
Seema Lasi ( Human Development Programme, Aga Khan University, Karachi. )
Ghazala Rafique ( Human Development Programme, Aga Khan University, Karachi. )
Habib Peermohammad ( Human Development Programme, Aga Khan University, Karachi. )
September 2012, Volume 62, Issue 9
Original Article
Abstract
Objective: To determine the incidence, nature and the extent of infant injuries in two suburban and rural communities of Pakistan.
Methods: The cross-sectional study was conducted on a cohort of 310 infants in suburban and rural communities of Pakistan in September 2007. The information was collected from primary care-givers based on any injury that had occurred to their infants during the preceding 3 months that required treatment at home or in a hospital.
Result: The incidence of non-fatal injury for infants up to 1-year-old was found to be 19 injuries per 100 person (child) years of exposure (95% CI 9.90 - 27.21). In suburban area, the rate was 26 injuries /100 person (child) years (95 % CI 15.37 - 35.71), while in rural area, it was 13 injuries/100 person (child) years of exposure (95 % CI 4.79-18.39). Altogether, 13 episodes of injury were reported among infants in both the communities. The male to female infant ratio for injury was 1:2.2. Suburban area had more than double injuries compared to the rural area.
Conclusion: The magnitude of infant injuries was quite significant, especially among suburban and female children. There is a dire need to develop community-based interventions creating awareness on the matter.
Keywords: Infants, Injury, Non-fatal injuries. (JPMA 62: 910; 2012)
Introduction
Injuries during infancy are enormously underestimated due to high numbers of infectious and perinatal causes of illnesses and deaths. In fact, Low Middle Income Countries (LMIC) carried the highest burden of infant injuries among the under-5 age group, with 103 deaths per 100,000 children in 2004.1,2
During infancy, it is assumed that children are less mobile and live in a well-protected and controlled environment, close to the care-giver; hence, less likelihood of coming across any adverse outcomes. There is still high risk of injury to infants due to their lack of control, coordination and disproportionate body size.3 Consequently, these infants come across various life-threatening events. Most common injuries happening to infants are drowning, fall, burn, choking and smothering.2 Head injury is found to be the most common cause of death during infancy.4 Injury repercussions could be temporary as well as permanent. This includes, but is not limited to, physical, behavioural and cognitive impairments, delays or even disabilities which may have lifelong consequences.5,6 Major risk factors identified for childhood injury are exposure to hazardous environment, absence of adult supervision and lack of safe play areas.2
Global data on infant injury is very limited, especially in the developing countries.2 In Bangladesh, the leading cause of mortality during infancy is found to be smothering. Besides, drowning, burn and fall were also found to cause significant number of deaths.3 In Singapore, 405 cases of infant injury were reported from various healthcare facilities during a period of 6 months.7
Infant mortality rate in Pakistan is 78 per 1000 livebirths; major causes are neonatal and infectious diseases.8 Injury is emerging as a major cause of infant mortality and accounts for 16 per 1000 live births.
In Pakistan, population-based annual incidence rate of non-fatal injuries during 1990-94 was reported to be 14 per 1000 infants.9 Infant injuries were also reported to be the lowest among the under-5 group. Besides, childhood injury was also reported by a few studies in Karachi, but the burden due to infant injuries was not specifically provided.
Our study provides information on the magnitude, nature and causes of injury which are generally not available for the infant population in Pakistan. The basic premise of the study was to determine the community-based incidence of morbidity due to infant injuries in suburban and rural communities of Pakistan. Besides, it also identified the sources of injury and the healthcare seeking behaviour of the care-givers.
The data presented here is part of a larger cohort of 2865 children of 0-8 years of age. The findings of infants (up to 01 year olds) are reported here, and, because the pattern of injury epidemiology differs for infants,10 the rest of the age group (1+ to 8 years) is reported elsewhere.11
Patients and Methods
The study was undertaken in Tandojam district, Sindh, and in Mastung district, Balochistan. Tandojam is a suburban area about 20km from the main city of Hyderabad. Mastung is a rural area about 100km from the main city of Quetta, the provincial capital of Balochistan, and has a mountainous terrain.
The Aga Khan University-Human Development Programme (AKU-HDP) is running a community-based early childhood development (Cb ECD) programme in these two districts since 2005. The programme regularly monitors the growth and development and provides advice to primary care-givers for a cohort of children aged 0-8 years. The present information is based on a cross-sectional survey conducted in September 2007.
The survey was conducted on the entire sampling frame of 2865 children enrolled at the time in the ECD programme. The respondents were the children\\\'s primary care-givers, and information was collected retrospectively based on any injury that had happened to the infant during the preceding three months.12 A structured questionnaire was specifically developed for the purpose. The questionnaire was translated into the national language and then back-translated into English, and then pretested to assess and evaluate its effectiveness before administration in the field. Informed consent was taken from the care-givers with the assurance of complete confidentiality. Ethical approval for the study was obtained from the Ethical Review Committee of the Aga Khan University.
The number of infants identified from this cohort was 316. The data-collectors were Early Childhood Development Workers (ECDWs) involved in routine growth and development monitoring of these infants for another longitudinal project. One-day training was provided to these workers to develop an understanding of childhood injuries and comprehension of the questionnaire. For quality assurance of data, consistency checks on completeness and accuracy of the collected data was ensured by the field supervisors and data management staff.
After taking informed consent, the data was collected from 98% care-givers; the rest either refused or could not participate due to non-availability. The present analysis is based on a total sample size of 310 infants.
Data were double-entered using the Visual FoxPro software (version 6.0) and analysed using the SPSS software (version 13 and 16). To study the characteristics of the subjects, descriptive statistics were generated for the entire range of variables under study. Most variables were categorical for which proportions were reported, and means and standard deviations were calculated for continuous variables.
Results
The incidence of non-fatal injury for infants up to 1 year old was found to be 19 injuries/100 person (child) years of exposure (95% CI 9.90 - 27.21). In suburban area, it was 26 injuries/100 person (child) years (95 % CI 15.37 - 35.71), while in rural area, it was 13 injuries/100 person (child) years of exposure (95 % CI 4.79-18.39). Altogether, 13 episodes of injury were reported among infants in both the communities.
The suburban community had a population of 9770 with 652 households and 714 families spread over 6 villages. The mean monthly household income in suburban areas was Pak Rupees 11,323 (US $133) ± 9,835 and the mean monthly per capita income was Pak Rupees 2828 (US $33). Literacy among the population was 65%, but among the females it was only 39%.13
The rural area had a mountainous terrain with scattered population. According to the community census, the catchment population was 8354 with 504 households and 721 families in 11 villages. The mean monthly household income is Pak Rupees 9165 (US $108) ± 9356 and the mean monthly per capita income was Pak Rupees 1095 (US $13). Literacy among the population was 56%, but among the females it was only 38%.12
Altogether, 310 families were found to have children less than a year old, and were approached for data collection in both the communities [163 (52.6%) families in Tandojam, and 147 (47.4%) families in Mastung]. Male infants were 47% and the rest were female infants. The mean age of infants was 6.07 months and the mean number of siblings (up to 8 years old) in the families was 2.4 among the surveyed population of both the communities (Table-1).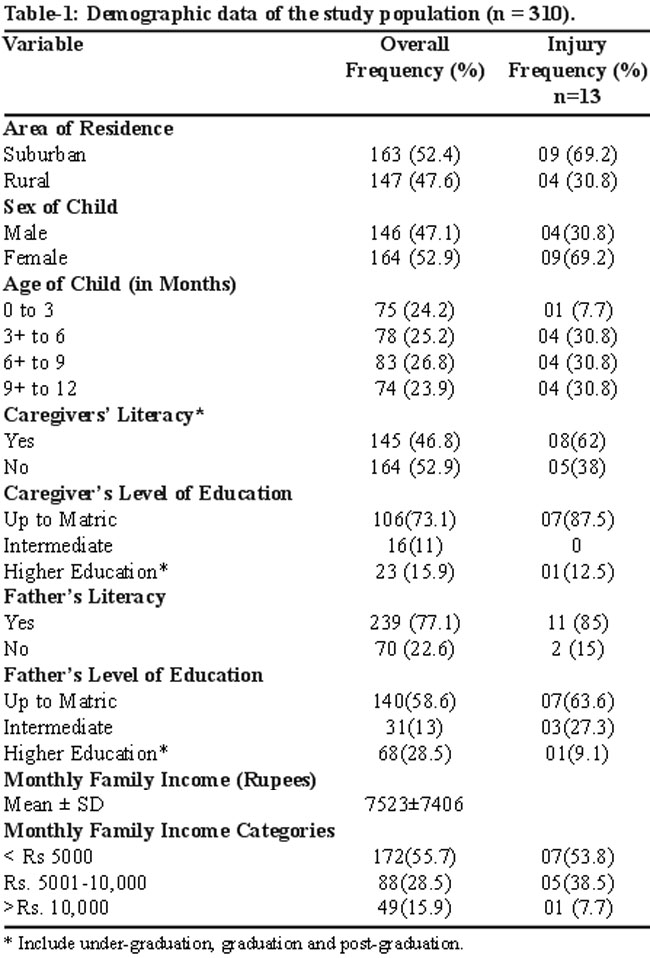
The male-to-female infant ratio for injuries was 1:2.2, that is, the female child was found to have more than double injuries (p = 0.179). Likewise, the suburban area also reported more than double the injuries compared to the rural area. However, the difference was statistically insignificant (p = 0.173).
For 0 to 3 months, the numbers of injuries were the lowest. From 3 months onwards; there was a tremendous increase in the rate of injury which stayed constant for all age categories up to 1 year.
Majority of fathers 301(97%) were engaged in some kind of occupation, whereas the remaining 9 (3%) were unemployed, retired or studying. Similarly, 24 (7.7%) care-givers were engaged in some kind of earning activities; the majority being either teachers or tailors. Injury happening to infants of earning mothers was not found to be significantly different from non earning mothers.
There were significantly more literate mothers in the suburban area as compared to the rural area (p = < 0.05). No significant difference was found for injuries among infants of literate and illiterate mothers. However, a trend was seen among the literate mothers, with the majority of injuries happening to infants of mothers whose educational qualification was below the tenth grade. The same was true for father\\\'s literacy status. There were more literate fathers in suburban as compared to rural (p = <0.05) areas, and the same increasing trend for occurrence of injury was observed.
The mean monthly family income was found to be Rs. 7523 ± 7406. A trend for infant injuries was seen with family income — more injuries happening to families in the low-income category (< Rs. 5000). However, the difference was not statistically significant.
Twelve (92%) of the 13 events of injuries took place inside the home and the most frequent area of occurrence was found to be the courtyard and the bedroom (Table-2).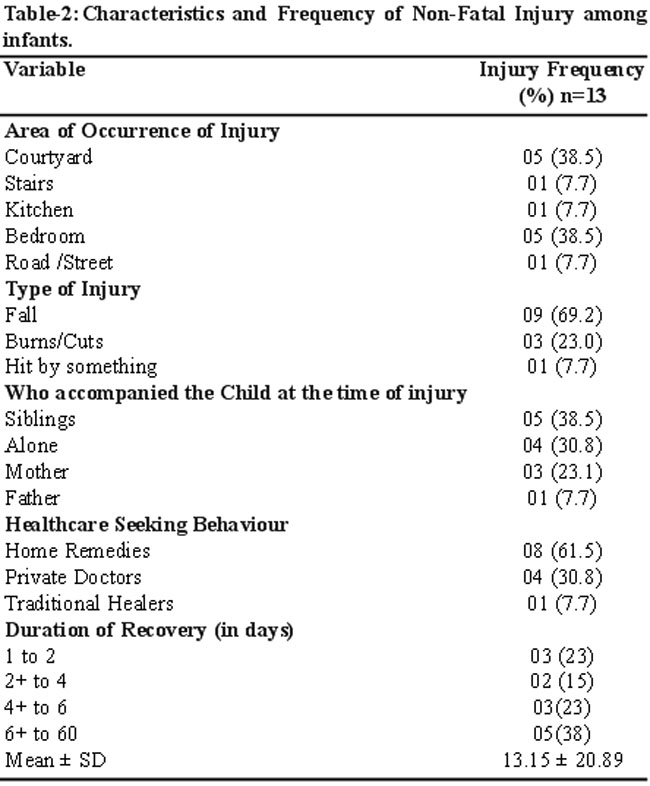
For type of injury, fall14 (77%) rated the highest, followed by cuts and burns (23%). For child supervision at the time of injury, 214 (69.3%) children were either found to be alone or with siblings less than 15 years of age.
For care-givers\\\' healthcare-seeking behaviour, no infant was taken to a government facility, 04 (30.8%) went to private clinics, and 01 (7.7%) visited a traditional healer; the rest were treated at home. Two infants felt unconscious right after the occurrence of injury, but were not taken to any healthcare facility. The analysis showed that for every three infants injured, only 1 infant (approximately) was taken to a healthcare facility.
The average days of recovery was found to be approximately 13 days ± 20.8 with 1 day as minimum and 60 days as the maximum.
Ninety percent of the fall injury involved either the head or the face, including the neck (Figure-1).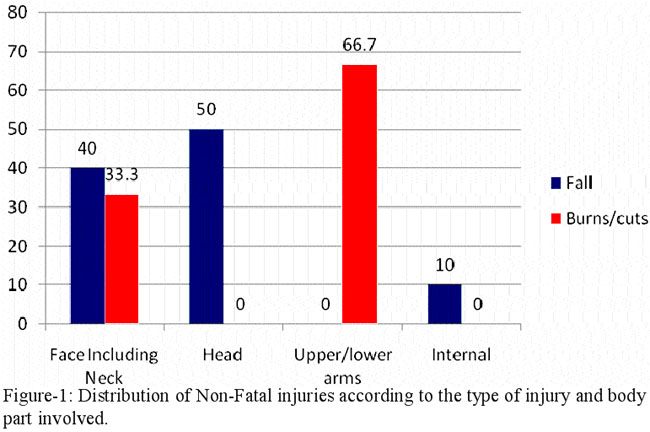

This was followed by burns and cuts involving the face and the neck (33.3%) and injuries to upper/lower arm (66.7%).
The most commonly involved body part for injury among female infants was the head (n=05; 38.4%) and the face, including the neck, (n=4; 30.7%). The girls outnumbered injuries as compared to the boys, and among infant girls, head injuries were found to be the highest among the group.
Discussion
In literature only a few studies were found with respect to injuries among infants. For the first time in Pakistan, the current study provides an exclusive snapshot of the highly-neglected area of infant injuries. The magnitude of non-fatal infant injuries is quite considerable in both the communities. Compared with the National Health Survey of Pakistan (NHSP), the incidence rate is more than 11 times higher. The reason for this high rate of injury could be that the NHSP only considered events which required expert attention. In our study, the majority of injuries were head-related. Even then a high number of injuries were treated at home. This was the main reason for not considering injury requiring healthcare referral only, as there is ample evidence, especially in developing countries, that the severity of injuries is not the only factor which decides healthcare-seeking behaviour of care-givers. There are factors such as the awareness level of care-givers, cultural and financial constraints involved which may discourage families from seeking expert advice. The fact was also observed during the current study where two infants fell unconscious after a fall, but were not taken to any healthcare provider. According to the Center of Disease Control and Prevention (CDC), an infant becoming unconscious even for less than a minute after injury may be in very critical condition. The reasons for not seeking healthcare were not explored and could be an interesting research question to explore in future.
Another study reporting non-fatal childhood injuries during early years (1+ to 8 years) found a similar incidence rate; the only difference was that injuries requiring expert attention were considered.11 In Singapore also, a significant number of infant injuries were reported to healthcare facilities.7 The preceding comparative account clearly interprets that infant injuries are not any less than the injuries happening to the rest of the early childhood period.
In terms of the present study there seems to be an underreporting as only two types of injury — fall and burns/cuts — were reported by the care-givers. The study, as such, was unable to capture incidence of drowning, smothering, poisoning, choking and other forms of infant injuries. Among fall and burns/cut, there was a high incidence of fall. The same trend was also observed by other research studies.7,11,15
Rural infants as well as the girl child were found to be more at risk. Generally, injury is more common among the boys, but for infants the reverse seems to be true. A trend for infant injuries was seen for family income, with more injuries happening to families in the low-income category (< Rs. 5000). Research studies from Pakistan9 and rural Vietnam16 also show similar findings with more injuries happening to children from poor households.
The findings of the present study also underscore the need for full-time supervision of infants by an adult. A study in Jordan identified the presence of an adult to be a significant factor to reduce the occurrence of injuries, especially in early and middle childhood.17 Supervision by an adult is an important factor, but an overall safe environment cannot be ignored as a key factor in reducing the number of childhood injuries.
The occurrence of injury predominantly took place either in the courtyard or the bedroom. In most rural and suburban households, most of the activities take place in the courtyard and this is the place where infants spend most of their time when not sleeping. The study carried out in Singapore also identified bedroom as the most frequent place for majority of injury occurrences.7
Road traffic injury, though rare in the present study, shall not be underestimated. Of special concern is the mode in which these infants are seen accompanying their care-givers on the roads without any safety gear. A study to measure the burden of morbidity and mortality is very much in need to assess the current burden of road traffic injuries among infants. Such a study would also help to set safety regulations to protect these infants against road traffic injuries.
The study clearly points out the places where the majority of injuries occurred. This is another indication of inadequate safety measures of child-proofing in these households.
The small sample size was an important limitation of the study. To draw meaningful inferences, large sample sizes are required and due to this very reason the associations between many variables were found to be insignificant. As this study was carried out in rural and suburban communities only, the findings cannot be generalised over urban populations.
In a study reporting childhood injuries,11 reporting only on injuries that sought medical care was identified as a limitation. This study has tried to overcome this limitation by considering all injuries irrespective of their healthcare-seeking behaviour. In this way, underestimation has been taken care of in one way. However, keeping in view the limited type of injuries that were reported by the care-givers, underestimation of injuries cannot be completely ruled out. Another way to control underestimation, keeping in view the very different nature of infant injuries, is to develop validated tools/questionnaires which can capture infant injuries to its entirety. Under-reporting due to recall bias is another possibility for under-estimation due to the retrospective nature of data collection. However, this is inherent in all community-based surveys.18
Conclusion
With the possibilities of underestimation, the study reports that infant injury is a far more significant problem than reported by earlier studies and there is a dire need to look into ways to minimize the numbers. An active surveillance system to monitor injuries is highly recommended to obtain a further understanding of infant injuries and to guide the development of interventions accordingly. An important area for future research would be to assess the potential causes of infant injury. Viewing the current magnitude of infant injury, it is imperative to develop interventions to reduce its incidence. An important component of this intervention should be to educate families, especially primary care-givers, about the consequences of injuries and the preventive measures to mitigate the risk of injuries. The interventions should be directed towards three Es; education, enforcement and engineering.
Acknowledgement
We acknowledge the funding by the Royal Netherlands Embassy for the Releasing Confidence and Creativity (RCC) project under the umbrella of the Aga Khan Foundation, Pakistan. We are also thankful to Mr. Iqbal Azam, Assistant Professor of Statistics, Aga Khan University, for his input in statistical analysis and valuable comments.
References
1. Linnan M, Giersing M, Linnan H, Cox R, Williams M, Voumard C, Hatfield R. Child mortality and injury in Asia: policy and programme implications. Florence, UNICEF Innocenti Research Centre; 2007.
2. Peden M, Oyebite K, Ozanne-Smith J. World report on child injury prevention: World Health Organization; 2008.
3. Linnan, Michael, et al. \\\'Child Mortality and Injury in Asia: An overview\\\', Innocenti Working Paper 2007-04, Special Series on Child Injury No. 1. Florence, UNICEF Innocenti Research Centre, 2007.
4. Billmire M, Myers P. Serious head injury in infants: accident or abuse? Pediatrics 1985; 75: 340-2.
5. Polinder S, Meerding W, Toet H, Mulder S, Essink-Bot M, van Beeck EF. Prevalence and prognostic factors of disability after childhood injury. Pediatrics 2005; 116: e810-7.
6. Rivara FP. Developmental and behavioral issues in childhood injury prevention. J Dev Behav Pediatr 1995; 16: 362-70.
7. Snodgrass AM, Ang A. Unintentional injuries in infants in Singapore. Singapore Med J 2006; 47: 376-82.
8. National Institute of Population Studies (NIPS) [Pakistan], and Macro International Inc. Pakistan Demographic and Health Survey 2006-07. Islamabad, Pakistan: National Institute of Population Studies and Macro International Inc; 2008.
9. Fatmi Z, Kazi A, Hadden WC, Bhutta ZA, Razzak JA, Pappas G. Incidence and pattern of unintentional injuries and resulting disability among children under 5 years of age: results of the National Health Survey of Pakistan. Paediatr Perinat Epidemiol 2009; 23: 229-38.
10. Linnan M. Child mortality and injury in Asia: survey results and evidence. Innocenti Working Papers; 2007.
11. Lasi S, Rafique G, Peermohamed H. Childhood injuries in Pakistan: results from two communities. J Health Popul Nutr 2010; 28: 392-8.
12. Sethi D, Habibula S, McGee K, Peden M, Bennett S, Hyder AA, et al. Guidelines for conducting community surveys on injuries and violence. Geneva: World Health Organization, 2004; 150.
13. Census Report. Aga Khan University - Human Development Programme: Pakistan; 2008.
14. Christoffel K, Scheidt PC, Agran PF, Kraus JF, McLoughlin E, Paulson JA. Standard definitions for childhood injury research: excerpts of a conference report. Pediatrics 1992; 89: 1027-34.
15. Linnan M, Giersing M, Cox R, Linnan H, Williams MK, Voumard C, et al. Child mortality and injury in Asia: an overview. Florence: UNICEF Innocenti Research Center; 2007; 26.
16. Thanh NX, Hang HM, Chuc NTK, Byass P, Lindholm L. Does poverty lead to non-fatal unintentional injuries in rural Vietnam? International Journal of Injury Control and Safety Promotion 2005; 12: 31-7.
17. Janson S, Aleco M, Beetar A, Bodin A, Shami S. Accident risks for suburban preschool Jordanian children. J Trop Pediatr 1994; 40: 88-93.
18. Sethi D, Habibula S, McGee K, Peden M, Bennett S, Hyder AA, et al. Guidelines for conducting community surveys on injuries and violence. Geneva: World Health Organization 2004; 150.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: