
Saeed Akhter ( Department of Otolaryngology Head & Neck Surgery, Karachi, Pakistan. )
Sadaf Zia ( Liaquat National Hospital, Dow International Medical College, Karachi, Pakistan. )
Rafay Zafar ( Department of Neurosurgery, Karachi, Pakistan. )
September 2012, Volume 62, Issue 9
Case Series
Abstract
The objectives of the study was to determine the causes and outcome of endoscopic repair of cerebrospinal fluid (CSF) leak in a developing country. A total of five patients were recruited in the study. The age of patients ranged from 8 to 65 years. Four patients were male and one was female. In two cases of iatrogenic injury, the first was in the sphenoid sinus. The second was following functional endoscopic sinus surgery (FESS). Fascia lata was used to repair all cases. Beriplast was used as sealing agent in four cases and clotted blood was used in remaining case. Despite the small number, CSF rhinor rhoea was resolved in all cases. The patients were followed up for 2.5 to 6.5 years.
Endoscopic repair is a viable option even in developing countries. It is cost effective and has a very low morbidity rate with no mortality at all.
Keywords: Cerebrospinal fluid leak, Endoscopic repair.
Introduction
The origin of cerebrospinal fluid (CSF) rhinorrhoea can be from anterior skull base defect or secondary to temporal bone fractures. Anterior skull base defect leading to CSF rhinorrhoea can be a serious problem; as it is difficult to diagnose and to treat. The etiology varies from trauma, iatrogenic injuries, congenital malformations, tumours or idiopathic.
The risk of meningitis from untreated CSF rhinorrhoea ranges from 10% annually1 upto 40% in long-term follow-up.2 For this, high rate of morbidity from ascending meningitis surgical repair is recommended in all cases. The approach can vary from intracranial approaches that was first described by Dandy in 1926.3 The morbidity of intracranial approaches may include haemorrhage, cerebral oedema, anosmia, memory deficit and osteomylilitis of bone flap.4 The success rate is 70 to 80% while 10% of patients have persistent leak after multiple intracranial treatments.5-7
Dohlman reported the first extra-cranial approach8 and Wigand in 1981 reported the first endoscopic repair of CSF fistula.9 A variety of techniques and materials have been first described for it. A Meta analysis showed a success rate of 90% in the first attempt and 97% overall10 with the endoscopic technique. The present study determines various causes and outcome of endoscopic repair of Cerebrospinal Fluid (CSF) leak in a developing country.
Case Series
This prospective descriptive study included patients with CSF rhinorrhoea managed by the Department of Otolaryngology and Neurosurgery in a tertiary care hospital from 2004 to 2009. Convenience sampling was used for late collection. A retrospective review of charts and follow up interviews were conducted for patients with CSF rhinorrhoea. Data collected included site of leak, surgical approach and any recurrence of leak. Data was analyzed with descriptive statistics.
Operative Technique:
All patients were evaluated using thin cut computer tomography (CT) Scan of Para nasal sinuses to identify the site of leak pre-operatively, except the two cases of iatrogenic CSF leaks in which site was already very evident. Patients were administered systemic antibiotics. A TV monitor and camera were attached to the endoscope for good visual control and for teaching purposes. Fascia Lata graft was harvested with antiseptic precautions before starting the nasal procedure.
The site was identified with the help of Rigid endoscope (Karl Storz - 0º, 30º & 70º) and fascia lata graft was plugged in the defect. Fluroescein was not used in any of the cases. Beriplast (CSL Behring GmbH, 35041 Marburg, Germany) or clotted blood (patient\\\'s own) was used in all the cases for sealing the graft. Lumbar drain was kept in place for all the cases postoperatively for at least 72 hours.
Results
Total of five patients were included in the study. The age of patients ranged from 8 to 65 years. Four patients were male and one female. Fluroescein was not used in any of the cases. In two patients, the defect could not be identified preoperatively but repair was done according to the site identified on CT scan (Table).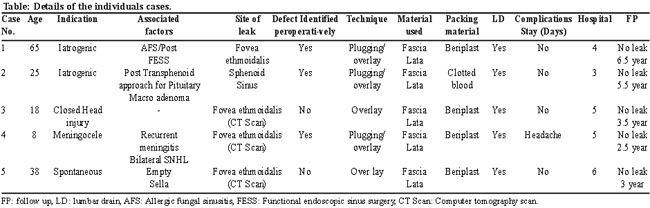
In the two cases of iatrogenic injury, the first was in the sphenoid sinus following trans- sphenoid sinus surgery for pituitary macro adenoma; making the site of leak quiet obvious. The second case was following FESS in the initial stages of developing the expertise for it, the primary surgeon did the repair and as he was well aware of the site of leak, a second CT scan was avoided to reduce the cost of surgery. There was one case each of closed head injury, meningocele and spontaneous cerebrospinal fluid rhinorrhoea.
Discussion
Endoscopic repair of CSF rhinorrhoea is now an established practice for most cases in the developed countries. This procedure is still in the evolving stages in the developing countries as the nasal endoscopic assisted surgeries are still relatively new. The surgeons are still developing expertise for this procedure. In our hospital, on an average 1293 patients get admitted in neurosurgery service from the emergency department. Ten patients who were diagnosed as having CSF rhinorrhoea underwent open technique repair in the last five years. During this same period five patients have been operated in our department with the endonasal endoscopic approach.
We had a diverse group of patients in our study with male female ratio of 4:1. Two patients had iatrogenic injuries of different nature of surgery. First was following functional endoscopic sinus surgery (FESS) for allergic fungal sinusitis and second was following trans sphenoid surgery for pituitary macro adenoma. One patient had persistent CSF leak following closed head injury after a road traffic accident. He was given a period of 6 weeks for spontaneous healing to which he did not respond. The youngest patient was an eight year old boy with history of recurrent meningitis secondary to a congenital meningocele. Whereas the only female was 38 years old tall, obese, with a history of headache and an associated empty sella. She had spontaneous CSF rhinorrhoea and high BMI which has been associated with spontaneous leaks in other studies.11
Four patients had their leaks identified in the area of fovea Ethmoidalis (Anterior Ethmoid cells) and one patient had a large defect in the sphenoid sinus following trans sphenoid resection of pituitary adenoma. In two patients, the defect could not be identified peroperatively even on doing Valsalva maneuver therefore the repair was done according to the site identified on CT scan.
Fluroescein has been used in other studies12 to identify the defect but it was not used in any of our patients. This was due to the concern that it is not an FDA approved drug for intrathecal injection. Fluroescein in some case has been found to cause convulsions, transient paresis and neuropathic pain though the frequency is sporadic. However, the reported incidence of complications is very low and seems to be related to the concentration of fluroescein used.13 Also it has a restricted availability and high cost of the drug in Pakistan.
The material used was fascia lata in all cases as it had adequate strength and a large graft can be taken to plug in the defects as much as desired. Gel foam and Beriplast was used as a packing material in all cases except one, due to the issue of financial constraints. In this case, clotted blood of same patient was used as packing to seal the graft area.
Lumbar drain was placed in all cases to decrease CSF pressure. There was no major complication in our study despite being a relatively new procedure. Only two reports of headache were encountered which resolved post operatively after removal of lumbar drain in one patient and the other took almost 2 months to resolve.
Despite the small number, the results were 100% resolution of CSR rhino rhoea. The patients were followed up from 2.5 to 6 years. We need to create better awareness and liaison with the neurosurgeons about this approach. Their confidence needs to be improved for this procedure as it has better results with minimum of complications. Another study by Mazhar Husain et al has reported a 88.8% success rate in a study of nine patients in the first attempt.14
The limitations of the study was the small number of the patients which is directly related to the awareness among the neurosurgeons for this procedure. The neurosurgeons are the people who are dealing with these patients primarily and a better referral base has to be created with them. The other limitation was the difficulty in identifying the site of leak preoperatively in two patients which is high for a small study. Fluroescein may help in better visualization in these cases.
Conclusion
Endoscopic repair is a viable option even in developing countries where the surgeons are still developing the expertise for this procedure. As it is cost effective and have a very low morbidity rate and no mortality, the neurosurgeons need to be taken into confidence; for this repair. Flourescien may help in better visualization of these defects and seems to be a safe option if concentration is kept low.
References
1. McMains KC, Gross CW, Kountakis SE. Endoscopic management of cerebrospinal fluid rhinorrhoea. Laryngoscope 2004; 114: 1833-7.
2. Park JI, StStrlzow VV, Friedman WH. Current management of cerebrospinal fluid rhinorrhoea. Laryngoscope 1983; 93: 1294-300.
3. Dandy WD. Pneumocephalus (intracranial pneumocele or aerocele). Arch Surg 1926; 12: 949-82.
4. McCormack B, Cooper PR, Persky M, Rothstein S. Extracranial repair of cerebrospinal fluid fistulas: technique and results in 37 patients. Neurosurgery 1990; 27: 412-7.
5. Schick B, Ibing R, Bros D,Draf W. Long-term study of endonasal duraplasty and review of the literature. Ann Otol Rhinol Laryngol 2001; 110: 142-7.
6. Lanza DC, O\\\'Brien DA, Kennedy DW. Endoscopic repair of cerebrospinal fluid fistulae nad encephaloceles. Laryngoscope 1996; 106: 1119-25.
7. Ray BS, Bergland RM. Cerebrospinal fluid fistulae: clinical aspects, techniques of localization and methods of closure. J Neurosurg 1969; 30: 399-405.
8. Dohlman G. Spontaneous cerebrospinal fluid rhinorrhoea. Acta Otolaryngol Suppl 1948; 67: 20-3.
9. Wigand ME. Transnasal ethmoidectomy under endoscopial control. Rhinology 1981; 19: 7-15.
10. Hegazy HM, Carrau RL, Synderman CH, Kassam A, Zweig J. Transnasal endoscopic repair of cerebrospinal fluid rhinorrhoea: a meta analysis. Laryngoscope 2000; 110: 1166-72.
11. Lindstrom DR, Toohill RJ, Loehrl TA, Smith TL. Management of cerebrospinal fluid rhinorrhoea: the Medical College of Wisconsin Experience. Laryngoscope 2004; 114: 969-74.
12. Tabee A, Placantonakis DG, Schwartz TH, Anand VK. Intrathecal fluorescein in endoscopic skull base surgery. Otolaryngology-Head and Neck Surgery 2007; 137: 316-20.
13. Keerl R, Weber RK, Draf W, Wienke A, Schaefer SD. Use of sodium fluorescein solution for detection of cerebrospinal fluid fistulas: an analysis of 420 adminstrations and reported complications in Europe and the United States. Laryngoscope 2004; 114: 266-72.
14. Husain M, Jha D, Vastsal DK, Husain N, Gupta RK. Neuroendoscopic Transnasal Repair of Cerebrospinal Fluid Rhinorrhoea. Skull Base 2003; 13: 73-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: