
Ilker Arikan ( Department of Gynecology and Obstetrics, Zonguldak Karaelmas University, Zonguldak, Turkey. )
Aykut Barut ( Department of Gynecology and Obstetrics, Zonguldak Karaelmas University, Zonguldak, Turkey. )
Muge Harma ( Department of Gynecology and Obstetrics, Zonguldak Karaelmas University, Zonguldak, Turkey. )
Mehmet Ibrahim Harma ( Department of Gynecology and Obstetrics, Zonguldak Karaelmas University, Zonguldak, Turkey. )
Sener Gezer ( Obstetrics and Gynecology Clinic, Zonguldak Maternity Hospital, Zonguldak, Turkey. )
Zuhal Erdem ( Department of Radiology, Faculty of Medicine, Zonguldak Karaelmas University, Zonguldak, Turkey. )
December 2012, Volume 62, Issue 12
Case Reports
Abstract
Lung cancer during pregnancy is a rare situation which is being increasingly reported during the past two decades due to a rising trend of cigarette smoking among young women and the tendency to delay pregnancy to a later age in life. We describe the case of a 32-year-old woman with primary pulmonary sarcoma, diagnosed at 31st week of pregnancy. X-ray chest and thoracic magnetic resonance imaging revealed a 9 × 6 cm mass in the left mediastinum, with tracheal shift, and pleural effusion. Biopsy performed during broncoscopy, was reported as mesenchymal tumour. She delivered a baby by Caesarean section at the 32nd week of gestation due to the development of superior vena cava syndrome. A skin biopsy taken 3 weeks later from the nodular lesion at the periumblical region was reported as a tumour metastasis. She received radiotherapy for 10 days, but died in the intensive care unit. Malignancies, even those as uncommon as a pulmonary sarcoma, should be considered in the differential diagnosis of pleural effusion during pregnancy.
Keywords: Pregnancy, Lung cancer, Pulmonary sarcoma.
Introduction
Lung cancer is labelled as the most common malignant tumour in developed and developing countries. The prevalence of lung cancer in women is increasing over the last two decades, and females account for 12% of all cancers and 27% of all deaths.1 About 1 in 1000 pregnancies, will be complicated with cancer.2 Breast cancer, cervical cancer, lymphoma, and melanoma are most frequently diagnosed. Lung cancer is very rare during pregnancy, and few cases have been reported in the literature.3 The rising trend of cigarette smoking among young women and the tendency to delay pregnancy to later in life are associated factors for lung cancer in pregnant woman.4 We describe the case of a 32-year-old woman with primary pulmonary sarcoma diagnosed at the 31st week of pregnancy. She delivered an alive baby by Caesarean section at the 32nd week of gestation, but died 4 weeks postpartum.
Case Report
A 32-year-old non-smoking pregnant woman was admitted with cough, dyspnoea, nausea and vomiting at 30th week of pregnancy. Breath sounds were diminished on the left side on auscultation, and pleural effusion was evident in left hemithorax on chest X-ray. Her haematocrit was 28.8%, white blood cells 24,900/ml, and platelets were 797,000/ml. Blood chemistry was normal.
Because of the risk of X-ray exposure during pregnancy, magnetic resonance imaging (MRI) was used instead of a thoracic computed tomography scan. A 9 × 6 cm mass with shifted trachea and pleural effusion were observed on the MRI in left mediastinum (Figure).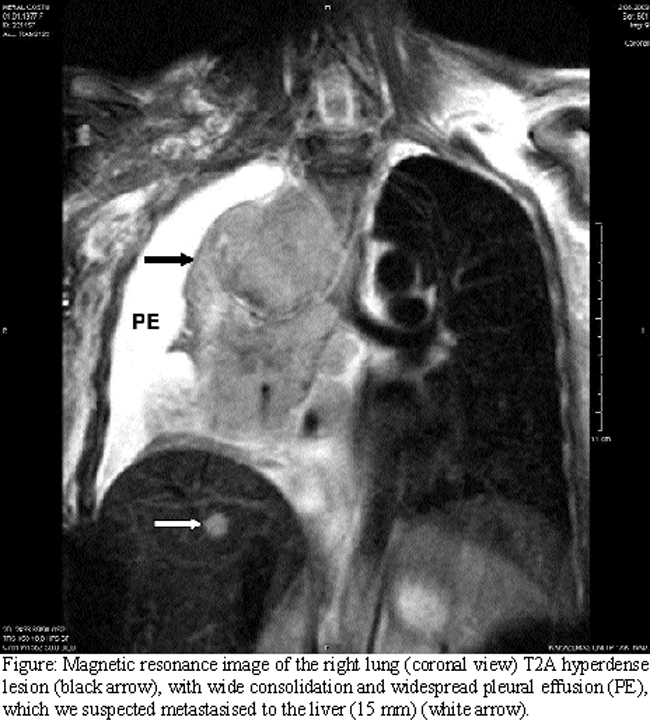
On the same MRI, a rounded hyperdense lesion of 15mm was observed which was suspected as metastasis in the liver. Bronchoscopy and bronchoalveolar lavage were performed under local anaesthesia. A pathological examination of the bronchoscopic biopsy was reported as a malignant mesenchymal tumour or pulmonary sarcoma. The diagnosis was confirmed by means of histochemical and immunhistochemical stainings. There were no specific features with periodic acid-Schiff (PAS), toluidin blue (pH:1) and masson- trichrome histochemical stainings. In tumour tissue, immunoreaction was observed only by vimentin, but no expressions were observed with pankeratin, epithelial membrane antigen (EMA), carcinoembryonic antigen (CEA), cytokeratin-7, cytokeratin-20, leukocyte common antigen (LCA), smooth muscle actin (SMA), desmin, Myo-D1, chromogranin-A, synaptophysin, S100 protein, HMB45, CD68, CD30, CD34, CD31, factor VIII, alpha feto protein (AFP), beta human chorionic gonadotropin (b hCG), placental alkaline phosphatase (PLAP), and Neu-N.
The patient delivered a baby by Caesarean section at the 32nd week of gestation due to the development of superior vena cava syndrome. A skin biopsy taken 3 weeks later from a nodular lesion at the periumblical region was reported as a tumour metastasis. She received radiotherapy for 10 days and died in the intensive care unit.
Discussion
Lung cancer is a rare diagnosis during pregnancy. A literature search indicated that most of these patients had non squamous cell lung cancer (NSCLC) at advanced stages. Most NSCLCs were adenocarcinomas.3 Unfortunately, the majority of reported cases were in advanced stages. Also, foetal and placental metastases have been observed.5
Treatment for lung cancer during pregnancy is a controversial topic because of few data and ethical problems. Platinum-based chemotherapy is used for some cases, as well as vinorelbine, paclitaxel, gemcitabine and etoposid, which are rarely used in combination.3,6 Radiotherapy has been used in two cases during gestation.7,8
No foetal anomalies have been reported among patients who took chemotherapy during pregnancy, but radiotherapy might be more harmful to the foetus. Our patient delivered immediately because of superior vena cava syndrome and received radiotherapy in the postpartum period. The perinatal outcome will be affected by the early gestational time and nutritional deficiencies caused by the tumour. The foetus had no need for newborn intensive care and is still living without any complications.
Conclusion
Lung cancer is rare during pregnancy but should be considered in the differential diagnosis of pleural effusion. To the best of our knowledge, this is the second reported case of primary pulmonary sarcoma during pregnancy as per literature search.
References
1. Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, et al. Cancer statistics, 2005. CA Cancer J Clin 2005; 55: 10-30.
2. Pentheroudakis G, Pavlidis N. Cancer and pregnancy: poena magna, not anymore. Eur J Cancer 2006; 42: 126-40.
3. Garrido M, Clavero J, Huete A, Sanchez C, Solar A, Alvarez M, et al. Prolonged survival of a woman with lung cancer diagnosed and treated with chemotherapy during pregnancy. Review of cases reported. Lung Cancer 2008; 60: 285-90.
4. Pavlidis N. Lung cancer during pregnancy: an emerging issue. Lung Cancer 2008; 59: 279-81.
5. Harpold TL, Wang MY, McComb JG, Monforte HL, Levy ML, Reinisch JF. Maternal lung adenocarcinoma metastatic to the scalp of a fetus. Case report. Pediatr Neurosurg 2001; 35: 39-42.
6. Janne PA, Rodriguez-Thompson D, Metcalf DR, Swanson SJ, Greisman HA, Wilkins-Haug L, et al. Chemotherapy for a patient with advanced non-small-cell lung cancer during pregnancy: a case report and a review of chemotherapy treatment during pregnancy. Oncology 2001; 61: 175-83.
7. Reiter AA, Carpenter RJ, Dudrick SJ, Hinkley CM. Pregnancy associated with advanced adenocarcinoma of the lung. Int J Gynaecol Obstet 1985; 23: 75-8.
8. Van Winter JT, Wilkowske MA, Shaw EG, Ogburn PL, Jr., Pritchard DJ. Lung cancer complicating pregnancy: case report and review of literature. Mayo Clin Proc 1995; 70: 384-7.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: