
Murat Kalayci ( Departments of Neurosurgery, Zonguldak Karaelmas University Medical School, Turkey. )
Erol Aktunc ( Department of Family Medicine, Zonguldak Karaelmas University Medical School, Turkey. )
Sanser Gul ( Departments of Neurosurgery, Zonguldak Karaelmas University Medical School, Turkey. )
Volkan Hanci ( Department of Anesthesiology, Zonguldak Karaelmas University Medical School, Turkey. )
Nurullah Edebali ( Departments of Neurosurgery, Zonguldak Karaelmas University Medical School, Turkey. )
Ferda Cagavi ( Department of Neurosurgery Kocaeli Acibadem Hospital, Turkey. )
Bektas Acikgoz ( Departments of Neurosurgery, Zonguldak Karaelmas University Medical School, Turkey. )
January 2013, Volume 63, Issue 1
Original Article
Abstract
Objective: To identify specific factors that can be used to predict functional outcome and to assess the value of decompressive craniectomy in patients with acute subdural haematoma.
Methods: The retrospective study was done at the Zonguldak Karaelwas University Practice and Research Hospital, Turkey, and included 34 trauma patients who had undergone decompressive craniectomy for acute subdural haematoma from 2001 to 2009. At the 30th day of the operation, the patients were grouped as survivors and non-survivors. Besides, based on their Glasgow Outcome Scale, which was calculated 6 months post-operatively, the patients were divided into two functional groups: favourable outcomes (4-5 on the scale), and unfavourable outcomes (1-3 on the scale). The characteristics of the groups were compared using SPSS 15 for statistical analysis.
Results: One-month mortality was 38.2% (n=13) and 6-month total mortality reached 47% (n=16). Patients with higher pre-operative revised trauma score, Glasgow coma scale, partial anterial pressure of carbon dioxide, arterial oxygen pressure, Charlson co-morbidity index score, blood glucose level, blood urea nitrogen, and lower age had a higher rate of survival and consequently a favourable outcome. Higher platelet values were only found to be a determinant of higher survival at the end of the first month without having any significant effect on the favourable outcome.
Conclusion: In patients of traumatic acute subdural haematoma whose Glasgow coma scale on arrival was < 8, a massive craniectomy along with the evacuation of the haematoma, may be considered as a treatment option for intra-operative and post-operative brain swelling. But in patients with a score of 3 on arrival and bilaterally fixed and dilated pupils, decompressive craniectomy is unnecessary.
Keywords: Acute subdural haematoma, Trauma, Decompressive craniectomy, Outcome. (JPMA 63: 38; 2013).
Introduction
Traumatic acute subdural haematoma (SDH) continues to have high morbidity and mortality rates despite the advent of rapid transportation, computed tomography (CT) scanning, intracranial pressure monitoring and intensive care management.1,2 Outcome for these patients may be influenced mainly by the underlying brain injury than the SDH itself.3
Despite studies on the impact of early craniectomy (EC) in traumatic acute SDH,4,5 the value of primary decompressive craniectomy (DC) remains uncertain. To our knowledge, there are only two studies comparing mortality rates between normal craniotomy and DC.3,6 In a group of 180 patients, one study reported a higher mortality rate in DC than EC.3 However, the study had some pitfalls, as the two groups were not adjusted for age and Glasgow coma scale (GCS), or the presence of the signs of herniation. Consequently, subjects undergoing DC have had a higher rate of herniation and mortality than the subjects in the other group.3
The other study reviewed a group of 34 patients having acute SDH.6 The study performed DC in severe patients having significant brain oedema, while craniotomy was performed in less severe patients without any cliniclally devastating brain oedema.6 The study failed to find any favourable neurological outcome in patients undergoing DC seemingly due to a randomisation pitfall.6
Our aim in the present study was to assess the value of DC in acute SDH. We sought to assess whether the surgical procedure conferred any increase in short-term survival rates and long-term favourable outcomes defined by the Glasgow outcome scale (GOS) score in the study population. Special emphasis was placed on the relationship between patient characteristics and functional outcome to ascertain patient selection criteria that may ensure better surgical results in the future.
Patients and Methods
In this retrospective cross-sectional study, records of 34 patients were analysed who had undergone DC for acute SDH from 2001 to 2009 at the Zonguldak Karaelmas University Practice and Research Hospital in Zonguldak, Turkey. Following the establishment of airway patency and appropriate fluid resuscitation, patients having significant acute SDH in CT were immediately operated for decompression.
Data about the demographical characteristics such as age and gender, the history and clinical findings such as mechanism of injury, the time duration from the traumatic event until surgical decompression, the hemispherical location of the haematoma, the presence of extracranial injury, systolic and diastolic blood pressure, the pupillary reactivity and the signs of herniation (unilateral or bilateral pupil dilatation) were recorded.
Laboratory data such as the presence of midline shift at the level of septum pellucidum in CT, complete blood count, full biochemistry and arterial blood gas measurements were also recorded at admission to the emergency department.
Complete blood count tests included haemoglobin (normal value 12-18 mg/dl), white blood cell count (normal value 4800-10800/mm3) and platelet (PLT) count (normal value 130.000-400.000/mm3).
Full biochemistry included blood glucose level (GLU) (normal value 70-110 mg/dl), blood urea nitrogen (BUN) (normal value 10-50 mg/dl), creatinine (CRE) (normal value 0.5-1.2 mg/dl), sodium (Na) (normal value 135-157 mEq/lt), potassium (K) (normal value 3.5-5.5 mEq/lt), calcium (Ca) (normal value 8.4-10.2 mEq/lt), chlorine (Cl) (normal value 98-110 mEq/lt), aspartate aminotransferase (AST) (normal value <40 IU.L-1), alanine aminotransferase (ALT) (normal value <40 IU.L-1), alkaline phosphatase (ALP) (Normal value 40-129 IU.L-1), gamma glutamil transferase (GGT) (Normal value <73 IU.L-1 in males; <38 IU.L-1 in females), lactate dehydrogenase (LDH) (normal value 120-146 U.L-1), creatine kinase (CK) (normal value 32-294 U.L-1 in males; 33-211 U.L-1 in females), creatine kinase-MB (CKMB) (normal value 0.6-6.3 ng/ml), total protein (Normal value 6.4-8.3 gr/dl), and albumin (normal value 3.2-4.8 gr/dl).
Arterial blood gas measurements included pH (normal value 7.35-7.45), partial arterial pressure of carbondioxide (PaCO2) (normal value 35-45 mmHg), partial arterial pressure of oxygen (PaO2) (normal value 80-100 mmHg), and arterial oxygen saturation (SO2) (normal value >90%).
Patients were preoperatively evaluated for GCS, Revised trauma score (RTS) (Table-1),7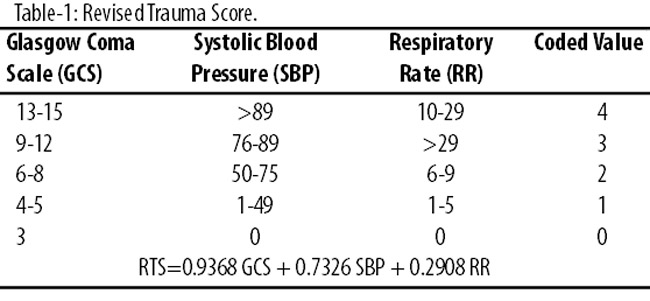
Charlson co-morbidity index score (CCIS) (Table-2)8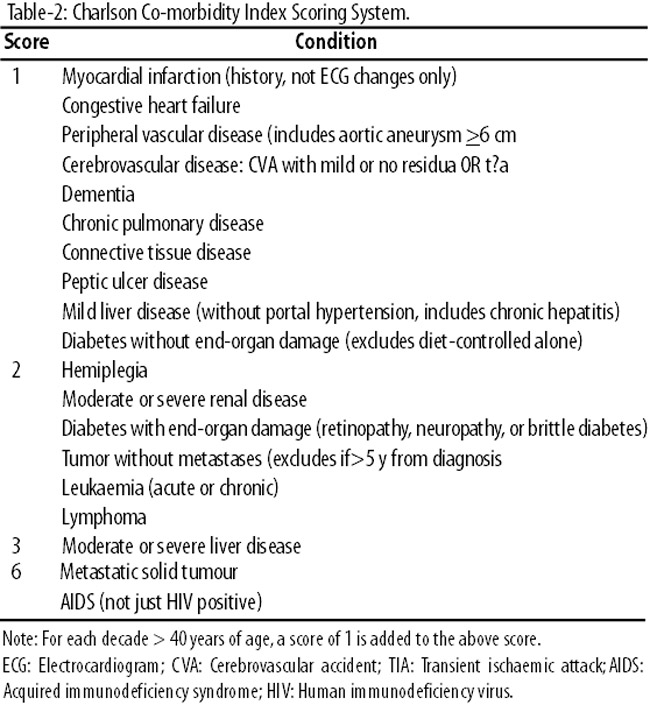
and GOS.9
Therapeutic measures such as the duration for intravenous infusion of mannitol solution, the need and the duration for thiopental infusion and mechanical ventilation were recorded.
A unilateral or bilateral fronto-temporo-parietal craniectomy was performed depending on the extent and location of SDH with a question mark-shaped skin flap based on the ear. The bone flap was approximately 15cm in diameter. The temporal bone was craniectomised upto the base of the skull to maximise the extent of decompression at the level of the perimesencephalic cisterns. The dura was opened in stellate fashion and then haematoma was evacuated. The cortical surface of the swollen brain was protected against the sharp edges of the cut dura. Following the decompression, autologous pericranial layer was spread over the brain instead of a watertight duraplasty. The removed bone flap was then placed in a subcutaneous pocket overlying the abdomen for subsequent cranioplasty. The continuous sedation was tapered according to the needs of each patient and withheld on day five or six of the surgical decompression. Post-operatively, patients had at least one CT. If and when the patient recovered sufficiently, the preserved bone flaps were replaced or methyl methacrylate cranioplasties were performed (Figure-1).
At the 30th day of the operation, the patients were grouped as survivors and non-survivors and were compared for their demographical, history-related and clinical parametres as well as laboratory test results. The factors affecting the survival rate were evaluated.
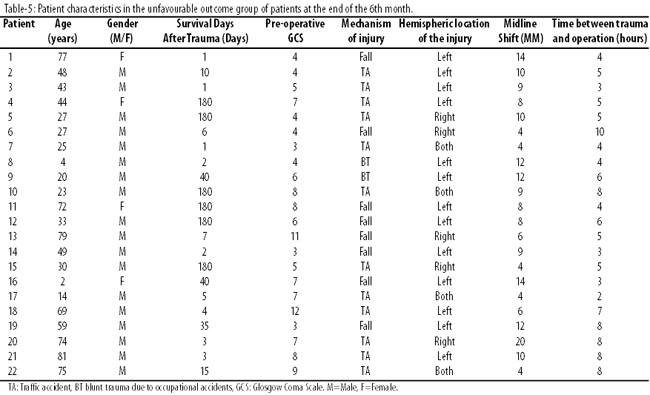
At the end of the 6th month, the surviving patients were re-classified into favourable and unfavourable outcome groups according to their GOS in order to disclose the factors affecting long-term physical disabilities. The favourable outcome was defined as GOS 4 (moderate disability) and 5 (good recovery including independent daily living activity), while unfavourable outcome was defined as GOS 1 (death), 2 (vegetative state) or 3 (severe disability).
Statistical analaysis was carried out using SPSS 15. Continuous variables were presented as means ± standard deviation, while categorical variables were presented in terms of frequency and percentage. P values less then 0.05 were considered to be significant. Mann Whitney U test was used to compare the continuous variables, whereas the Chi-square test was used for comparing categorical variables. Pearson\\\'s correlation analysis was used to disclose factors affecting survival and favourable outcome.
Life table analysis was performed using \\\'Survival days following surgery\\\' as the dependent variable. The maximum life span was determined as 180 days (6 months) with an interval of 10 days. The status variable was selected as GOS at the end of the 6th month.
A cox regression analysis was conducted in order to disclose any indicators affecting the mortality rate. The relative risks were calculated.

Results
The study group consisted of 26 (76.5%) males and 8 (23.5%) females, with the mean age being 37.2±24.3 years, ranging between 2 and 81 years. The mechanisms of injury were traffic accidents in 17 (50.0%); fall in 13 (38.2%) and blunt injury due to occupational accidents in 4 (11.8%) patients. Left hemispheric injury was found in 18 (52.9%); right hemispheric injury in 11 (32.4%); and bilateral hemispheric injury in 5 (14.7%) patients.
Acute SDH was the only injury in 26 (76.5%) patients, while the remaining 8 (23.5%) had accompanying extracranial injuries. The extracranial injuries were classified as intra-abdominal bleeding in 2 (5.9%); pneumothorax in 2 (5.9%); traumatic enucleation of the eye in 2 (5.9%); cervical vertebral fracture in 1 (2.9%); and thoracic vertebral fracture in 1 (2.9%) patient. Pre-operative median GCS was 7, ranging from 3 to 13, and the mean midline shift in CT was 8.7±4.2mm, ranging from 2 to 20mm.
By the 30th day of the operation, 13 (38.2%) patients were dead and 21 (61.8%) had survived (Figure-2).
The survival rate at this point of time did not differ according to gender, mechanism of injury, the time duration from the traumatic event until surgery, hemispheric location of the injury, the presence of extracranial injury, or the level of systolic and diastolic blood pressure at admission to the emergency department. However, the age and the presence of the signs of herniation differed significantly between the survivors and the non-survivors (Table-3).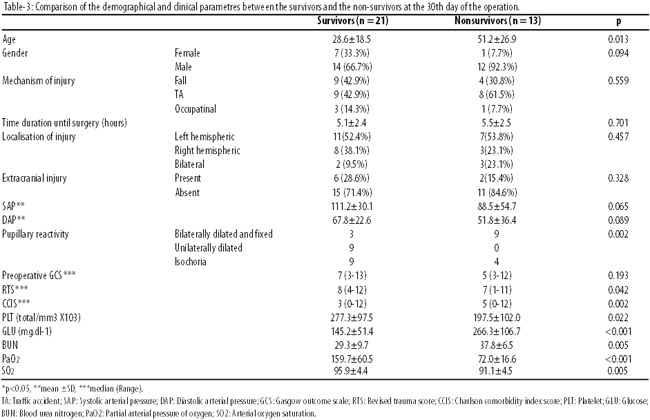
All of the patients with unilaterally dilated pupils (n=9) survived. Pre-operative GCS did not differ among the survivors and the non-survivors at the 30th day of the surgery. All the 3 patients scoring 3 in pre-operative GCS were dead. Four of the 5 patients scoring 4 in pre-operative GCS were dead and the remaining 1 patient scored GOS 2 at the 6th month (Tables 4 and 5).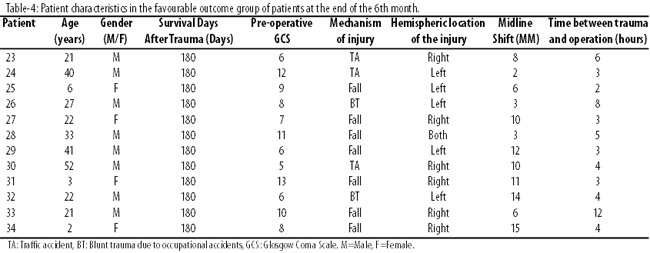
However, the survivors scored significantly higher RTS and lower CCIS.
Among the laboratory values at admission, PLT, GLU, BUN, PaO2 and SO2 values differed significantly between the survivors and the non-survivors. The rest of the CBC, biochemistry and arterial blood gas analysis along with the midline shift in CT remained insignificant between the groups.
A couple of complications were observed on the 30th day of the operation in 7 (20.6%) of the surviving patients; 1 (2.9%) being cerebral abscess, 1 (2.9%) being hydrocephalus, and superficial wound infections in the remaining 5 (14.7%) were observed. The surgical defect was closed using autograft in 7 (20.6%) patients and methyl methacrylate cranioplasty in 7 (20.6%) patients.
The Pearson\\\'s analysis of correlation revealed a couple of prognostic factors (Table-6).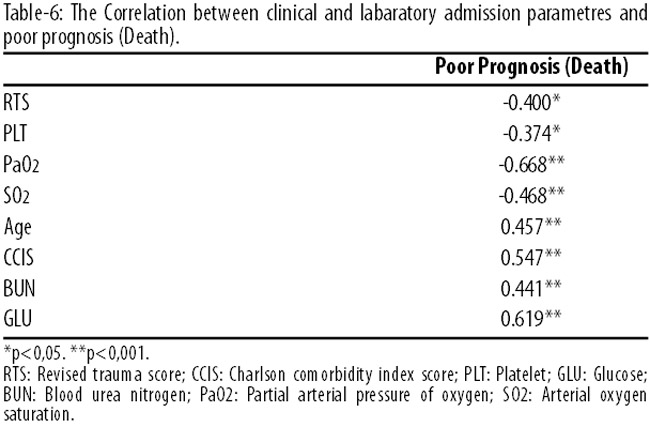
At the 30th day of the surgery, good prognosis was positively correlated with lower age, CCIS, BUN and GLU, whereas negatively correlated with lower RTS, PLT, PaO2 and SO2 on admission.
When 60 years of age was chosen as a cutoff point for age, the survivors at the 30th day of the operation were found to be significantly younger than the non-survivors. Similarly, pre-operative GCS>5, RTS>5, CCIS<5, glucose<180 mg.dl-1, PaO2 >160 (mmHg), SO2 >96 (%) were found to be the significant clinical and laboratory findings affecting the survival positively at the 30th day of surgery (Table-7).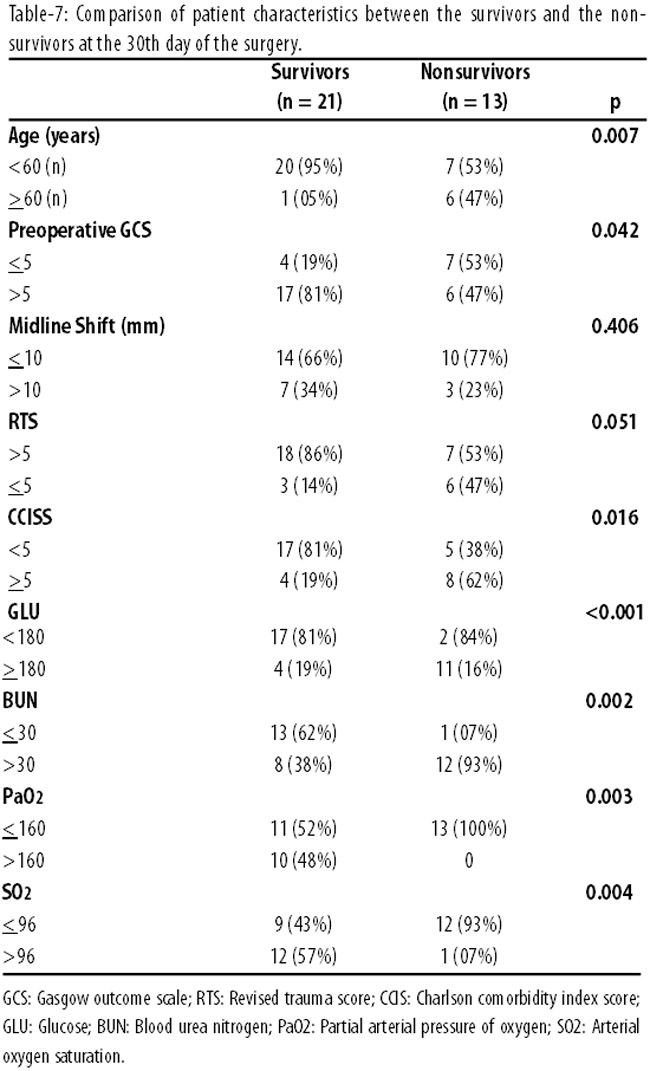
At the end of the 6th month from the surgery, 16 (47.0%) of the patients were dead, while 18 (53.0%) had survived (Figure-2). At this point of time, the patients were re-classified into favourable (n=12; 35%) and unfavourable (n=22; 65%) outcome groups according to their GOS (Table-8).
The favourable outcome rate at this time point did not differ according to gender, mechanism of injury, the time duration from trauma untill surgery, hemispheric location of the injury, the presence of extracranial injury, or the levels of systolic and diastolic arterial blood pressure at admission to the emergency department (Table-9).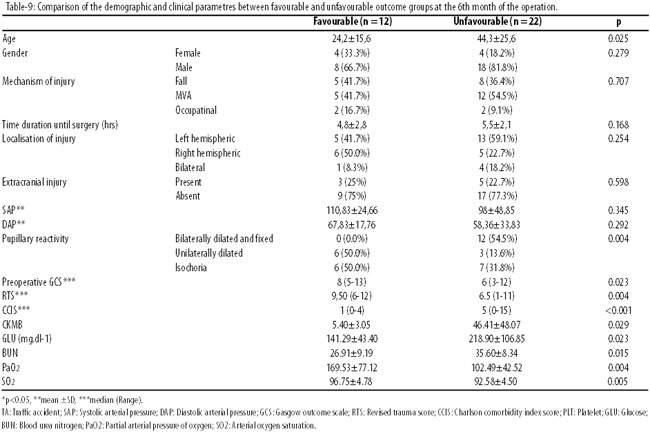
The age and the presence of the signs of herniation differed significantly between favourable and unfavourable outcome groups.
All of the patients with bilaterally dilated and fixed pupils (n=12) were in the unfavourable outcome group at the end of the 6th month. All the patients older than 60 years of age scored GOS 1 or 2 at the end of the 6th month. All of the patients in the favourable outcome group were ?60 years of age (Table-10).
The pre-operative GCS at the end of the 6th month of surgery was significantly higher in the favourable outcome group. All of the patients in the favourable outcome group had scored >5 in pre-operative GCS. They had also scored significantly higher RTS and lower CCIS.
Among the laboratory values at admission, significantly lower GLU, CKMB, BUN along with higher PaO2 and SO2 were observed in the favourable outcome group. Unlike the 30th day of the surgery, the PLT did not differ between the groups at the end of the 6th month. The rest of the CBC, biochemistry and arterial blood gas analyses along with the midline shift in CT remained insignificant between the groups at the end of the 6th month.
The Pearson\\\'s analysis of correlation revealed a couple of prognostic factors (Table-11).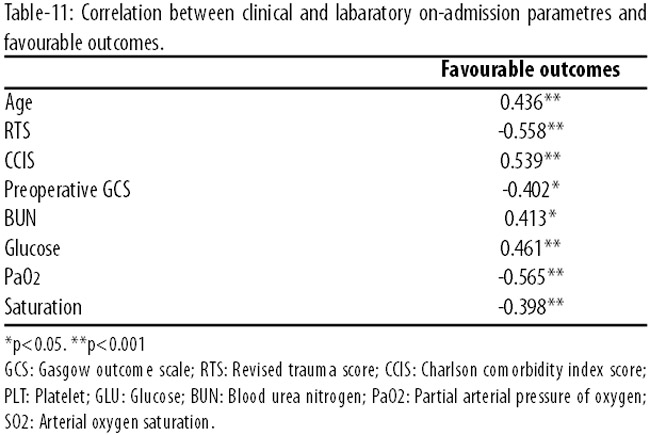
At the 6th month of the surgery, a favourable outcome was positively correlated with lower age, CCIS, BUN, CRE and GLU, whereas it was negatively correlated with lower RTS, PaO2, SO2 and pre-operative GCS on admission.
When 60 years of age was taken as the cutoff point for age, patients older than 60 years had a significantly unfavourable outcome at the end of the 6th month of the surgery. Similarly, pre-operative GCS <5, RTS <5, CCIS >5, glucose >180 (mg.dl-1), PaO2 <160 (mmHg), SO2 <96 (%) were all the determinants of poor prognosis and unfavourable outcome at the end of the 6th month of the surgery (Table-12).
The number of terminal events were 13 during the first month, and 3 during the second month of the surgery. The proportion of termination was 0.38 for the first month, being the highest, and 0.14 for the second month (Table-13).
The survival rate decreased sharply during the initial two months time following the surgery and became steady from the third month onwards (Figure-3).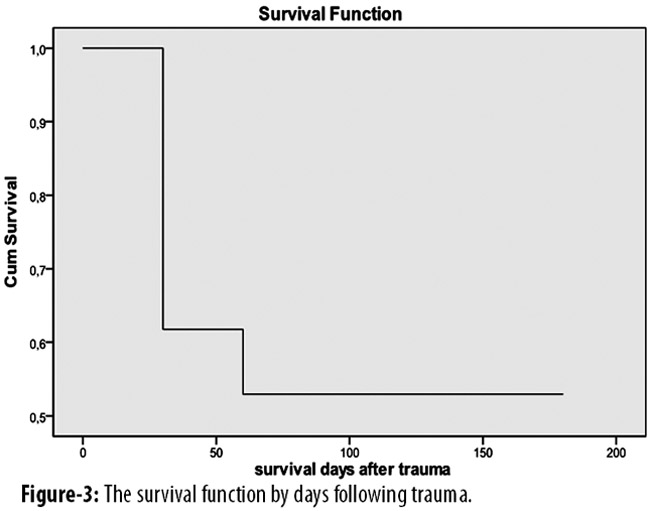
The survival regarding gender was apparently higher among the female patients (Figure-4).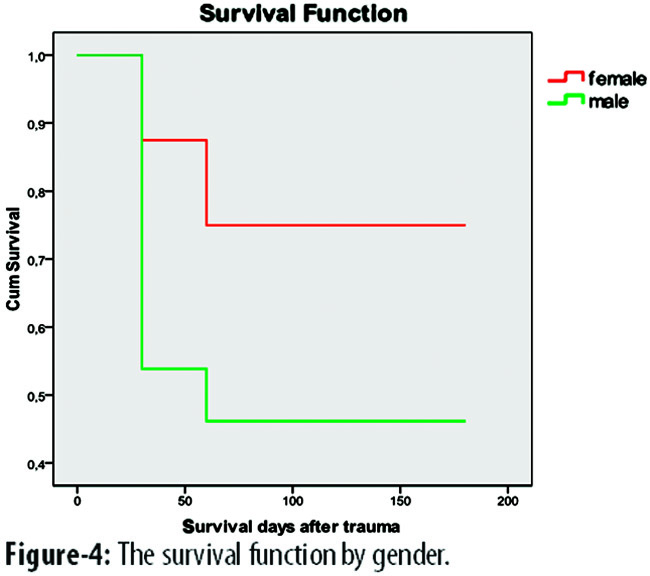
A cox regression analysis was conducted about some selected study parametres regarding the favourable and unfavourable outcome at the end of the 6th month. These selected parametres were transformed into categorical variables in order to perform the analysis (Table-14).
The predicted change in the hazard (Exp(B)) was significant for RTS>5 and age<60 years. Only younger age and RTS>5 were found to have significant effects on the favourable outcome at the end of the 6th month (Table 15).
The rest of the study parametres were insignificant regarding the favourable outcome in the study population.
Discussion
The present study mainly comprised of male patients having acute SDH primarily due to traffic accidents. Female patients had a higher survival rate than the male patients. The survival rate of the study group decreased sharply during the initial two months. The survival rate at the end of the first month as well as the favourable outcome at the end of the 6th month of the operation was higher in younger patients without any signs of herniation at admission to the emergency department.
Along with young age patients with higher pre-operative RTS, GCS, PaO2, SO2, CCIS, GLU, and BUN readings had a higher rate of survival and consequently a favourable outcome. Higher PLT values were only found to be a determinant of higher survival at the end of the first month without having any significant effect on the favourable outcome. Although BUN and pre-operative GCS produced lower p values than the other vairables in the cox regression analysis, the sample population was perhaps too small to detect any significant difference between the groups regarding these parametres. Studies in wider sample groups may be usefull to detect the effects, if any, of these parameters.
The mortality from acute SDH ranges from 55% to 79%, even with surgical treatment.1,3 There may be a trend of decreasing mortality over the last 25 years. However, in the present study, the first-month mortality rate was 38.2% and the 6th months mortality rate was 47%.
One study reported the brain dialysate lactate levels to rise and glucose levels to return to normal more rapidly in rats with induced SDH when these animals were ventilated 100% oxygen.[10] Thus, higher cerebral blood oxygen levels affect the cerebral glucose metabolism positively. Concordant with this finding, higher pre-operative PaO2 and SO2 values produced a more favourable outcome in our sample population.
Another study has shown that the vasogenic oedema in rats with intracerebral haemorrhage either in the affected hemisphere or in the contralateral part is exacerbated by hyperglycaemia. In cases with traumatic brain injury, hyperglycaemia may be considered a marker of brain injury and, when present upon admission, could reflect extensive brain damage which is associated with higher mortality and poor outcome.12,13 Concomittantly, lower glucose levels in our study population was found to be associated with better survival and favourable outcome.
Trauma is well known to be associated with cytotoxic and vasogenic brain oedema, aggravating intracranial hypertension associated with brain contusion.14-16 Less well recognised is that the presence of blood gives rise to haemotoxicity-related inflammation, which acts on capillaries to further aggravate oedema.14,17,18 The presence of blood in the subdural space of healthy or contused brain reduces regional cerebral microcirculation and causes oedema, ischaemia, and increased intracranial pressure (ICP).14,19,20 There is evidence that DC in animals can lower ICP and improve cerebral blood flow.21 A study22 indicated that DC is efficacious in adding to the available intracranial volume. DC significantly reduces intractable intracranial hypertension14,23 and improves brain tissue oxygenation,24,25 brain compliance,26 cerebral blood flow,27,28 pressure reactivity29 and cerebrovascular resistance.30 Each of these factors may lessen the burden of ischaemic penumbra, ischaemic brain volume and ICP.14,31
Severe life-threatening brain oedema occurs in approximately 85% of patients with an acute subdural haematoma.32 Thus, frequently massive intra-operative brain swelling accompanies surgery for acute subdural haematoma, especially when the thickness of the haematoma is smaller than the deviation in midline, as measured on the CT. Massive brain swelling is far more common in patients with the lowest pre-operative GCS scores and those with unilateral or bilateral dilated pupils, suggesting a relationship to prior hypoperfusion.33 Most are associated with early death due to increased ICP and subsequent uncal herniation.32 Our patients with herniation both had a lower survival rate and unfavourable outcome.
The precondition necessary for surgical evacuation of traumatic acute SDH has previously been well defined. An acute SDH with a thickness greater than 10mm or a midline shift greater than 5mm as determined from a CT scan should be surgically evacuated.6,34-36 However, there is no consensus regarding which surgical technique should be employed for the evacuation of acute traumatic SDH. Some surgeons perform craniotomies, while others perform DC. The presence and the degree of midline shift have not had any significant effect on either the survival or the favourable outcome in our study group.
In the 1970s, one study presented encouraging results with a hemicraniectomy followed by haematoma evacuation for SDH. It reported a recovery rate of 40%, but could not confirm these results in a later study.4,37 In a separate series of 15 patients, researchers found a slightly improved recovery and lower mortality in patients with hemicraniectomy and external drainage, but the results were not statistically significant.5
A 2008 study reported that 80 patients with acute SDH had early DC combined with uncusectomy and tentorial section to relieve brainstem compression.38 Craniectomy threshold was abnormal pupillary response to light and ICPs greater than 20mmHg. In that study, 75% patients had good outcome and only 15% died. Younger age was significantly related to good outcome.38 The association of higher survival and favourable outcome were also confirmed in our study population.
It is still a controversial point that in patients who have undergone craniectomy, cerebral oedema and the risk of additional cerebral damage due to the displacement of the brain increases.39 Although significant reduction of ICP and secondary ischaemia can be achieved, the procedure may allow herniation of brain tissue through the bone defect. This frequently results in the compression of arteries and veins by dural margin, causing further congestion, oedema and ischaemia in the herniated tissue.40-42 In order to prevent this complication, studies41,42 have suggested that the dura be opened in stellate fashion and the main cortical vessels to be left under the margins and not the corners of the dural opening. They have also emphasised the importance of generating a vascular tunnel by the placement of haemostatic sponges on both sides of the main vessels. The technique, as shown by them, decreased mortality and morbidity. We also followed this procedure in our study population.
When considering the treatment options, one should always keep in mind that DC, although not an obligation, entails certain risks for the patient. Blood loss, not an unusual complication in large wounds, during and after the operation and impaired blood coagulation, a frequently seen problem, can lower the cerebral perfusion pressure (CPP) dramatically.14,22 One study reported the risk of a new or expanded haemorrhagic contusion to be 58% in patients undergoing DC.43 The expansion of the haemorrhagic contusion was not life-threatening in our study group.
Moreover, DC for traumatic brain injury may incite a new mass lesion, contralateral or remote to the decompressed hemisphere.44,45 A study reported a 7% incidence of new contralateral haematomas, over half occurring within the initial 24-hour period following DC.45 Decompressive surgery may relieve the tamponade effect on a contralateral bleeding site and predispose the patient to an epidural haematoma.44 A study has reported new contralateral epidural haematomas in 71% of its population. We observed no such complications in our study group.
Decompressive craniectomy alters the dynamics of cerebrospinal fluid circulation. This may exacerbate the occurrence of subdural hygromas and hydrocephalus.14,22,44 Researchers reported a 50% rate of subdural hygroma and hydrocephalus following DC, regressing spontaneously over weeks to months.47 Others have reported a 21% rate of subdural hygroma, 87% resolving spontaneously without having any resultant neurological deficit.45 Only one patient developed hydrocephalus in our study group who was treated through placement of a ventriculoperitoneal shunt.
Infectious complications may emerge either following the surgery or the replacement of the bone flap.14,22,44 Our study group had one patient with cerebral abscess which deceased by the 5th month, while superficial wound infections were treated successfully in five patients.
Conclusion
The concept of performing decompressive craniectomy in traumatic acute subdural haematoma patients seems to be attractive. In SDH patients whose GCS on arrival is < 8, a massive craniectomy along with the evacuation of the haematoma may be considered as a treatment option for intra-operative and post-operative brain swelling. But in patients whose GCS is 3 on arrival and who have bilaterally fixed and dilated pupils, decompressive craniectomy is unnecessary. Patients over 60 years of age, or those with signs of herniation, male gender, pre-operative GCS<5, RTS<5, CCIS >5, GLU >180mg.dl-1, BUN >30mg.dl-1, PaO2 <160mmHg, SO2 <96% were found in our study to have poor prognosis. In order to assess the efficacy of DC on acute SDH and to provide solid criteria for the necessity of this type of surgical decompression of the brain, it is essential to perform studies with larger population size.
References
1. Servadei F. Progostic factors in severely head injured adult patients with acute subdural haematomas. Acta Neurochir 1997; 139: 279-85.
2. Koc RK, Akdemir H, Oktem IS, Meral M, Menku A. Acute subdural hematoma: outcome and outcome prediction. Neurosurg Rev 1997; 20: 239-44.
3. Woertgen C, Rothoerl RD, Schebesch KM, Albert A. Comparison of craniotomy and craniectomy in patients with acute subdural haematoma. J Clin Neurosci 2006; 13: 718-21.
4. Ranshoff J, Benjamin MV, Gage EL, Epstein F. Hemicraniectomy in the management of acute subdural haematoma. J Neurosurg 1971; 34: 70-6.
5. Shigemori M, Syojima K, Nakayama K, Kojima T, Ogata T, Watanabe M, et al. The outcome from acute subdural haematoma fallowing decompressive hemicraniectomy. Acta Neurochir 1980; 54: 61-9.
6. Wong GK, Hung YW, Chong C, Yeung J, Chi-Ping Ng S, Rainer T, et al. Assessing the neurological outcome of traumatic acute subdural hematoma patients with and without primary decompressive craniectomies. Acta Neurochir Suppl 2010; 106: 235-7.
7. Champion HR, Sacco WJ, Copes WS, Gann DS, Gennarelli TA, Flanagan ME. A revision of the trauma score. J Trauma 1989; 28: 623-9.
8. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A. new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-83.
9. Jennett B, Bond M. Assessment of outcome after severe brain damage: a practical scale. Lancet 1975; 1: 480-4.
10. Reinert M, Alessandri B, Seiler R, Bullock R. Influence of inspired oxygen on glucose-lactate Dynamics after subdural hematoma in the rat. Neurol Res 2002; 24: 601-6.
11. Song EC, Chu K, Jeong SW, Jung KH, Kim SH, Kim M, at al. Hyperglycemia exarbates brain edema and perihematomal cell death after intracerebral haemorrhage. Stroke 2003; 34: 2215-20.
12. Melo JR, Di Rocco F, Blanot S, Laurent-Vannier A, Reis RC, Baugnon T, et al. Acute hyperglycemia is a reliable outcome predictor in chilhren with severe traumatic brain injury. Acta Neurochir 2010; 152: 1559-65.
13. Kreutziger J, Schlaepfer J, Wenzel V, Constantinescu MA. The role of admission blood glucose in outcome prediction of surviving patients with multiple injuries. J Trauma 2009; 67: 704-8.
14. Aarabi B, Hesdorffer DC, Simard JM, Ahn ES, Aresco C, Eisenberg HM, et al. Comparative study of decompressive craniectomy after mass lesion evacuation in severe head injury. Neurosurgery 2009; 64: 927-40.
15. Marmarou A. Traumatic brain edema: an overview. Acta Neurochir Suppl 1994; 60: 421-4.
16. Simard JM, Kent TA, Chen M, Tarasov KV, Gerzanich V. Brain oedema in focal ischaemia: Molecular pathophysiology and theoretical implications. Lancet Neurol 2007; 6: 258-68.
17. Chen-Roetling J, Regan RF. Effect of heme oxygenase-1 on the vulnerability of astrocytes and neurons to haemoglobin. Biochem Biophys Res Commun 2006; 350: 233-7.
18. Hoff JT, Xi G. Brain edema from intracerebral hemorrhage. Acta Neurochir Suppl 2003; 86: 11-5.
19. Fujisawa H, Maxwell WL, Graham DI, Reasdale GM, Bullock R. Focal microvascular occlusion after acute subdural haematoma in the rat: A mechanism for ischemic damage and brain swelling. Acta Neurochir Suppl 1994; 60: 193-6.
20. Sawauchi S, Beaumont A, Signoretti S, Tomita Y, Marmarou C, Marmarou A. Diffuse brain injury complicatd by acute subdural hematoma in the rodents: The effect of early or delayed surgical evacuation. Acta Neurochir Suppl 2002; 81: 234-44.
21. Rinaldi A, Mangiola A, Anile C, Maira G, Amante P, Ferraresi A. Hemodynamic effects of decompressive craniectomy in cold induced brain oedema. Acta Neurochir Suppl 1990; 51: 394-6.
22. Münch EC, Horn P, Schürer L, Piepgras A, Paul T, Schmiedek P. Management of severe traumatic brain injury by decompressive craniectomy. Neurosurgery 2000; 47: 315-23.
23. Schneider GH, Bardt T, Lansksch WR, Unterberg A, Decompressive craniectomy following traumatic rain injury: ICP, CPP and neurologic outcome. Acta Neurochir Suppl 2002; 81: 77-9.
24. Jaeger M, Soehle M, Meixensberger J. Effect of decompressive craniectomy on brain tissue oxygen in patients with intracranial hypertension. J Neurol Neurosurg Psychiatry 2003; 74: 513-5.
25. Stiefel MF, Heuer GG, Smith MJ, Bloom S, Moloney-Wilensky E, Gracias VH, et al. Cerebral oxygenation following decompressive hemicraniectomy for the treatment of refractory intracranial hypertension. J Neurosurg 2004; 101: 241-7.
26. Timofeev I, Czosnyka M, Northje J, Smielewski P, Kirkpatrik P, Gupta A, et al. Effect of decompressive craniectomy on intracranial pressure and cerebrospinal compensation following traumatic brain injury. J Neurosurg 2008; 108: 66-73.
27. Csokay A, Pataki G, Nagy L, Belan K. Vascular tunnel construction in the treatment of severe brain swelling caused by trauma and SAH (evidence based on intra-operative blood flow measure). Neurol Res 2002; 24: 157-60.
28. Hlatky R, Valadka AB, Goodman JC, Robertson CS. Evolution of brain tissue injury after evacuation of acute traumatic subdural hematomas. Neurosurgery 2004; 55: 1318-24.
29. Wang EC, Ang BT, Wong J, Lim J, Ng I. Characterization of cerebrovascular reactivity after craniectomy for acute brain injury. Br J Neurosurg 2006; 20: 24-30.
30. Bor-Seng-Shu E, Hirsch R, Teixeira MJ, De Andrade AF, Marino R Jr. Cerebral hemodynamic changes gauged by transcranial Doppler ultrasonography in patients with posttraumatic brain swelling treated by surgical decompression. J Neurosurg 2006; 104: 93-100.
31. Cunningham AS, Salvador R, Coles JP, Chatfield DA, Bradley PG, Johnston AJ, et al.Physiological thresholds for irreversible tissue damage in contusional regions following traumatic brain injury. Brain 2005; 128: 1931-42.
32. Coplin WM, Cullen NK, Policherla PN, Vinas FC, Wilseck JM, Zafonte RD, et al. Safety and feasibility of craniectomy with duraplasty as the initial surgical intervention for severe traumatic brain injury. J Trauma 2001; 50: 1050-9.
33. Lobato RD. Sarabia R, Cordobes F, Rivas JJ, Andoras A, Cabrera A, et al. Post-traumatic cerebral hemispheric swelling. Analysis of 55 cases studied with computerized tomography. J Neurosurg 1988; 68: 417-23.
34. Bullock MR, Chesnut R, Ghajar J, Gordon D, Hartl R, Newell DW, et al. Surgical management of acute subdural hematomas. Neurosurgery 2006; 58: S2-16-S2-24.
35. Mathew P, Oluoch-olunya D, Condon B, Bullock R. Acute subdural haematoma in the conscious patient: outcome with initial nonoperative management. Acta Neurochir 1993; 121: 100-8.
36. Wong CW. Criteria for conservative treatment of supratentorial acute subdural haematmas. Acta Neurochir 1995; 35: 38-43:100-8.
37. Cooper PR, Rovit R?, Ranshoff J. Hemicraniectomy in the management of acute subdural haematoma: a re-appraisal. Surg Neurol 1976; 5: 25-8.
38. Salvatore C, Marco M, Antonio R, Salvatore I, Eugenio B. Combined internal uncusectomy and decompressive craniectomy and decompressive craniectomy for the treatment of severe closed head injury experience with 80 cases. J Neurosurg 2008; 108: 74-9.
39. Soukiasian HJ, Hui T, Avital I, Eby J, Thompson R, Kleisli T, et al. Decompressive craniectomy in trauma patients with severe brain injury. The American Surgeon 2002; 68: 1066-71.
40. Cooper PR, Hagler H, Clark WK, Barnett P. Enhancement of experimental cerebral edema after decompressive craniectomy: implications for the management of severe head injuries. Neurosurgery 1979; 4: 296-300.
41. Csokay A, Egyud L, Nagy L, Pataki G. Vascular tunnel creation to improve the efficacy of decompressive craniotomy in post-traumatic cerebral edema and ischemic stroke. Surg Neurol 2002; 57: 126-9.
42. Csokay A, Nagy L, Novoth B. Avoidance of vascular compression in decompressive surgery for brain edema caused by trauma and tumour ablation. Neurosurg Rev 2001; 24: 209-13.
43. Flint AC, Manley GT, Gean AD, Hemphill JC 3rd, Rosenthal G. Post-operative expansion of hemorrhagic contusion after unilateral decompressive hemicraniectomy in severe traumatic brain injury. J Neurotrauma 2008; 25: 503-12.
44. Stiver SI. Complications of decompressive craniectomy for traumatic brain injury. Neurosurg Focus 2009; 26: E7.
45. Yang XF, Wen L, Shen F, Li G, Lou R, Liu WG, et al. Surgical complications secondary to decompressive craniectomy in patients with head injury: a series of 108 consecutive cases. Acta Neurochir 2008; 150: 1241-8.
46. Su TM, Lee TH, Chen WF, Lee TC, Cheng CH. Contralateral acute epidural hematoma after decompressive surgery of acute subdural hematoma: clinical features and outcome. J Trauma 2008; 65: 1298-302.
47. Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg 2006; 104: 469-79.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: