact on dental anxiety and improving dental followup in the long run. Other means of management of dentally anxious patients include proper pain control strategies, behaviour modification, and consideration of patient holistically with access to sedation, if necessary. Inclusion of behavioural sciences and integration of ethics in dental education may turn out to be very helpful for upcoming dental graduates.17
Self-assessment of oral health status provides an opportunity to determine dental health standing not only at an individual level, but for populations as well. This means of oral health assessment is more popular among those who are shy of clinical examination, for reason of either cost or fear of embarrassment of their oral condition.18 It is a common observation that regular dental visits are assist early diagnosis, timely treatment and long-term prevention.19 The present study results indicate that most of the patients consider their dental health needs to be \\\'little\\\', and dental status to be \\\'satisfactory\\\'.
Tooth-brushing is the most primary and basic means of oral hygiene aid used in history. It is also the best way of mechanical plaque removal and should commence as soon as the child\\\'s first tooth erupts. The present study indicates that less than 50% of the population brushes once daily, while only 34% brushes twice. However, no significant difference was observed between genders towards their brushing habits, contrary to other studies which claim that females are more hygiene-conscious.20 But frequency of tooth-brushing was found to be significantly associated with the study populations\\\' self assessed treatment needs and their last dental visit.
Regular dental checkups are recommended globally for children and adults alike. But such a recommendation should be tailored to the needs of each patient depending on the assessment of disease level and risks involved. The shortest interval suggested for all patients is of three months and the longest of 12 months for patients younger than 18 years. Long interval is for those individuals who have shown to maintain their oral health in good shape. However, such compliance was relatively low in the current study population. Only a quarter of population had its last dental visit a year ago, and there were an unfortunate handful who never had a dental visit in their entire life. Such a high level of those having limited compliance of oral hygiene practices would not have occurred if the basics of oral care would have been included in our educational system through oral health promotion and education. Oral health promotion should also be carried out through media in the form of public service messages. The promotion should be carried out with the help of community healthcare workers. Oral care should not be treatment-oriented. In fact, a more holistic approach should be adopted by including preventive and promotive strategies.21
The current study had a few limitations in terms of reliance on subjective evaluation of self rather than a true picture ascertained through clinical assessment by a professional. Another limitation is of the method chosen for sampling. As it was a public dental setting, the majority of study subjects were of low social strata and little educational background, hence exclusion of people from other social strata may lead to under-representation of the general population. However, the available data helps to assess the perceptions of the majority. The data should, therefore, be interpreted with extreme caution so as to minimise overestimation of hygiene practices and underestimation of dental needs, as this gives an indirect magnitude of oral health needs of a society. Hence, this should help focus on those who are in need of preventive services the most but get them the least. The information attained through this study can be used as baseline data for policy-making and innovative preventive programmes can be initiated and established.
Conclusion
Dental anxiety is a public health problem as it affects not only the individual, but community as a whole. Its prevention is possible as effective treatments exist such as creating awareness and educating society.
References
1. Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C. The global burden of oral diseases and risks to oral health. Bulletin of the World Health Organization. 2005; 83: 661-9.
2. Kelly M, Steele J, Nuttall N, Bradnock G, Morris J, Nunn J, et al. (1998) Adult dental health survey. Oral health in the United Kingdom. London: The Stationery Office, 2000.
3. Corah NL, Gale EN, Illig SJ. Assessment of a dental anxiety scale. J Am Dent Assoc 1978; 97: 816-9.
4. Thomson WM, Dixon GS, Kruger E. The West Coast Study II: Dental anxiety and satisfaction with dental services. NZ Dent J 1999; 95: 44-8.
5. Moore R, Brødsgaard I, Mao TK, Kwan HW, Shiau YY, Knudsen R. Fear of injections and report of negative dentist behavior among Caucasian, American, and Taiwanese adults from dental school clinics. Community Dent Oral Epidemiol 1996; 24: 292-5.
6. Facco E, Zanette G, Manani G. Italian version of Corah\\\'s Dental Anxiety Scale: Normative Data in Patients undergoing Oral Surgery and relationship with the ASA Physical Status Classification. Anesth Prog 2008; 55: 109-15.
7. Liddell A, Locker D. Changes in levels of dental anxiety as a function of dental experience. Behav Modif 2000; 24: 57-68.
8. Hollister MC, Weintraub JA. The association of oral status with systemic health, quality of life, and economic productivity. J Dent Educ 1993; 57: 901-12.
9. Mehrstedt M, John MT, Tonnies S, Micheelis W. Oral health-related quality of life in patients with dental anxiety. Community Dent Oral Epidemiol 2007; 35: 357-63.
10. Corah NL. Development of a dental anxiety scale. J Dent Res 1969; 48: 596.
11. Honkala E. Oral health promotion with children and adolescents. In: Schou L, Blinkhorn AS (eds): Oral Health Promotion. New York: Oxford University Press, 1993, pp 169-87.
12. Singh SV, Tripathi A, Akbar Z, Chandra S, Tripathi A. Prevalence of dental myths, oral hygiene methods and tobacco habits in ageing North Indian rural population. Gerodontology 2012; 29: 53-6.
13. Peretz B, Efrat J. Dental anxiety among young adolescent patients in Israel. Int J Paediatr Dent 2000; 10: 126-32.
14. Sohn W, Ismail AI. Regular dental visits and dental anxiety in an adult dentate population. J Am Dent Assoc 2005; 136: 58-66.
15. De Jongh A, Fransen J, Oosterink-Wubbe F, Aartman I. Psychological trauma exposure and trauma symptoms among individuals with high and low levels of dental anxiety. Eur J Oral Sci 2006; 114: 286-92.
16. Maggirias J, Locker D. Five-year incidence of dental anxiety in an adult population Community Dent Health 2002; 19: 173-9.
17. Berggren U. Long-term management of the fearful adult patient using behavior modification and other modalities. J Dent Educ 2001; 65: 1357-68.
18. Gilbert AD, Nuttall NM. Self-reporting of periodontal health status. Br Dent J 1999; 186: 241-4.
19. Axelsson P, Nystrom B, Lindhe J. The long term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. J Clin Periodontol 2004; 31: 749-57.
20. Bamigboye O, Akande TM. Oral Hygiene Status of Students in Selected Secondary Schools in Osogbo, Nigeria. Nigesrian Medical Practitioner 2007; 51: 71-5.
21. Behbehani JM, Scheutz F. Oral health in Kuwait. Int Dent J 2004; 54 (Suppl 1): 401-8.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: