
Asad Ali Toor ( Hamdard College of Medicine & Dentistry, Hamdard University, Karachi. )
Seema Nigh-e-Mumtaz ( Department of Community Health Sciences, Hamdard University, Karachi. )
Rasheedullah Syed ( Hamdard College of Medicine & Dentistry, Hamdard University, Karachi. )
Mahmood Yousuf ( Department of Surgery, Hamdard University, Karachi. )
Ameena Syeda ( Hamdard College of Medicine & Dentistry, Hamdard University, Karachi. )
January 2013, Volume 63, Issue 1
Original Article
Abstract
Objectives: To evaluate the current practices regarding formal or informal implementation of individual elements of the World Health Organisation\\\'s Surgical Safety Checklist in tertiary care hospitals of Karachi and to establish a pre-checklist baseline to suggest a plan for implementation of the checklist.
Methods: The qualitative knowledge-attitude-practice (KAP) survey was conducted from May 1, 2009 to January 31, 2010, during whch 103 surgeries were observed in 10 hospitals across Karachi based on simple stratified sampling. Initially, 15 tertiary care hospitals were selected, but response and consent was received from 10 of them. The WHO checklist was applied after some basic changes according to local needs and perspectives. The surgical teams were also observed for coordination and working harmony. The data was analysed on SPSS version 12 and statistical tests were applied accordingly.
Results: Of the 103 surgeries observed, 13 (13.4%) patients did not confirm their identity, site of surgery or procedure. There was no concept of timeout in 91 (88.5%) cases, while in 52 (53.8%) cases, the anaesthetist did not ask for known allergy, and prophylaxis antibiotic was not given in 36 (37.5%) cases. In 20 (21.2%) cases, sponge, needle and instruments were not counted.
Conclusion: The results suggest that the safety of surgical patients in the operating theaters in hospitals under review was far from satisfactory. Introduction of and adherence to a safety checklist would result in significant reduction in death and complication rate.
Keywords: Surgical safety, Quality, General surgery, Operation theatres. (JPMA 63: 76; 2013)
Introduction
Surgical adverse events due to negligence are increasingly recognised as an important aspect for preventing morbidity and mortality in healthcare system.1 Half of all the adverse events in healthcare occur in surgical care and more than half of these are preventable. The number of these adverse events is directly proportional to the complexity of surgery, length of the hospital stay and patient\\\'s poor compliance.2 A look at the figure of global volume of surgery reveals an enormous 272 million surgical procedures annually which is more than twice the number of annual childbirths.3 This is largely due to substantial rise in life expectancy and surgically treatable conditions like ischaemic heart disease, cerebrovascular disease, cancers, and mental illness in low-income, middle-income, and high-income countries.4 Surgical care can be divided into pre-operative, per-operative and post-operative care. Previous studies have shown that improvement in per-operative care can prevent postoperative complications.5,6 The risk of complications in surgical care is poorly characterised in many parts of the world; studies in the industrialised world have shown major complications of 3-17% and a mortality rate of 0.4-0.8%.7 In Pakistan, the mortality rate is higher than reported in high-income countries.8
Different protocols were developed to prevent these devastating complications.9,10 Joint Commission on Accreditation of Healthcare Organisation (JACHO) implemented universal protocol in 2004 for preventing wrong-site, wrong-procedure and wrong-person surgery.11-13 In recent years, the most notable effort to prevent complications from negligence is by World Health Organisation (WHO) which developed a Surgical Safety Checklist. A study published in 2009 showed that the comprehensive checklist can reduce morbidity and mortality in a global population.14 The checklist outlines essential standards of surgical care and is designed to be simple, to be widely applicable, and to address common and potentially disastrous lapses. Use of the checklist can identify gaps in per-operative practice and can establish or confirm adherence to proven standards of care that can improve surgical results and decrease death and complications. In Pakistan the use of surgical safety checklist is practised only in three hospitals.15 Other hospitals are practicing different protocols. There is no standardised protocol for the safety procedures to be adopted in the surgical theatres of tertiary care hospitals. There is a gross need for some standardised safety tool for the avoidance of preventable adverse events in surgical care. The WHO\\\'s Surgical Safety Checklist seems to be quite simple and appropriate tool which can easily be implemented in tertiary care hospitals. Keeping this scenario in mind, the researchers planned this study to pilot test the need base of surgical safety checklist.
Material and Methods
The study design was qualitative KAP survey. The sampling method was probability simple random. The study population was all surgical operation theatres of tertiary care hospitals of Karachi, Pakistan. The study was conducted from May 1, 2009 to January 31, 2010. The target population was general surgical operation theatres of tertiary care hospitals of Karachi, who gave written consent and had a surgical team conducting general surgery. Fifteen hospitals (tertiary care) were selected and 10 (66%) of them gave consent. The study setting was general surgery operation theater suites of the hospitals (Table-1).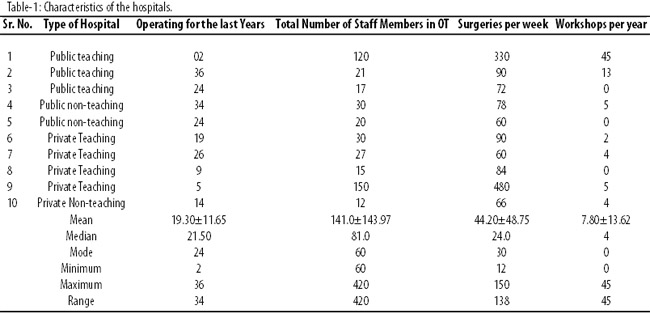
The study duration was 9 months as a whole, but the time period for data collection was 75 working days. It took about 2.5 month for data collection and on an average 5 days at each hospital.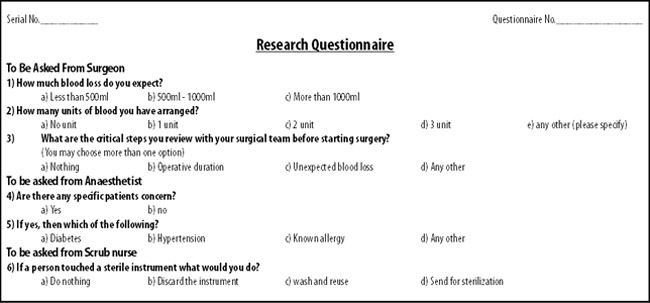
The surveyors were trained by the research supervisor and principal investigator in association with the Surgical Safety Checklist programme which is run from Harvard School of Public Health. Two questionnaires were used; one filled by the surgical team, and the other filled by the surveyors. The patient was followed from the time of entry into the operation theater till shifting to post-operative care. A total of 103 cases were observed during the 2.5-month period. Statistical analysis was done by using SPSS 12, and test of significance were applied where needed.
Results
A total of 103 elective surgeries were observed at 10 hospitals in the study. A summary of the different surgeries that were observed was noted (Table-2). Each element of checklist was individually observed regarding formal or informal implementation of checklist of any kind. The WHO Surgical Safety Checklist (Figure)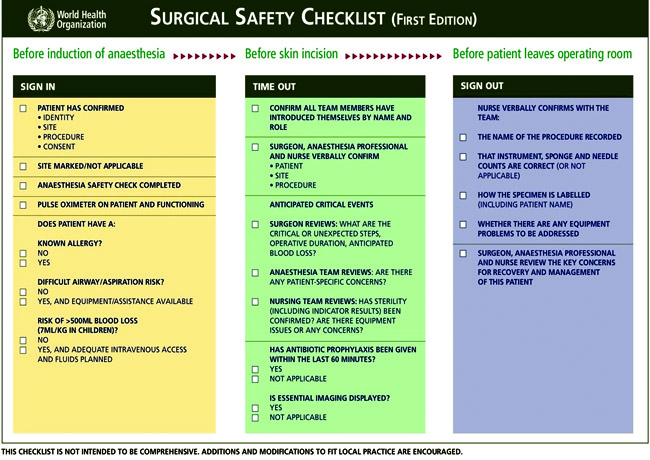
has three parts: sign in; time out; and sign out.
Sign in, which is the period after the handing over of patient to operation theatre staff and before the induction of anaesthesia was observed first (Table-3).
Surgical site was not marked in 11 (10.7%) cases; anaesthetist assessment for safety of anaesthesia was not done in 22 (21.4%) cases; pulse oximeter was not on patient in 2 (1.9%) cases; any known allergy was not asked in 47 (45.6%) cases; difficult airway was not checked in 40 (38.8%) cases; blood loss was not estimated in 3 (2.9%) cases; and inadequate intravenous access was present in 2 (1.9%) cases.
Time out, which is the period after the induction of anaesthesia and before surgical incision, was assessed next. During time out, 91 (88.3%) team members did not introduce themselves by name and role; surgeons did not discuss critical steps in 43 (41.7%) cases; anaesthetist did not review specific patient concerns in 42 (40.8%); nursing team did not review sterility in 29 (28.2%) cases; and prophylaxis antibiotic was not administered in 38 (38.7%) cases within the final 60 minutes.
Sign out, the period during or immediately after wound closure but before removing the patient from the operating room, was the final observation scale. The name of the procedure was not recorded in 34 (33%); instruments, needles and sponges were not counted in 21 (20.4%) cases; specimen was taken in 28 (27.2%) cases; out of these 11 (10.7%) were labelled by patient’s name and specimen; 10 (9.7%) by patient’s name, specimen and registration number and 7 (10.7%) were labelled by patient’s name; concerns for the recovery and management were not reviewed in 35 (34.0%) patients.
Discussion
The findings showed that the concept of formal confirmation of patient\\\'s identity, site, procedure, and consent was new to most of our research locations. A study showed the commonest error for malpractice claims was wrong-site surgery (62%).16 Another study showed anatomical marking reduced wrong-site surgery to 1 in 112,500 patients which resulted in minimal harm.17 In addition, none of the surgical teams called a formal time out which is to conduct a final verification of the correct patient, procedure, and site and, as applicable, implant.18 The researchers ascertained there was no formal team introduction and briefing in 88.3% cases which can cause failure in communication. In one survey, two-thirds of nurses and physicians cited better communications in a team as the most important element in improving safety and efficiency in the operating room.19 One study accounted a considerable discrepancy in perceptions of teamwork existing in the operating room, with physicians rating the teamwork of others as good, but at the same time, nurses perceive teamwork as mediocre which can only be solved by communication.20 The researchers witnessed failure to count sponges, instruments and needles in almost one-fifth of the cases. A study showed most common retained foreign body was a sponge (69%) which sometime presents in the most unexpected way.21 In one-fifth of the cases, the patients were not assessed for safety of anaesthesia which accounts for 2.5% of early post-operative deaths.22 In more than half of the cases, patients were not asked for any known allergy which occurs in 2-4% anaesthetic drugs.23 Failure to administer prophylactic antibiotics was found in 40% of cases which is associated with surgical-site infection, mortality and excess length of hospitalization.24 Use of WHO Surgical Safety Checklist not only ensures administration of antibiotic medications, but also appropriate timing for best outcome.
The WHO checklist has already proved its efficacy in a global population. An interesting aspect of the checklist is that clinicians held the checklist in high regard and the overwhelming majority would want it used if they were undergoing surgery themselves.25
There is a need of an implementation plan by involving the surgical team and integrating it into routine practice. At most of our research locations, people were not aware of the WHO checklist. All healthcare professionals involved in performing invasive procedures as well as the patients must be actively involved in ensuring correct surgical and interventional procedures. Team training with its explicit knowledge, skills, and attitudes required of the full surgical team, including the clerical scheduling personnel, nurses, surgeons, and anaesthesiologists should be required in healthcare facilities.26
The study was limited to one city and most of the study settings were teaching hospitals where surgical safety measures are expected to be better. This study was also limited to per-operative care only. The actual outcome of the surgical procedures was not detected by the researchers.
Conclusion
There is a gross need for implementation of a standardised surgical safety checklist at tertiary care hospitals. This can be done by adopting the tool of WHO which has been globally tested. Some amendments may be made to fulfill local needs. Large-scale studies need to be conducted for overall need assessment of surgical safety checklist in Pakistan. The use of a surgical safety checklist can prevent many adverse events.
References
1. Brennan TA, Leape LL, Larid NM, Herbert L, Localio AR, Weilier PC, et al. Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. N Eng J Med 1991; 324: 370-6.
2. Dindo D, Demartines N, Clavien PA, Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240: 205-13.
3. Weiser TG,Regenbogen SE, Thompson KD, Haynes AB, Lipsitz SR, Berry WR, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 2008; 372: 139-44.
4. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2006; 3: e 442.
5. Saufl NM. Universal protocol for preventing wrong site, wrong procedure, wrong person surgery. J Perianaesthesia Nurs 2004; 19: 348-51.
6. Silen-Lipponen M, Smith A, Tossavainen K, Turunen H, et al. Potential errors and their prevention in operating room teamwork as experienced by Finnish, British and American nurses. Int J Nurs Pract 2005; 11: 21-32.
7. Gawande AA, Thomas EJ, Zinner MJ, Brennan TA. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery 1999; 126: 66-75.
8. Ahmed N, Aurangzeb M, Alam K, Khitab N, Zaein M. Surgical audit with risk adjusted mortality rates using the POSSUM scoring system. Pak J Surg 2008; 24: 163-7.
9. Michaels RK, Makary MA, Dahab Y, Frassica FJ, Heitmiller E, Rowen LC, et al. Achieving the National Quality Forum\\\'s "Never Events": prevention of wrong site, wrong procedure, and wrong patient operations. Ann Surg 2007; 245: 526-32.
10. Cima RR, Kollengode A, Pool SR, Moore D, Koch MB, Weisbrod CA, et al. A multidisciplinary team approach to retained foreign objects. Jt Comm J Qual Patient Saf 2009; 35: 123-32.
11. Saufl NM, Universal protocol for preventing wrong site, wrong procedure, wrong person surgery. J Perianesth Nurs 2004; 19: 348-51.
12. Ludwick S. Surgical Safety: Addressing the JCAHO Goals for Reducing Wrong-site, Wrong-patient. 2005.
13. Angle JF, Nemcek AA Jr, Cohen AM, Miller DL, Grassi CJ, Khan AA, et al. Quality improvement guidelines for preventing wrong site, wrong procedure, and wrong person errors: application of the joint commission "universal protocol for preventing wrong site, wrong procedure, wrong person surgery" to the practice of interventional radiology. J Vasc Interv Radiol 2009; 20: S256-62.
14. Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Dellinger EP, Herbosa T, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med 2009; 360: 491-9.
15. World Health Organization. Patient Safety. A world alliance for safer health care. Surgical Safety web map. (Online) (Cited 2010 June). Available from URL: http://maps.cga.harvard.edu:8080/Hospital/.
16. Kwaan MR, Studdert DM, Zinner MJ, Gawande AA, et al. Incidence, patterns, and prevention of wrong-site surgery. Arch Surg 2006; 141: 353-7.
17. Knight N, Aucar J. Use of an anatomic marking form as an alternative to the Universal Protocol for Preventing Wrong Site, Wrong Procedure and Wrong Person Surgery. Am J Surg 2010; 200: 803-7.
18. Guidelines for implementing the Universal Protocol for Preventing Wrong Site Wrong Procedure and Wrong Person Surgery. (Online) (Cited 2004 July 4). Available from URL: www.jcaaho.org/accredited+organizations/patient+safety/universal+protoc/up+guidelines.pdf.
19. Sexton JB, Thomas EJ, Helmreich RL. Error, stress, and teamwork in medicine and aviation: cross sectional surveys. Br Med J 2000; 320: 745-9.
20. Makary MA, Sexton JB, Freischlag JA, Holzmueller CG, Millman EA, Rowen L, et al. "Operating room teamwork among physicians and nurses: teamwork in the eye of the beholder." J Am Coll Surg 2006; 202: 746-52.
21. Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med 2003; 348: 229-35.
22. Ouro-Bang\\\'na Maman AF, Tomta K, Ahouangbévi S, and Chobli M. Deaths associated with anaesthesia in Togo, West Africa. Trop Doct 2005; 35: 220-2.
23. Runciman WB. Iatrogenic harm and anaesthesia in Australia. Anaesth Intensive Care 2005; 33: 297-300.
24. Kirkland KB, Briggs JP, Trivette SL, Wilkinson WE, Sexton DJ. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hospital Epidemiol 1999; 20: 725-30.
25. Senior K. WHO Surgical Safety Checklist has value worldwide. Lancet Infect Dis 2009; 9: 211.
26. Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Vats A, Taylor B, et al. Changes in safety attitude and relationship to decreased postoperative morbidity and mortality following implementation of a checklist-based surgical safety intervention. BMJ Qual Saf 2011; 20: 102-7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: