
Sirajus Salekeen ( Medical Unit III, Civil Hospital, Dow University of Health Sciences, Karachi, Pakistan. )
Khalid Mahmood ( Medical Unit III, Civil Hospital, Dow University of Health Sciences, Karachi, Pakistan. )
Iftikhar Haider Naqvi ( Medical Unit III, Civil Hospital, Dow University of Health Sciences, Karachi, Pakistan. )
Mirza Yousuf Baig ( Postgraduate Trainee, Civil Hospital, Dow University of Health Sciences, Karachi, Pakistan. )
Syed Tehssen Akhter ( Medical Unit III, Civil Hospital, Dow University of Health Sciences, Karachi, Pakistan. )
Amanullah Abbasi ( Medical Unit III, Civil Hospital, Dow University of Health Sciences, Karachi, Pakistan. )
May 2013, Volume 63, Issue 5
Original Article
Abstract
Objective: To assess the clinical course, complications and predictors of mortality in reducing the consequent morbidity and mortality in patients with tuberculous meningitis.
Methods: A prospective study was carried out at Civil Hospital Karachi from January 2009 to January 2011. Fifty-two confirmed cases of tuberculous meningitis were included. The entire clinical course with complications and predictors of mortality were assessed. Data was analyzed using SPSS version 17.0.
Results: The mean age of the patients was 36.29±16.7 years with an equal gender distribution. The presenting complaints were fever 51 (98.1%), neck-stiffness 44 (84.61%), and altered level of consciousness 40 (76.9%), headache 31 (59.6%), vomiting 19 (36.5%) and focal weakness 10 (19.2%). Among CNS signs, 47 (90.4%) patients had signs of meningeal irritation, 14 (26.9%) had cranial nerve palsies with abducent nerve being the most commonly involved cranial nerve (25%). Mean GCS was 11.4±2.9 and most of the patients presented with medical research council Stage 2 of tuberculous meningitis (which is minimally altered level of consciousness with minor focal neurological signs). Overall mortality was 21.1%. Univariate analysis revealed old age; advanced stage of tuberculous meningitis, serum sodium < 125 mmol/l, TLC >9000/mL development of hydrocephalus and use of mechanical ventilation as major predictors of mortality.
Conclusion: Tuberculous meningitis is a frequently reported problem in our part of the world. Hydrocephalus along with other sequelae are common complications. All patients should be assessed for the presence of risk factors affecting mortality of the disease.
Keywords: Extra pulmonary tuberculosis, Tuberculous meningitis, Central nervous system tuberculosis, Tuberculoma. (JPMA 63: 563; 2013).
Introduction
Tuberculosis captain of death with its various forms is still a challenging problem in Pakistan. According to WHO Global Health Observatory Database, tuberculosis accounts for 373 cases per 100,000 population in Pakistan.1 In Pakistan mortality rate of tuberculosis is about 38 per 100,000 deaths in HIV negative individuals.2 This brings Pakistan among the top 35 countries with the highest mortality rates in the world. Central nervous system (CNS) tuberculosis is the third most common manifestation of extra-pulmonary tuberculosis as evidenced in a local study.3 Among CNS tuberculosis, tuberculous meningitis (TBM) is the commonest presentation with high morbidity and mortality.4,5 Most of the cases present late to the hospital as in the initial stage 1 of TBM the symptoms are non-specific.
In 1997, TBM was the 5th most common form of extra pulmonary tuberculosis, accounting to 5.2% of all such cases.6 TBM accounts for 2.1% of paediatric cases and 9.1% of adult cases.7 Local study conducted by Malik et al,5 described a high mortality of 23.3%
It is evident from the above data that complete understanding of the clinical course, early assessment for complications of TBM is mandatory for prompt institution of the treatment to prevent complications and avoid high mortality.
Hence, this study was conducted to observe the clinical course, complications and to analyze predictors of mortality in patients of TBM at Civil Hospital Karachi, Pakistan.
Patients and Methods
This is a prospective study conducted in Civil Hospital Karachi, Pakistan; which is one of the largest public sector tertiary care hospital in Karachi. Fifty-two patients of TBM from various medical units of Civil Hospital Karachi, Pakistan were selected over a period of two years. The evidence of radiographic features of pulmonary tuberculosis, enhancement of meninges or basal cisterns on imaging supported whereas the cerebrospinal fluid (CSF) analysis confirmed the diagnosis of TBM. Acid fast bacilli (AFB) staining with culture, polymerase chain reaction (PCR) for mycobacterium tuberculous, other necessary ancillary investigations like lymph node biopsy in an accessible part and MRI were also carried out in selected patients. Fungal staining was also done to rule out fungal meningitis in equivocal cases. During their stay in the medical ward all the patients were assessed for complications and managed accordingly.
A follow-up protocol was devised and all the patients and their relatives were counseled about periodic follow-ups. Maximum follow-up period was one year. Outcome was determined at the cessation of follow-up, in terms of complete recovery or recovery with residual disability and mortality.
In the study protocol all confirmed cases of TBM, above 18 years, either sex and after informed consent were included. Patients under 18 years of age or those not consenting for participation in the study were excluded. Patients having central nervous system (CNS) pathologies which can mimic TBM like bacterial meningitis, viral encephalitis, subarachnoid haemorrhage, intra-cranial bleed, cerebral malaria, enteric fever, stroke or epilepsy were excluded.
A detailed history of illness was obtained including family history of tuberculous contact, age, gender, previous history of default of anti tuberculous therapy (ATT). A default was taken as a case who had quit ATT after confirmation of TB anywhere in the body. A through clinical examination both general physical and systemic especially nervous system was done in all patients. All routine investigations like complete blood count (CBC), liver function tests ( LFTs), random blood sugar ( RBS), urea, creatinine, electrolytes (UCE), Mantoux test (MT), chest X-ray, and fundoscopy were carried out. Computed tomographic (CT) brain scan with contrast and CSF analysis with AFB staining and cultures were also carried out. The necessary ancillary investigations like lymph node biopsy in an accessible part and MRI were carried out in only selected patients.
On the basis of clinical presentation, patients of TBM were classified into 3 clinical stages according to British Medical Research Council:6
Stage 1 includes early nonspecific symptoms and signs, such as apathy, irritability, headache, malaise, fever, anorexia, nausea, and vomiting, without impaired level of consciousness. Stage 2 is altered consciousness without coma or delirium but with mild focal neurological deficits. Symptoms and signs of meningism and meningitis may be present, in addition to focal neurological deficits, isolated cranial nerve palsies, and abnormal involuntary movements. In stage 3 patient is in stupor or coma, with severe neurological deficits, seizures, posturing and abnormal movements may be present.
For analysis of fifty-two patients data, statistical package version 17.0 was used.. Univariate analysis was done to assess the factors which affected mortality in TBM and a direct logistic regression model was used to assess the individual risk factors.
Results
A total of 52 patients were included in the study from January 2009 to December 2010 over a period of two years. The mean age of the patients was 36.29±16.7 years. There were equal number of males and females.
Forty-seven patients (90.4%) were admitted through emergency department and 5 (9.6%) through out-patient department. Fever was found to be the most common symptom at presentation seen in 51 (98.1%) patients, followed by neck-stiffness in 44 (84.6%) cases and altered level of consciousness in 40 (76.9%) cases (Table-1).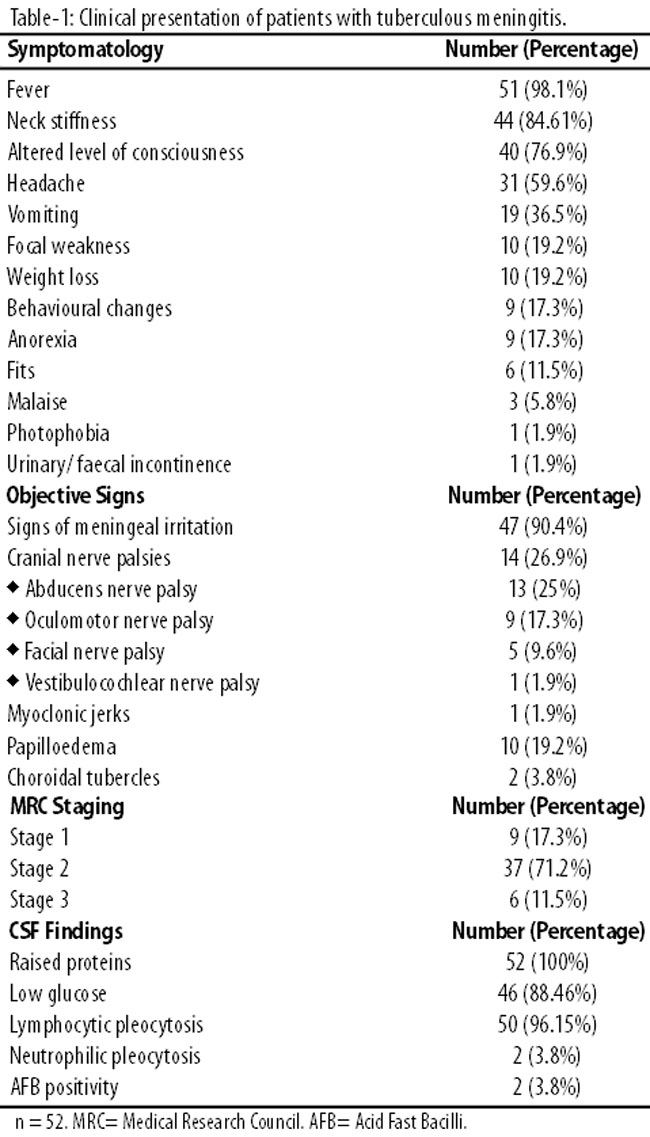
The duration of admission varied from 2 to 120 days with a mean of 30.08±31.177 days. Seven patients (13.5%) gave a past history of tuberculosis. Fourteen patients (26.9%) reported history of contact with tuberculous patient. Seventeen patients (32.69%) were found to have tuberculous infection affecting other organs at presentation. Of these pulmonary tuberculosis was found to be the most common 15/52 (28.85%). Other sites included extrameningeal CNS TB (9.6%), disseminated (9.6%), abdominal (3.8%), lymph node (1.9%), spinal (1.9%), and others (3.8%).
Out of 52 patients, 4 (7.7%) had diabetes, 4 (7.7%) had hypertension while 1 (1.9%) patient was pregnant. Two (3.8%) patients had history of delivery within a two week period at presentation. One (1.9%) patient had chronic kidney disease. Four (7.69%) patients had already been prescribed ATT in recent past due to tuberculosis elsewhere in the body but had either quit ATT after resolution of symptoms or due to poverty issues.
The clinical examination findings with the stage of presentation and CSF picture are summarized in Table-1. The mean Glasgow Coma Scale at presentation was found to be 11.42±2.913. The patients were classified into stage I (9/52 = 17.3%), stage II (37/52 = 71.2%) and stage III (6/52 = 11.5%). Radiography revealed infiltrates in 11 (21.2%) patients, miliary pattern in 2 (3.8%), cavity in 1 (1.9%) and hilar lymphadenopathy in 1 (1.9%) patient. Twenty-one (44.1%) patients were found to have haemoglobin of less than 11g/dl and the mean haemoglobin was found to be 10.2g/dl. Erythrocyte sedimentation rate (ESR) >20mm/hour was found in 40 (76.92%) patients with a mean ESR of 35.79±18.7mm/hour. Hyponatraemia (serum sodium level <135 mmol/l) was present in 31 (59.61%) patients.
CT scan was done in 44 (92.4%) patients. MRI was done in eleven patients upon the recommendation of radiologists whenever CT scan was inconclusive. CT scan and MRI findings are summarized in Table-2.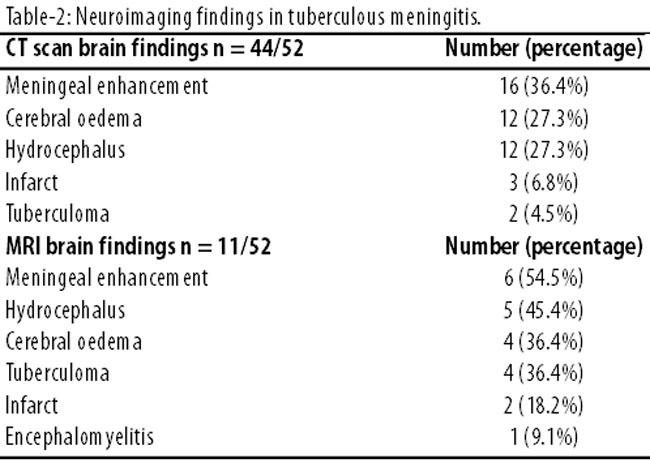
ATT with adjunctive steroids was started in all patients. During the course of stay 13 (25%) developed hydrocephalus, out of which 10 (19.2%) were of communicating type while 3 (5.8%) patients were non-communicating type. Among these patients, ventriculo-peritoneal shunt had to be placed in 8 (15.4%) while the rest were managed conservatively. Four (7.7%) patients developed drug-induced hepatitis. One patient developed ethambutol induced optic neuritis. Two patients developed aspiration pneumonia while in deep coma while five had to be mechanically ventilated. Mean duration of stay in hospital was 17±8.325 days (range: 2-40 days).
During overall hospital stay, eight patients died and three patients left against medical advice. Remaining forty-one patients were discharged on ATT. Two of these were lost to follow-up. Two patients developed hydrocephalus after discharge from the hospital, were re-admitted and ventriculoperitoneal (VP) shunt was placed. One of these patients developed severe intolerance to ATT and had to be switched to multiple second line agents. At the end of standard duration of treatment twenty-eight (53.8%) patients had complete recovery without residual defects. Eight (15.4%) had residual deficits including cranial nerve palsies in five and limb weakness in three. Death during follow-up was noted in three patients; one due to urosepsis and two due to complicated bed-sores and respiratory tract infections. Overall mortality was noted to be 21%.
Univariate analysis to assess the impact of "old age (age greater than or equal to 60 years)", "advanced stage (Stage 3 vs Stage 1 and 2)", "severe hyponatremia (serum sodium <125 mmol/l)", "raised total leucocyte count (greater than 9000 WBCs/ microlitre)", "development of hydrocephalus" and "use of mechanical ventilation" on mortality were assessed. The strongest predictor of mortality was found to be "use of mechanical ventilation" with an odds ratio of 25.54 at 95% CI. Other findings are summarized in Table-4.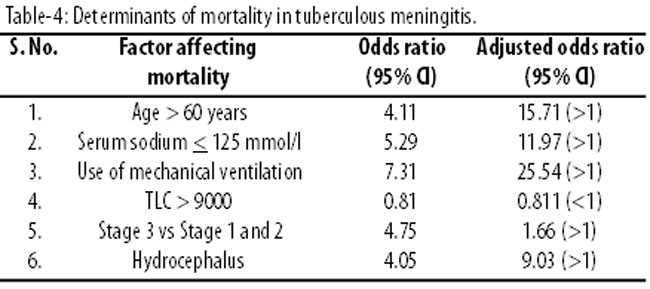
Discussion
Tuberculous meningitis has a highly variable presentation. It is difficult to diagnose in the early stage, and difficult to treat. It has high mortality and if left untreated, is almost fatal.8,9 Fifty-two cases were selected in this study.
Mean age of the patients was 36.29±16.7 years which is near to the results by Qureshi et al10 but higher than in earlier studies.4,5 This study also did not show any significant gender differences. Other studies4,5 have found a minor male predominance whereas Qureshi et al10 revealed a slight female preponderance. Past history of tuberculosis was found in 7 patients (14.9%) which is similar to Qureshi et al.10 Other studies revealed a very high percentage of positive past history (40% and 32.5%).4,5
Seventeen patients (32.69%) had concurrent tuberculosis elsewhere in the body. Most commonly involved site was pulmonary in fifteen (28.85%). These findings are also similar to other studies.4,5,10 Majority of the patients presented in stages 2 or 3 of TBM as classified by Research Medical Council. The delayed presentation of TBM appears to be multifactorial and probably reflects overall flaws in our health care system which includes poor primary health care, reduced awareness among both primary care physicians as well as poor population. Many of the patients also present from remote urban areas having false myths and believe in spiritual healing as well as traditional medicine. Further studies are needed on this subject to highlight the causes.
Most of the patients presented in stage 2 which is in accordance with most of the other studies.4,5
Anaemia in tuberculosis is attributed to erythropoiesis suppression due to inflammatory mediators. Analysis from this study revealed haemoglobin of less than 11 g/dl in twenty-one patients (44.1%) and a mean haemoglobin of 10.2±2.0g/dl. Other studies report a 31.9% prevalence of anaemia in TBM.11
Hyponatraemia was found to be the most common electrolyte abnormality associated with tuberculous meningitis in our study. Other studies have also reported the same. Hyponatraemia is attributed to the association of SIADH with TBM.12 Chest radiographs revealed findings consistent with pulmonary tuberculosis in fifteen patients (28.8%). Most commonly found abnormality was presence of infiltrates in 21.2%. Other studies report a higher frequency of infiltrates from 35 - 50%.4,5,10
CSF pleocytosis with predominant lymphocytes, increased proteins and reduced sugar was found in fifty patients. Two patients were however found to have neutrophilic pleocytosis. Evidence shows that atypical findings in CSF do not rule out tuberculous meningitis.10 AFB smear was found positive in two patients only (3.8%) which correlates well with other local studies.4,5 The reason for low yield may be the small quantity of CSF which is usually taken.
The findings of neuroimaging studies in our patients revealed the most common finding to be meningeal enhancement, usually basal. Most of other studies however have described hydrocephalus as the most frequent finding.13-18 MRI showed even more findings in cases where CT scan results were suspicious especially in case of meningeal enhancement or tuberculomas. In literature most of the hydrocephalus associated with TBM is non-communicating type but communicating hydrocephalus has been seen in upto 26.9% in some studies.15 However, studies from India report otherwise.16 To the best of our knowledge none of the local studies in Pakistan have reported the frequency of both types of hydrocephalus in TBM.4,5
Evidence has shown that steroids reduce mortality when administered as an adjunct to anti-tuberculous therapy.19-21 In our study all the patients were treated similarly. This study revealed an overall mortality of 21.1% in total with eight in-hospital deaths and three deaths during follow-up. Mortality in all local studies range from 20% to 25%4,5,10 while in studies abroad it ranges from 6.9% - 77%.8,9,22,23 This is probably due to the fact that tuberculosis is more common in our community and a high index of suspicion among our physicians in tertiary care setup for early detection of tuberculosis is required. Mortality rate of extra pulmonary TB is dependent on site, stage of disease, degree of resistance of mycobacterium and other factors. The referred studies where mortality was high is not due to their low index of suspicion but must be accounted by other factors like extensive disease, GCS state, critical care facilities for patients, multi drug resistant (MDR) or extreme drug resistant (XDR) cases and delayed presentation.
Regarding predictors of mortality, study by Queshi et al has revealed age > 60 years and use of mechanical ventilation to be the sole independent predictor of mortality.10 This study reveals use of mechanical ventilation to be the most determining factor of mortality in TBM.
Conclusion
Tuberculous meningitis is a frequently reported problem in our part of the world. Hydrocephalus along with other sequelae are common complications. Wherever suspected CT scan should be repeated for hydrocephalus and VP shunting planned if necessary to reduce hydrocephalus. Most common predictors of mortality include mechanical ventilation followed by advanced age and presence of hyponatraemia. All patients should be assessed for the presence of these risk factors to prognosticate outcome and to enhance management.
References
1. WHO. World Health Organization Global Health Observatory Database. Tuberculosis Cases Mortality and prevalence. (Online) 2011. (Cited 2011 April 10). Available from URL: http://apps.who.int/ghodata/?vid=510.
2. WHO. World Health Organization Global Health Observatory Database. Tuberculosis Cases Mortality and prevalence. (Online) 2011. (Cited 2011 April 10). Available from URL: http://apps.who.int/ghodata/?vid=510.
3. Chandir S, Hussain H, Amir M, Lotia I, Khan A J, Salahuddin N, Ali F. Extra-pulmonary tuberculosis: A retrospective review of 194 cases at a tertiary care hospital in Karachi. J Pak Med Assoc 2010; 60: 105-9.
4. Fazel P A, Makki KU, Haroon H, Soomro I B, Afzal U. Clinical spectrum and outcome of patients with tuberculous meningitis. Med Channel 2006; 12: 21-3.
5. Malik ZI, Ishtiaq O, Shah NH, Anwer F, Baqai HZ. Analysis and outcome of 30 patients with tuberculous meningitis. Pak J Med Res 2002; 41: 137-41.
6. Ramachandran TS. Tuberculous meningitis. (Online) 2011 March 29 (Cited 2011 April 17). Available from URL: http://emedicine.medscape.com/article/1166190-overview#a0156.
7. Nelson LJ, Schneider E, Wells CD, Moore M. Epidemiology of childhood tuberculosis in the United States, 1993-2001: the need for continued vigilance. Pediatrics 2004; 114: 333-41.
8. Heemskerk D, Day J, Chau TT, Dung NH, Yen NT, Bang ND, et al. Intensified treatment with high dose Rifampicin and Levofloxacin compared to standard treatment for adult patients with tuberculous meningitis (TBM-IT): protocol for a randomized controlled trial. Trials 2011; 12: 25.
9. Karstaedt AS, Valtchanova S, Barriere R, Crewe-Brown HH. Tuberculous meningitis in South African urban adults. Q J Med 1998; 91: 743-7.
10. Qureshi HU, Merwat SN, Nawaz SA, Rana AAK, Malik A, Mahmud MK, et al. Predictors of inpatient mortality in 190 adult patients with tuberculous meningitis. J Pak Med Assoc 2002; 52: 159-63.
11. Lee SW, Kang YA, Yoon YS, Um S, Lee SM, Yoo C, et al. The Prevalence and Evolution of Anemia Associated with Tuberculosis. J Korean Med Sci 2006; 21: 1028-32.
12. Singh BS, Patwari AK, Deb M. Serum sodium and osmolal changes in tuberculous meningitis. Indian Pediatr 1994; 31: 1345-50.
13. Etlik Ö, Evirgen Ö, Bay A, Yilmaz N, Temizöz O, Irmak H, et al. Radiologic and clinical findings in tuberculous meningitis. Eur J Gen Med 2004; 1: 19-24.
14. Bhargava S, Gupta AK, Tandon PN. Tuberculous meningitis - A CT study. British J Radiol 1982; 55: 189-92.
15. Sobri M, Merican JS, Nordiyana M, Valarmathi S, Al-Edrus SA. Neuroimaging features of tuberculous meningitis. Med J Malaysia 2006; 61: 36-40.
16. Rajshekhar V. Management of hydrocephalus in patients with tuberculous meningitis. Neurol India 2009; 57: 691.
17. Bullock MMR, Welcman JM. Diagnostic and prognostic features of tuberculous meningitis on CT scanning. J Neurol Neurosurg Psychiatr 1982; 45: 1098-101.
18. Villoria MF, Fortea F, Moreno S, Munoz I, Manero M, Benito C, Alarcon JJ. MR imaging and CT of Central Nervous System: Tuberculosis in patients with AIDS. Radiol Clin North Am 1995; 33: 805-20.
19. Thwaites GE, Bang ND, Dung NH, Quy HT, Oanh DTT, Thoa NTC, et al. Dexamethasone for the treatment of tuberculous meningitis in adolescents and adults. N Engl J Med 2004; 351: 1741-51.
20. Escobar JA, Belsey MA, Dueñas A, Medina. Mortality from tuberculous meningitis reduced by steroid therapy. Pediatrics 1975; 56: 1050-5.
21. Prasad K, Volmink J, Menon GR. Steroids for treating tuberculous meningitis. Cochrane Database Syst Rev 2000; 3:CD002244.
22. Kent SJ, Crowe SM, Yung A, Lucas CR, Mijch AM. Tuberculous meningitis: A 30 year review. Clin Infect Dis 1993; 17: 987-94.
23. Kilpatrick ME, Girgis NI, Yassin MW, Ella AE. Tuberculous meningitis — clinical and laboratory review of 100 patients. J Hyg (London) 1986; 96: 231-8.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: