
Naim-Ur-Rahman ( Division of Neurosurgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia. )
Abdulbakim Jamjoom ( Division of Neurosurgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia. )
Zain Alabedeen B. Jamjoom ( Division of Neurosurgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia. )
June 1997, Volume 47, Issue 6
Case Reports
Introduction
Ruptured intracranial aneurysm is a major public health problem afflicting approximately 28,000 Norih Americans eachyear and resulting in death or disability in 18,000 of these patients1, Vast improvements have been made in the operative results for ruptured aneurysms during the past 3 decades, but these have not reflected in a proportional improvement in ovtrall management results. In spite of all these surgical advances, the overall mortality and morbidity of ruptured aneurysm continues to be very high2. The reason why the improvement is minimal in the overall management result is that more than one-third of the patients with ruptured aneurysms are dead or disabled before they reach the hospital or become available for treatment1, Nothing can at present be done to save these patients who die quickly after aneurysmal rupture3. The factors responsible for this fatal outcome in majority of these patients included: ignorance of warning symptoms, initial misdiagnoses and late referral1. For any future improvements in the overall outcome of the patients with aneurysmal subarachnoid hemorrhage, one has to address to the subtle warning signs of the unruptured aneurysms. Recognition of atypical migraine as an important warning symptom of unruptured aneurysm may lead to their treatment in the pre- rupture stage, thus improving the overall results.
Case Report
Case 1
A 35-year old woman presented with a history of severe left orbital and hemicranial pain for 6 weeks. The pain was continuous and refractory to medical treatment. Left third nerve palsy was noted 2 days prior to admission. The patient had a history of migraine diagnosed 5 years previously, for which she had been treated with caffergot and propanadol. Examination revealed an alert patient in excellent health but bitterly complaining of left-sided headache. Except forthe left third nerve palsy, the neurological examination was normal’. An axial CT scan through the suprasellar region showed a small lobulated contrast-enhancing structure adjacent to the posterior clinoid process (Figure 1).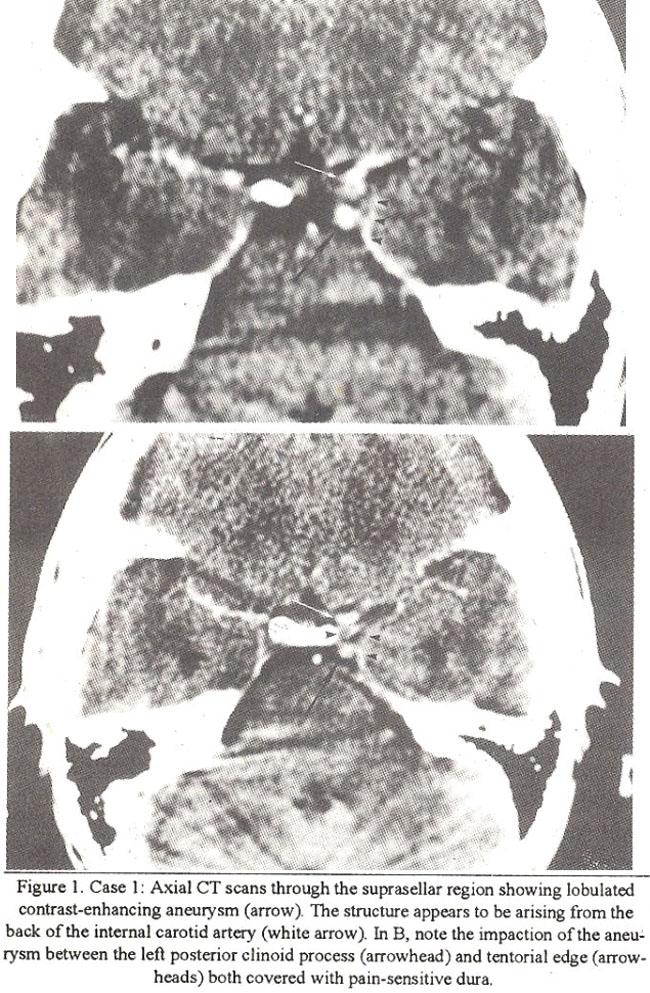
No blood was seen in the subarachnoid space. Left carotid angiogram (Figure 2) showed a posterior communicating artery aneurysm on the internal carotid artery. A weak saccule projected posteriorly from the fundus of the aneurysm (Figure 2).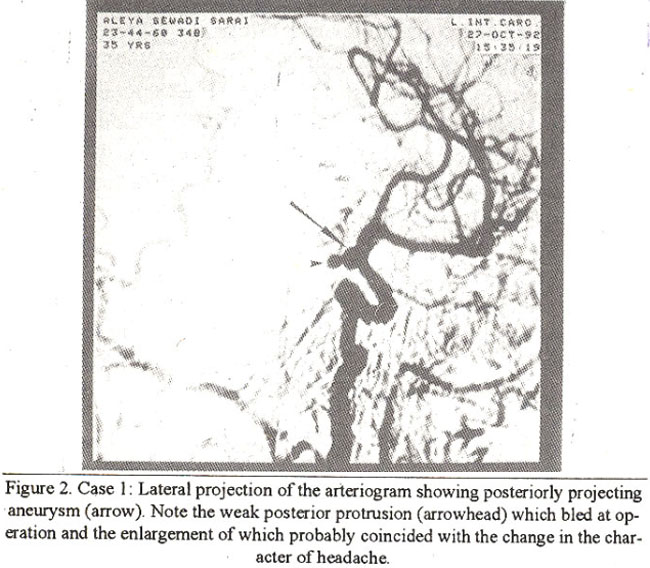
At operation, an unruptured internal carotid artery aneurysm medial to the edge of the tentorium was clipped (Figure 3).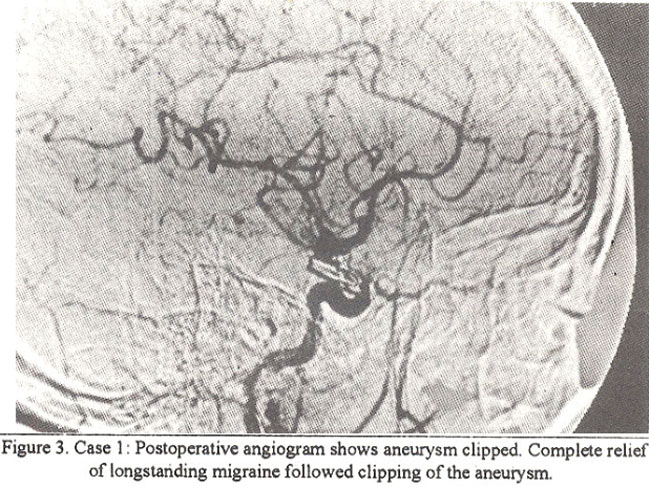
Notable operative findings included: (a) a tightly impacted aneurysm with a lobulated configuration, located medial to the tentorial edge; (b) a thin walled, angry-looking saccular protrusion from the fundus of the aneurysm that started leaking while arachnoid was being freed from the base of the aneurysm. Postoperative course and 3 year follow-up period was marked by complete resolution of the severe preoperative head pain and longstanding migrainous headaches. Recovery of the left oculomotor nerve palsy was complete 4 months after the operation.
Case 2
A 30-year old woman, who had suffered from paroxysmal left sided headaches for many years, was admitted because of increased severity of head and orbital pain that failed to respond to medical treatment for 3 weeks. Left third nerve palsy was noted a day before admission. CT scan of the brain was unremarkable but thin suprasellar cuts were not carried out. Examination revealed an alert patient complaining of severe left-sided head pain, but otherwise in good health. Third nerve palsy was present. Left carotid angiogram showed a posterior communicating artery aneurysm that projected posteriorly and had a lobulated configuration (Figure 4).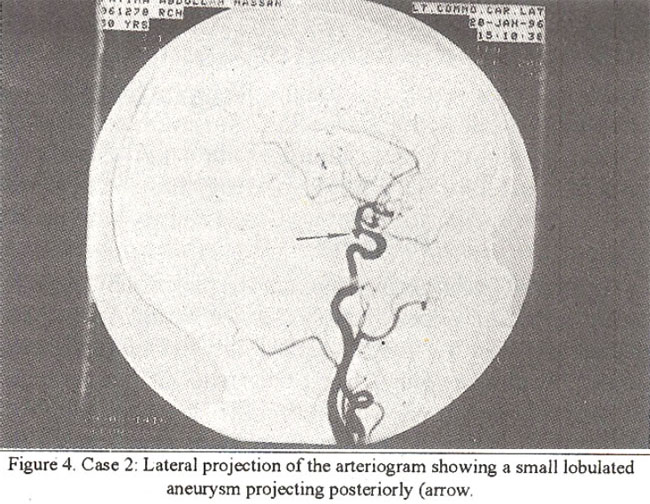
Operative findings were similar to the first case. The dome of the aneurysm as well as a thin-walled pulsating lobule were located in a tight space medial to the tentorial edge. The weak, thin-walled saccule started leaking just before the application of the clip, in spite of minimal manipulation. Postoperatively, the patient did well and volunteered a complete relief of her unilateral headache. Return of third nerve functionbegan soon after surgery with complete recovery by 3 months postoperatively.
Discussion
In typical migraine, a physical or surgically treatable cause is rarely found and angiography to rule out an intracranial vascular anomaly is seldom carried out We, alongwith others4-9, feel that intracranial aneurysms may, at times, cause a migraine headache syndrome, especially with atypical features. These atypical features of migraine that should arouse suspicion include: beginning of migmine after the age of 40 years5, sudden change in the character of the migmine6, transient weakness of one arm and leg or oculomotor nerve5,9. In our series of 50 patients who underwent aneurysm surgery, only two were diagnosed and pre-emptively operated in the pre-rupture stage on the basis of atypical migraine. However, careful questioning in the remaining 48 elicited a history of antecedent headache, distinct from that associated with the subarachnoid hemorrhage (SAB) in 19 (39%) patients, with orbital pain in nine (19%) patients. Similar migrainous histoiy is common in patients with unruptured but symptomatic cerebral aneurysms10. Change in the nature and severity of longstanding headache, as noticed in our patients, may be caused by aneuzysmal dilatation and enlargement leading to stretchingorcompressionofthe nerves orlocaipressure effect onthe sensitive dura111. The headaches may beperiodicoreven migrainous in nature8,11,12. Walton9 believed that the most common site of an aneuiysm associated with migraine headache is the internal carotid posterior communicating artery and in 150 cases of SAH, Magee12 found 2% with antecedent histoiy of ophthalmoplegic migraine. Local anatomical peculiarities of certain aneurysms provide the anatomico-physiological basis for the development of atypical migraine syndrome. For example, in both of our cases, the posterior communicating artety aneutysm was located in avery tight space medial to the tentorial edge where the fundus was in contact and pulsating against the sensitive basal dura as well as the third nerve. An enlarged thin walled lobule indicating recent dilatation was noticed in both the cases. The basal dura in this region is richly supplied by the sensoiy nerve endings from the first division of trigeminal nerve. The pain caused by the pressure/pulsation of the aneurysm against this dura is therefore referrd to the distributionof the ophthalmic division of the trigeminal nerve and at times becomes truly hemicranial. Alteration in the character of the headache may be an ominous sign6 and may indicate an impending rupture as was confinned by the operative findings of our cases. The possible mechanisms involved in the causation of headache by the unruptured aneurysms and change in character of headache prior to frank rupture are reviewed by others13 and include: (a) referred pain by traction or pressure of the aneurysm on the tentorial edge (first division trigeminal nerve supply); (b) distension of the aneurysmal sac stimulating periarterial sensoiy fibres. The true incidence of symptomatic unruptured aneuiysms is not known14, but their number is not insignificant10. Prompt referral of thIs group of patients with suggestive symptoms including atypical migraine, to specialized centres for angiographic evaluation and, possible treatment in the pre-rupture stage is the only way in which significant advances in reducing the overall mortality and morbidity of this serious condition canbe achieved.
References
1. Kassel, N.E and Drake, CO. Timing of aneurysm surgery. Neurosurgcry, 1982,10:514-519.
2. Kassell, N.F., Tome; J.C. and Haley, E.C. The International CoopeTative Study on the timing of aneurysm surgery: Part I. Overall management results. J. Neurosurg., 1 990;73: 18-36.
3. Walton, L. Subarachnoid hemorrhage. In: Lord Walton’s Essentials of Neurology. 6th Edition, Edinburgh, New York, Churchill Livingstone, 1989, pp. 268-271.
4. Bramwell, E. The etiology of.recurrent ocular paralysis (including periodic ocular paralysis and ophthalmoplegic migraine). Edinburgh Med. J., 1933;40:209.21. 8.
5. Dalessio, D.J. The cerebral circulation and the headache of subarachnoid hemorrhage. In: Woiffs: Headache and other head pain. 3rd edition, New York, Oxford University Press, 1972, pp. 189-212.
6. Frankel, K. Relation ofmigraine to cerebral aneurysm. Arch.Neurol. Psychiat., 1950;63:195-204.
7. Money, R.A. and Vanderfield, G.K, Periodic migrainous hcadache associated with cerebral vascular malformations and aneurysms. West J. Surg., 1960;68 :247-248.
8. Vanderfield, 0. Periodic headache associated with cerebral aneurysm, with report of a case successfully treated by surgery. Med. 3. Aust., 1957;2:289-290.
9. Walton, L. Migraine. In: Lord Walton’s Essential of Neurology. 6th edition, Edinburgh, New York, Churchill Livingstone, 1989, pp. 54-57.
10. Locksley, H.B. Report on the cooperative study of intracranial aneurysms and subarachnoid hemorrhage, SectionS, Part 2, Natural history of subarachnoid hemorrhage, intracranial aneurysms and arteriovenous malformations. J. Neurosurg., 1 966;25:321 -368.
11. Stehbens, W.E, The pathology of intracranial arterial aneurysms and their complications.ln: Fox, J.L. ed, Intracranial Aneurysms. Vol. 1, New York, Springer-Verlag, 1983, Pp. 272-342.
12. Magee, C.G. Spontaneous subarachnoid hemorrhage. Lancet, 1943;ii:497-500,
13. Jamn, K.K. Headache in relation to intracranial aneurysm. Headache, 1967;7: 122-126.
14. Fox, J.L. The incidence of intracranial aneurysms. In: Fox, J.L. Ed.). Intracranial aneurysms. VoL 1, New York, Springer Verlag, 1983, pp. 15-17.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: