
Raheela Mohsin Rizvi ( Department of Obstetrics and Gynaecology, Aga Khan University Hospital, Karachi, Sindh, Pakistan. )
January 2013, Volume 63, Issue 1
Short Communication
Abstract
The Multiparous Goat Pelvic Model was used to train obstetricians and residents for perineal and anal sphincter anatomy and techniques of repair of Obstetric Anal Sphincter Injuries (OASIs). The purpose of this study was to assess the similarity of this model with human anatomy and the usefulness of goat model for training obstetricians for perineal tears. Six workshops were conducted between June 2009 and December 2010. A total of 90 participants, including 64(70.3%) residents and 26(28.5%) consultants in Obstetrics and Gynaecology, attended hands-on training workshops using experimental goat pelvic model for the repair of perineal tears. Among the consultants, 23(88.5%), and 60(93.7%) residents could easily identify the goat anal sphincter. With reference to the similarity to human vaginal dimensions, 20 (76.9%) consultants and 43(67.1%) residents found it to be similar with human anatomy. Evaluating the anal canal anatomy, 22 (84.6%) consultants and 34(53.1%) residents reported it to be similar to the human anal canal. The perineal body anatomy was reported as very different by both consultants and residents (80% and 67.9% respectively). All the consultants and 49(76.5%) of the residents strongly recommended the use of this model for future hands-on workshops.
Keywords: Goat pelvic model, OASI, Anal canal.
Introduction
Obstetric Anal Sphincter injuries (OASI) occur in 0.5-9% of vaginal births.1 Women who have sustained OASI are more likely to suffer from faecal incontinence2 and OASI are responsible for significant physical, sexual and psychological sequelae.3 Women who have sustained OASI require more accurate, up to date information on the likelihood of developing faecal, urinary and sexual symptoms following primary repair.4 Therefore, accurate recognition and repair of anal laceration are of paramount importance in obstetric care. Unfortunately, it has been shown previously that up to half of OASI are not recognised by the surgeons.5 Perineal lacerations are repaired as an emergency surgical procedure and inadequate training of doctors and midwives in perineal and anal sphincter anatomy is believed to be a major factor in failure to recognise the injury and appropriate repair.6 An adequate experimental animal model is an alternative for training and humanising learning, avoiding the first training on humans. There is no local data available for the prevalence of perineal tears in Pakistan. However, one study showed the frequency of third and fourth degree perineal tears as 0.5%.7 Considering limited resources, we initiated local hands-on workshops using an experimental multiparous goat model for the repair of OASI to educate obstetricians and residents in perineal and anal sphincter anatomy and repair techniques of OASI. The objective was to present an animal model for training of identification of anal sphincter.
Methods and Results
The prospective cross-sectional study was conducted from June 2009 to December 2010 during which six workshops were held at Aga Khan University Hospital, Karachi. There were 90 participants; 64 (71.1%) residents, and 26 (28.8%) consultants in Obstetrics and Gynaecology.
Multiparous goats were selected due to similarity with human anatomy and special instructions were given to the butcher to prepare a model with intact vagina, anal canal and bladder (Figure).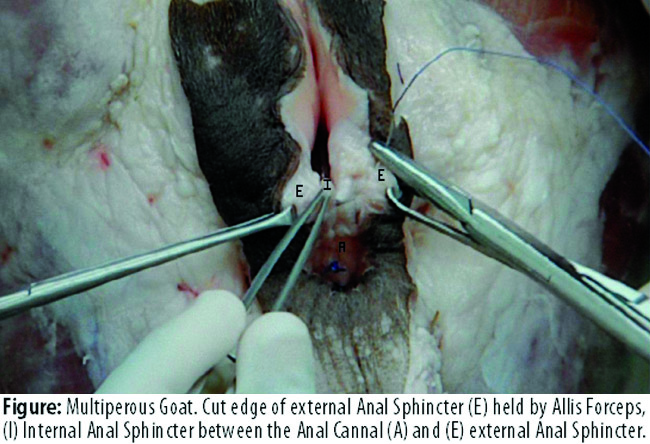
A 15-minutes video was prepared using this model for demonstration of the anal sphincter anatomy, recognition of tears and repair of laceration according to guidelines given by the Royal College of Obstetricians and Gynaecologists (RCOG). Each workshop included 15 participants who were divided into a group of three, and each group was given one animal model for hands-on experience, and, to avoid group biases, each participant was asked to identify and repair the perineal tear. One model was used three times by the removal of the applied sutures without distortion of anatomy. The participants gave the consent before answering all the related questions and the study received ethical exemption from the university\\\'s ethical research committee. An iatrogenic third or fourth degree tear was given and practical training included identification and repair of torn internal anal splincters (IAS) and external anal sphincters (EAS) according to the RCOG guidelines. The workshop participants answered a questionnaire (Appendix)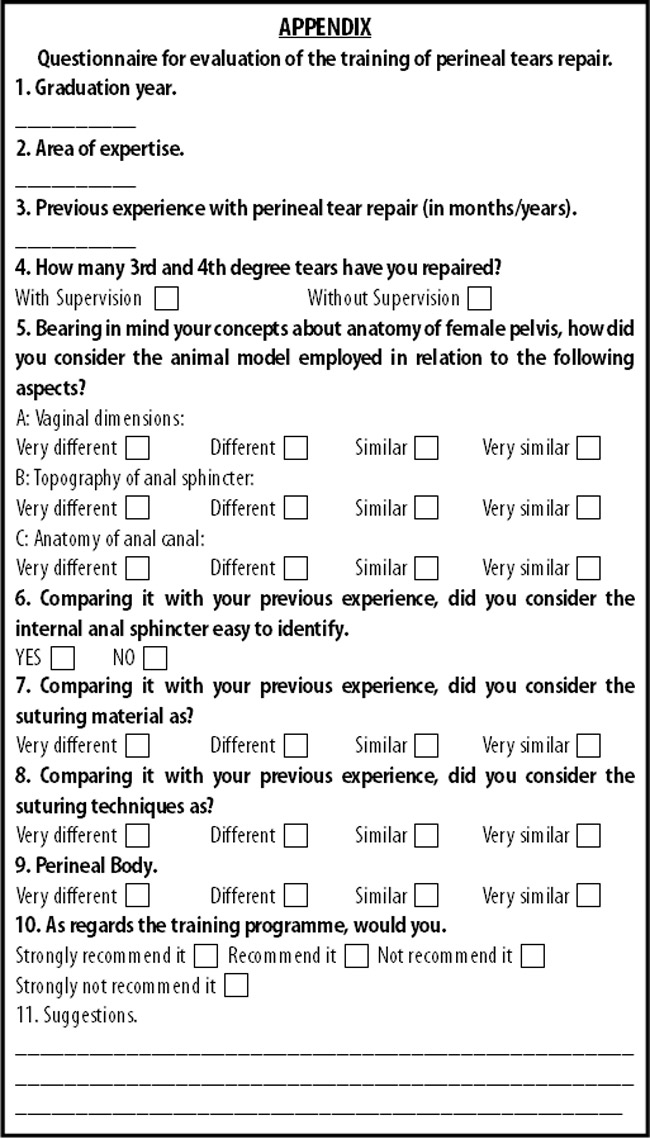
related to similarities found between goat and human female regarding anatomical aspects and surgical technique employed individually. SPSS 19 was used for statistical analysis.
A questionnaire was developed to get responses regarding usefulness of animal model for perineal repair training. The number of years since the participants had graduated ranged from 2 to 23 (median 11 years). Consultants had on average performed a mean of 5 supervised and 10 repairs of OASI independently. The previous experience with perineal tear identification and repair ranged from 0 to 20 years (median 4.5 years) among the consultants, and the residents\\\' experience ranged from 0 to 2 years. Sixty (93.7%) residents and 23(88.5%) consultants could identify both internal and external anal sphincter injuries (Table).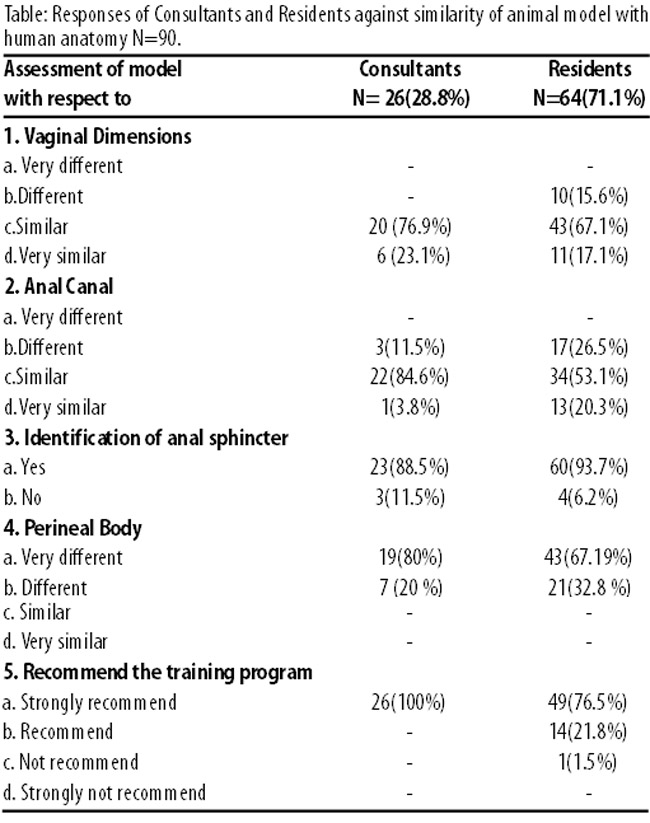
All the consultants and 49(76.5%) residents strongly recommended the use of animal model for future training of residents.
Discussion
Various models have been developed for teaching and assessment of residents\\\' competency in obstetric anal sphincter laceration repair. The beef-tongue model has been described in the literature as an economical and effective tool to demonstrate the repair of perineal tears.8 The original model lacked a clear demarcation of the internal sphincter and, hence, a modified model was introduced to check residents\\\' competence in sphincter laceration repair.9 The residents demonstrated sub-standard skill in repairing anal sphincter laceration. The low pass rate of 42.5% suggests lack of adequate training in repair and the satisfaction with the beef-tongue model was significantly higher with those who passed compared to those who failed (8.40 compared with 7.41; P=0.2).9 In our study, 84.6% consultants and 53.1% residents demonstrated similarity of anal canal with human anatomy, and 88.5% consultants and 93.7% residents were able to identify both external and internal anal sphincter in the goat model. Prior experience in perineal tears surgery helps in the identification of sphincter and the use of video enables postgraduate trainees to improve knowledge of the repair of third and fourth-degree laceration.5 We also incorporated a 15-minutes DVD on goat model for better understanding of anatomy and repair of sphincter and the results of a randomised controlled study showed a significant improvement in the anatomy, repair methods and complication subscales among the DVD and non-DVD users.10 The first international hands-on workshop was introduced by Thakar and Sultan11 on the management of OASI to educate obstetricians in perineal and anal sphincter anatomy and techniques of repair of OASI using cadaveric pig\\\'s anal sphincters. This one-day course comprised lectures, video demonstration on repair techniques and identification of OASI and hands-on training using a specially-designed latex perineal model and cadaveric pig\\\'s anal sphincters. Training evaluation was focused on change in practice amongst obstetricians after attending the course and does not include the validity of models used for simulating human anatomy.
Conclusion
There is no model that perfectly reproduces the anatomical disposition of the human female pelvis. The goat model has many similarities with human anatomy, but the major difference is the lack of distinct perineal muscles .The perineal body in goat is very thin, but it does demarcate the vagina and anal sphincter. Another study needs to be planned regarding the impact of such workshops on the participants\\\' future practise.
References
1. RCOG Green top Guidelines. The management of third and fourth degree perineal tears, 2007; 29.
2. Fenner DE, Genberg B, Brahma P, Marek L, DeLancey JO. Fecal and urinary incontinence after vaginal delivery with anal sphlincter disruption in an obstetrics unit in the United States. Am J Obstet Gynaecol 2003; 189: 1543-50.
3. Groom KM, Paterson-Brown S. Can we improve on the diagnosis of third degree tears? Eur J Obstet Gynecol Reprod Biol 2002; 101: 19-21.
4. Marsh F, Lynne R, Christine L , Alison W. Obstetric anal sphincter injury in the UK and its effect on bowel, bladder and sexual function.Eur J Obstet Gynecol Reprod Biol 2011; 154: 223-7.
5. Andrews V, Sultan AH, Thakar R, Jones PW. Occult anal sphincter injuries - myth or reality? Br J Obstet Gynaecol 2006; 113: 195-200.
6. Sultan AH, Kamm MA, Hudson CN. Obstetric perineal trauma: an audit of training. J Obstet Gynaecol 1995; 15: 19-23.
7. Rizvi RM, Chaudhury N. Practices regarding diagnosis and management of third and fourth degree perineal tears. J Pak Med Assoc 2008; 58: 244-7.
8. Woodman PJ, Nager CW. From the simple to the sublime:incorporating surgical models into your surgical curriculum. Obstet Gynecol Clin North Am 2006; 33: 267-81.
9. Uppal S, Harmanli O, Rowland J, Hernandez E, Dandolu V. Resident competency in obstetric anal sphincter laceration repair. Obstet Gynecol 2010; 115: 305-9.
10. Chao TT, Wendel GD Jr, McIntire DD, Corton M. Effectiveness of an instructional DVD on third and fourth -degree laceration repair for obstetrics and gynaecology postgraduate trainees. Int J Gynecol Obstet 2010; 109: 16-9.
11. Andrews V, Thakar R, Sultan AH. Structured hands-on training in repair of obstetric anal sphincter injuries (OASI): an audit of clinical practice. Int Urogynecol J Pelvic Floor Dysfunct 2009; 20: 193-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: